Purpose
To report the clinical outcomes of lamellar keratoplasty (LKP) in patients with delayed-onset mustard gas keratitis and to compare visual acuity and graft survival rates between subgroups with simultaneous or sequential keratolimbal allograft and LKP.
Design
Retrospective, comparative, interventional case series.
Methods
Fifty-two eyes of 37 male survivors of chemical warfare with mustard gas keratitis who underwent LKP were included. The results were evaluated with respect to best spectacle-corrected visual acuity (BSCVA), refractive error and keratometry readings, and graft clarity. Thirty-two eyes required stem cell transplantation (keratolimbal allograft), which was performed before or concomitant with LKP. The groups with sequential and concomitant intervention were compared regarding BSCVA, refraction, corneal graft surface stability, and stem cell and corneal graft survival rates.
Results
The mean patient age at the time of surgery was 43.4 ± 8.2 years, and the mean follow-up period was 41.4 ± 19.6 months. The mean preoperative BSCVA was 0.51 ± 0.48 logarithm of the minimal angle of resolution units, which increased to 0.33 ± 0.18 logarithm of the minimal angle of resolution units ( P = .03). The mean preoperative spherical equivalent refractive error was −2.40 ± 1.5 diopters, which remained unchanged after surgery (−1.52 ± 3.7 diopters; P = .77). No significant difference between the sequential and simultaneous subgroups was found with regard to postoperative BSCVA, refraction, keratometry readings, or corneal graft survival (90.3% and 89.9%, respectively; P = .68). However, the latter group had statistically better stem cell graft survival (40.0% vs 100% at month 41, respectively; P = .02).
Conclusions
LKP is an effective method of corneal transplantation in mustard gas victims. When stem cell and corneal transplantation are indicated, the simultaneous approach can yield better results than staged intervention.
Mustard gas is a lipophilic, highly cytotoxic agent that rapidly penetrates the tissue, and the eye is one of the organs typically most affected. Late complications, developing after 1 to 40 years, can cause progressive and permanent reduction in visual acuity in approximately 0.5% of severely wounded patients. The wide range of late ocular involvements reported includes chronic blepharitis, decreased tear meniscus, conjunctival vessel tortuosity, limbal ischemia and limbal stem cell deficiency, corneal scarring and neovascularization, corneal thinning, and lipid or amyloid deposits.
Penetrating keratoplasty is an established acceptable intervention for corneal involvement in mustard gas keratitis, but in cases with severe ocular involvement, a high rate of graft failure resulting from rejection reactions or opacity has been noted. Additionally, most cases of corneal involvement are limited to the anterior stroma, leaving the posterior stroma and endothelium relatively intact. Therefore, conventional lamellar keratoplasty can be considered as an alternative to full-thickness penetrating keratoplasty in mustard gas keratitis.
When significant limbal ischemia, stem cell deficiency, or both develop, stem cell transplantation is required to provide a viable source of corneal epithelial cells as well as to address conjunctival ischemia and scleral and peripheral corneal thinning. Because the involvement is bilateral in nearly all patients, transplantation of allogenic stem cells harvested from a living related donor (living-related conjunctival limbal allograft) or a cadaveric eye (keratolimbal allograft) should be performed. The outcomes of living-related conjunctival limbal allograft in these cases have been found to be acceptable. However, keratolimbal allograft provides more stem cells and simultaneously can address scleral and peripheral corneal involvement. In certain cases, limbal stem cell deficiency coincides with corneal involvement, necessitating both stem cell and corneal transplantation in individual patients.
The main objective of the present study was to report the outcomes of lamellar keratoplasty, alone or in combination with keratolimbal allograft, for the management of corneal involvement, limbal stem cell deficiency, or both in delayed mustard gas keratitis as well as to compare the 2 subgroups, which received sequential or simultaneous stem cell and corneal transplantations.
Methods
In this retrospective, comparative, interventional case series, a group of chemical warfare victims who were injured in the Iraq–Iran war (between 1980 and 1988) is presented. The patients had evidence of mustard gas-related keratitis, with conjunctival or corneal involvement (including corneal neovascularization and scarring, stromal thinning, and intrastromal lipid or amyloid deposits with or without limbal ischemia and stem cell deficiency). The corneal involvement was severe enough to necessitate lamellar keratoplasty in all participants, and keratolimbal allograft was performed in a subgroup of patients with clinical or laboratory signs, or both, of limbal stem cell deficiency.
