 Questions
Questions
1. Which is the correct order of the five layers of Bruch’s membrane (from retina toward sclera)?
a. Retinal pigment epithelium (RPE) basement membrane, inner collagenous zone, elastic layer, outer collagenous zone, and choriocapillaris basement membrane.
b. RPE basement membrane, elastic layer, inner collagenous zone, outer collagenous zone, and choriocapillaris basement membrane.
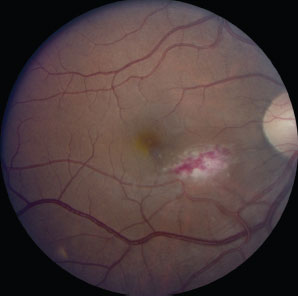
c. Elastic layer, RPE basement membrane, inner collagenous zone, outer collagenous zone, and choriocapillaris basement membrane.
d. Inner collagenous zone, elastic layer, outer collagenous zone, RPE basement membrane, and choriocapillaris basement membrane.
2. Which of the following statements regarding the vitreous is true?
a. The vitreous occupies approximately 50% of the entire eye volume and is primarily composed of water.
b. The vitreous is most firmly attached to the optic nerve, but is also attached to the vitreous base, the macula, and retinal vessels.
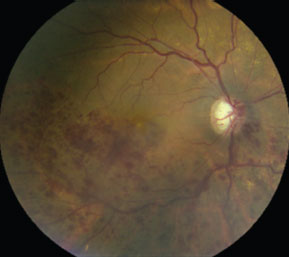
c. Vitreomacular traction syndrome generally results only after a complete posterior vitreous detachment.
d. The vitreous is composed of collagen and hyaluronate, which binds to water.
3. Which of the following statements regarding the neurosensory retinal anatomy is correct?
a. The internal limiting membrane is formed by the footplates of Müller’s cells.
b. The retinal vascular system generally supplies half of the oxygen used by the fundus.
c. Retinal photoreceptors generally synapse with bipolar cells, which then generally synapse with Müller’s cells.
d. The macula, as defined histologically, contains photoreceptors with two or more layers.
4. Which of the following patients should generally be considered for focal laser treatment of central serous chorioretinopathy (CSR)?
a. A patient with pigment epithelial detachment and surrounding sensory retinal detachment lasting for 3 weeks.
b. A retinal surgeon with a subfoveal lesion.
c. A patient whose prior episodes of CSR have been associated with permanently decreased acuity.
d. A patient with a history of bilateral CSR.
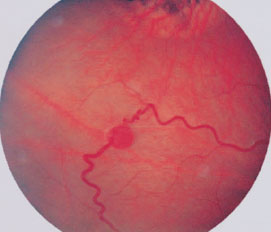
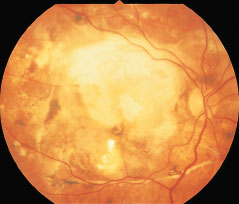
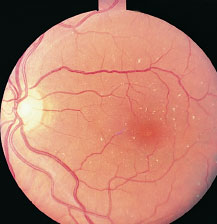
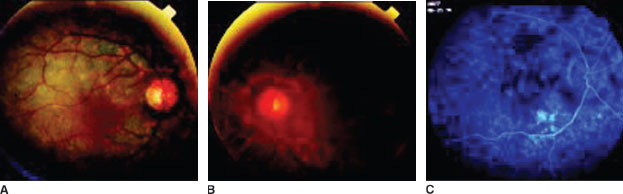
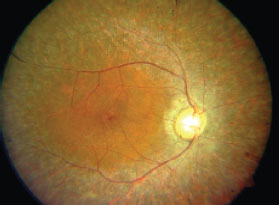
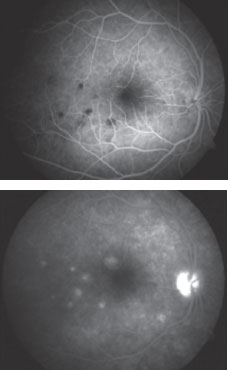
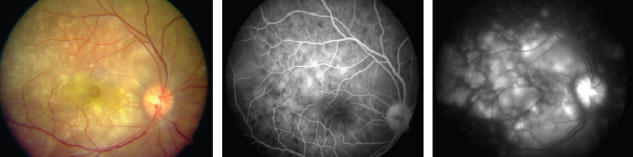
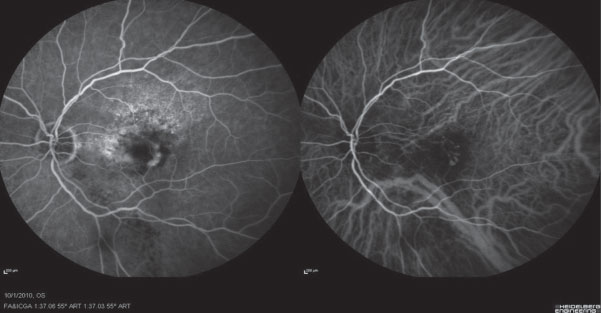
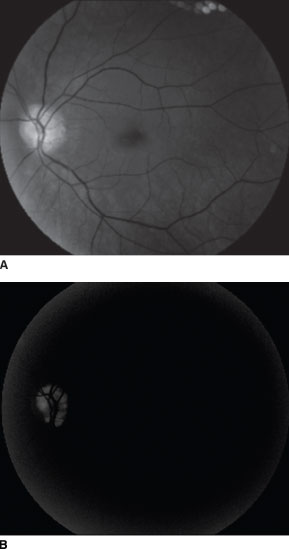
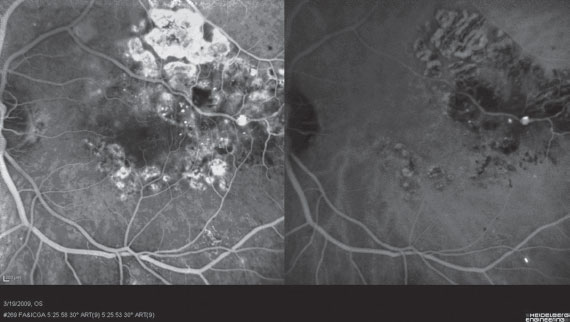
5. Systemic findings in a patient with the retinal pathology in the image below may include all of the following except
a. Café-au-lait spots.
b. Pancreatic and renal cysts.
c. Hemangioblastomas of the brainstem.
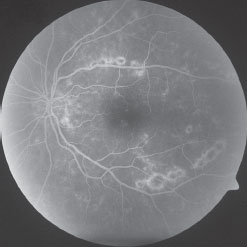
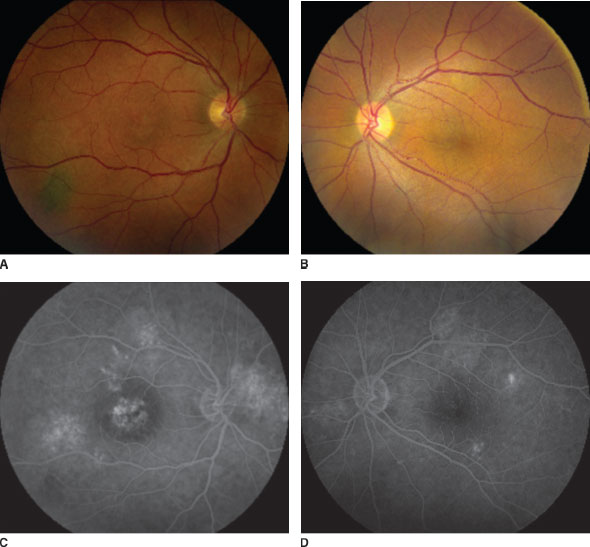
d. Pheochromocytoma.
6. Which one of the following concerning aphakic or pseudophakic cystoid macular edema (CME) is false?
a. The incidence of CME is lower with extracapsular surgery compared with intracapsular surgery.
b. Intraocular lens implantation decreases the incidence of CME following cataract surgery.
c. More than 75% of mild cases demonstrate regression within 6 months.
d. Topical nonsteroidal anti-inflammatory medications have been shown to reduce the incidence as well as to improve vision in CME following cataract surgery.
7. Which of the following statements regarding Eales’ disease is true?
a. It is primarily a disease of childhood and young adulthood, more commonly affecting girls.
b. It can be associated with tuberculosis, epistaxis, and cerebral vasculitis.
c. It is generally bilateral.
d. It generally affects males from the Middle East.
8. Which of the following statements regarding optical coherence tomography (OCT) is false?
a. Obtaining retinal OCT images is generally not possible in eyes with dense vitreous hemorrhage because the light is unable to penetrate through the hemorrhage.
b. Current OCT machines offer much better resolution than ultrasound.
c. Fourier-domain OCT offers the ability for registration in order to measure changes in macular volume in the same patient during subsequent patient visits.
d. Fourier-domain OCT offers better resolution images although they generally take longer to obtain than time-domain OCT.