The medical records of the patients were reviewed to gather data, including sex, age, type of symptoms, preoperative best spectacle-corrected visual acuity (BSCVA), corneal signs justifying corneal transplantation, follow-up duration, number of immune rejection reactions, graft clarity, complications, and final postoperative BSCVA. At the first presentation, a complete ophthalmologic evaluation consisting of BSCVA, slit-lamp biomicroscopy with special attention to tear meniscus and ocular surface status, intraocular pressure, and dilated funduscopy was performed. Thereafter, slit-lamp biomicroscopic examinations and intraocular pressure measurements were repeated at regular intervals, usually every 3 to 4 months. All procedures were performed by the 2 authors (M.A.J., M.R.J.) using the same surgical techniques.
Surgical Interventions
Lamellar keratoplasty
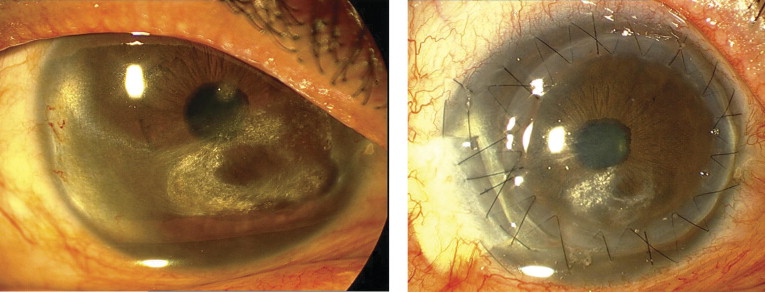
Indications for lamellar keratoplasty were corneal haziness leading to decreased visual acuity, photophobia, discomfort caused by corneal surface irregularity, abnormal deposits or severe thinning threatening globe integrity, or a combination thereof ( Figure 1 , Left). A Barron-Hessburg suction trephine with a diameter of 7.0 to 8.0 mm (based on the vertical corneal diameter and the extent of corneal involvement) was used to trephine at least 50% of the corneal thickness, and manual lamellar dissection was performed using a crescent blade (Alcon Laboratories, Fort Worth, Texas, USA). During lamellar dissection, an attempt was made to remove all scars and deposits, which chiefly were confined to the anterior and mid stroma, and to create a single-plane, smooth, and clear recipient bed ( Figure 1 , Right). A partial-thickness donated cornea, prepared from a fresh whole globe with an intact epithelium and oversized by 0.5 mm, was sutured into the recipient bed using 10-0 nylon sutures (Sharpoint; Angiotech, Vancouver, Canada). In most cases, temporary or permanent lateral tarsorrhaphy, punctal occlusion, or both were performed on conclusion of the operation.
In 3 eyes, deep anterior lamellar keratoplasty was attempted using the Anwar big-bubble technique. However, the procedure very soon was abandoned because it was not possible to achieve a successful big bubble even after several intrastromal air injections.
Stem cell transplantation
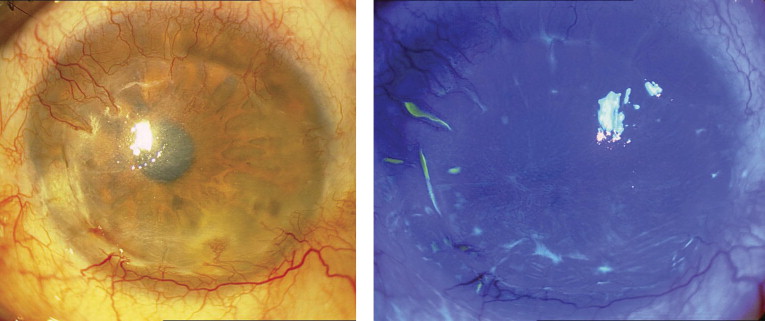
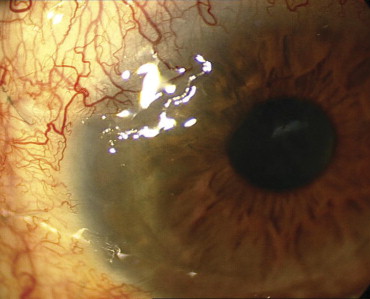
Limbal stem cell deficiency was diagnosed clinically as shown by limbal ischemia, loss of limbal palisades of Vogt, corneal surface irregularities, superficial vascularization ( Figure 2 , Left), and late corneal staining with fluorescein ( Figure 2 , Right) and was confirmed in 11 eyes using impression cytologic analysis. Limbal stem transplants, which were segmental in all cases, were harvested from cadaveric eyes (keratolimbal allograft) without human leukocyte antigen matching.
To prepare the recipient bed, involved limbal areas adjacent to the epithelial defects or thin cornea were chosen, and local peritomy, shaving, and mild cauterization of the sclera were performed. This was followed by half-thickness rectangular corneoscleral removal with an attempt to dissect all ischemic limbal areas as well as peripheral thin and opaque corneas up to the paracentral areas, if necessary. A corneoscleral block exactly matching the shape of the recipient bed and containing conjunctiva was prepared from a cadaveric eye and was sutured to the bed with interrupted 10-0 nylon sutures (Sharpoint; Figure 1 , Right).