9. Which of the following molecules is generally defective in Stargardt’s disease?
a. All-trans retinol.
b. ATP-binding cassette transporter of the retina.
c. 11-trans-retinaldehyde.
d. Rhodopsin.
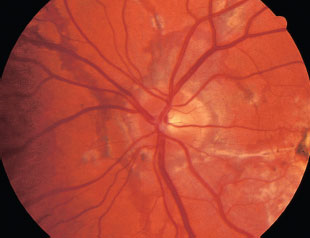
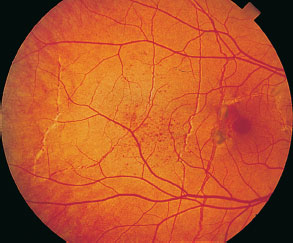
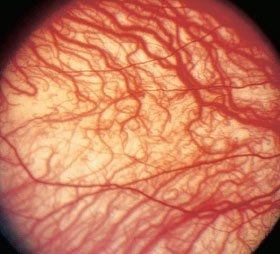
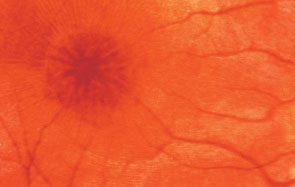
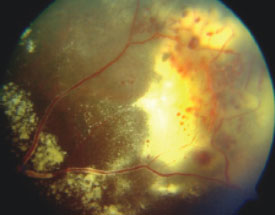
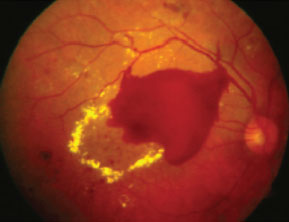
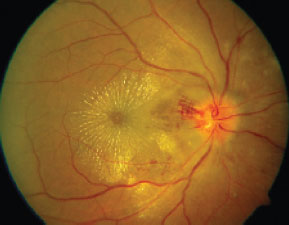
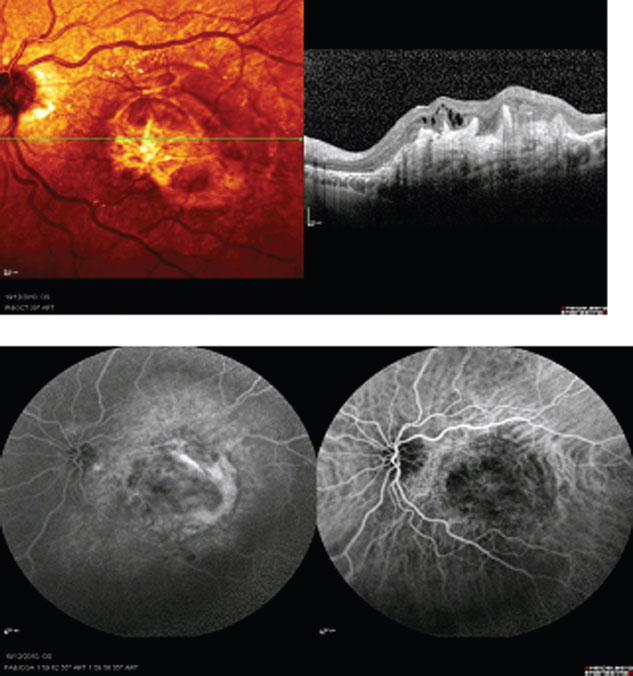
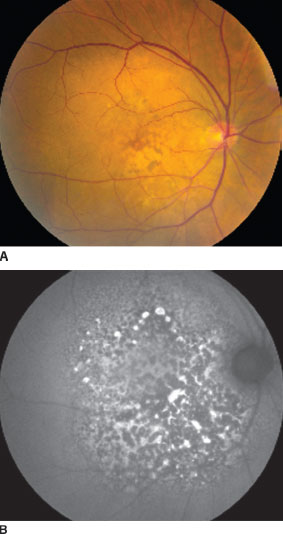
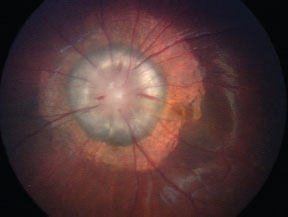
10. The pathology demonstrated in the image below anatomically represent breaks within
a. The RPE.
b. Bruch’s membrane.
c. Retinal photoreceptors.
d. Outer plexiform layer.
11. All of the following statements are true, except
a. Nanophthalmos typically is characterized by thickened sclera that can impede outflow leading to uveal effusion syndrome.
b. The choroid has the highest blood flow of any tissue in the human body.
c. The vortex veins drain into the central retinal vein.
d. The retinal pigment epithelium helps form the blood–ocular barrier.