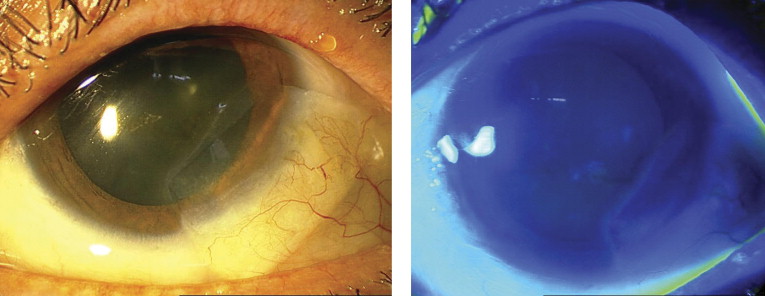
When indicated, both types of transplantation were performed either sequentially or simultaneously. Initially, a staged approach, in which keratolimbal allograft was performed first ( Figure 3 , Left) and then followed by lamellar keratoplasty after a few months, was carried out. Additionally, in some cases, limbal stem cell deficiency did not coincide with severe corneal opacities necessitating lamellar keratoplasty at the time. In these eyes, lamellar keratoplasty was performed after keratolimbal allograft when corneal involvements became severe enough to justify corneal transplantation. After a while, however, the technique evolved to a simultaneous approach in which the recipient was prepared for both transplantations harvested from a single cadaveric eye ( Figure 1 , Right).
Postoperative course
In all cases, topical eye drops, including chloramphenicol 0.5% every 6 hours, betamethasone 0.1% every 6 hours, preservative-free artificial tears every 2 hours, and lubricants every 8 hours, as well as systemic prednisolone 1 mg/kg daily, were started after surgery. The topical antibiotic was discontinued after complete reepithelialization, and systemic and topical corticosteroids were tapered off and discontinued over 2 to 4 weeks and 2 to 3 months, respectively, according to the severity of the ocular inflammation.
For patients who underwent keratolimbal allograft, oral cyclosporine A (Sandimmune; Novartis Pharma, Tokyo, Japan) 5 mg/kg daily, which was decreased to 3 mg/kg daily after a few weeks, and mycophenolate mofetil (CellCept; Hoffmann La Roche, Nutley, New Jersey, USA) 1 g twice daily were started at the time of surgery and were continued for at least 6 months. Afterward, the systemic immunosuppressive medications gradually were tapered off and discontinued after 1.5 to 2 years according to the condition of the patients. Cell blood counts, blood pressure, and renal and liver function tests were monitored at appropriate intervals in collaboration with a kidney transplant expert to monitor for possible complications of immunosuppressive therapy.
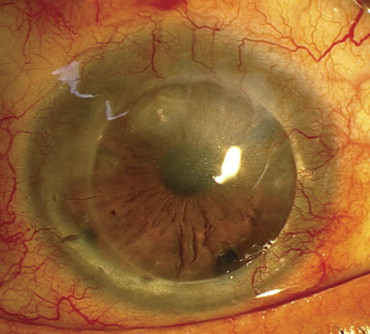
An episode of corneal graft rejection was defined as subepithelial or stromal infiltration in the corneal grafts. Corneal graft failure was diagnosed when the central portion of the graft became significantly opaque because of scarring, with or without vascularization (limbal stem cell deficiency or corneal ulcer). The presence of significant interface haziness involving the visual axis also was considered to be a failure ( Figure 4 ) . In eyes that underwent stem cell transplantation, acute stem cell graft rejection was diagnosed by limbal and perilimbal vascular engorgement, conjunctival chemosis in the transplant areas, or both ( Figure 5 ) . Stem cell transplantation failure was diagnosed in cases with progressive corneal vascularization or persistent epithelial defects (more than 2 weeks) adjacent to the graft. Acute rejection episodes of both corneal and stem cell transplantations were treated by increasing the dose and frequency of topical or systemic steroids, or both.
Statistical Analysis
General data such as age, BSCVA, and duration of follow-up (starting from stem cell or corneal transplantation, or both) were expressed as mean ± standard deviation using SPSS software version 15 (SPSS, Inc, Chicago, Illinois, USA). Preoperative and postoperative BSCVA and spherical equivalent refractive error were compared using the paired t test for normally distributed data and the Wilcoxon test for nonnormally distributed data. The Student t test, Mann–Whitney U test, and Fisher exact test were used to compare normally and nonnormally distributed as well as categorical data, respectively, between subgroups with sequential and simultaneous interventions. Kaplan-Meier survival curves and log-rank tests were used to evaluate and compare the cumulative incidence of corneal and stem cell graft survival between the 2 intervention subcategories. A P value of less than .05 was considered statistically significant.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