12. All of the following statements regarding potential adverse effects from fluorescein angiography are true, except
a. Anaphylaxis can occur after fluorescein angiography, but is rare and occurs at the rate of <1 in 100,000 injections.
b. Urinary discoloration from fluorescein angiography occurs in <1% of patients.
c. Vasovagal reactions and nausea occur in approximately 10% of injections.
d. Premedication with antihistamines such as diphenhydramine can reduce the risk of developing an urticarial reaction from sodium fluorescein injection.
13. Which of the following concerning blood pressure–induced choroidal disease is false?
a. Critical pathophysiologic events lead to occlusion of the choriocapillaris.
b. Elschnig spots are characteristic.
c. Exudative retinal detachment may develop as a secondary manifestation.
d. Hypertensive choroidopathy may be associated with chronic elevation in systemic blood pressure.
14. What is the prevalence of endophthalmitis after an intravitreal triamcinolone injection?
a. 0%
b. 0.01% to 0.05%
c. 0.1% to 0.3%
d. 0.5% to 1.5%
15. Histopathologic features seen in the retinal vasculature of patients with early diabetic retinopathy include all of the following, except
a. Loss of arteriolar pericytes.
b. Thickening of endothelial basement membranes.
c. Capillary closure and/or nonperfusion.
d. Medial hyperplasia.
16. Fundus autofluorescence helps evaluate the function of which of the following structures within the eye?
a. Retinal pigment epithelium.
b. Bipolar cells.
c. Ganglion cells.
d. Retinal photoreceptors.
17. Which of the following regarding diabetic retinopathy is true?
a. Visual prognosis is generally better in patients with diffuse macular edema than in those with focal macular edema.
b. One of the definitions of clinically signifi-cant macular edema (CSME) from the Early Treatment for Diabetic Retinopathy Study (ETDRS) is the presence of any thickening >500 mm within the macula.
c. Intraretinal microvascular abnormalities often lead to retinal neovascularization.
d. Rhegmatogenous retinal detachment (of any type) is uncommon in proliferative diabetic retinopathy.
18. Which factor is most strongly correlated with the development of choroidal effusion following panretinal photocoagulation?
a. Systemic hypertension.
b. Increasing age.
c. Total retinal surface area treated.
d. Short axial length (<23 mm).
19. Each of the following is a valid conclusion of the Diabetes Control and Complications Trial (DCCT), except
a. Among type 1 diabetics with no retinopathy, intensive treatment can lower the incidence of progressive retinopathy by a factor of five compared with conventional treatment.
b. Patients with macular edema realize the benefits of intensive control sooner than patients with proliferative retinopathy.
c. The early worsening seen in patients initiating intensive control has no long-term effect on severity of retinopathy, and the benefit of intensive control is not seen for the first 3 to 5 years of treatment.
d. The study only tested type 1 diabetics and the conclusions reached may not necessarily apply to type 2 diabetics.
20. All of the following are generally unfavorable clinical prognostic features for visual stabilization following laser treatment of diabetic macular edema, except
a. Macular nonperfusion.
b. Cystoid macular edema.
c. Extensive hard exudation within the fovea.
d. Focal leakage and thickening.
21. Which one of the following characteristics is felt to confer the greatest protection from the development of proliferative diabetic retinopathy?
a. Complete posterior vitreous detachment (PVD).
b. Younger age (<30 years).
c. Ipsilateral carotid artery stenosis.
d. No history of hypertension.
22. Which of the following statements regarding diabetic retinopathy is true?
a. The ETDRS showed that focal laser treatment of clinically significant diabetic macular edema leads to an improvement in vision in twice as many treated patients as untreated patients.
b. The Diabetic Retinopathy Study (DRS) showed that panretinal photocoagulation (PRP) could reduce the incidence of severe visual loss in certain patients by 50%.
c. One definition of high-risk proliferative diabetic retinopathy mandating immediate PRP neovascularization is optic disc neovascularization covering greater than half of its area (greater than standard photograph 10A), only if associated with vitreous hemorrhage.
d. One definition of high-risk proliferative diabetic retinopathy is moderate to severe neovas-cularization elsewhere, only if associated with vitreous hemorrhage.
23. When performed properly, which of the following is not a potential adverse effect of panretinal photocoagulation?
a. Decreased night vision.
b. Angle-closure glaucoma.
c. Iris atrophy.
d. Decreased reading acuity.
24. Which one of the following concerning hemoglobinopathy and retinopathy is false?
a. The incidence of proliferative retinopathy is higher in patients with sickle cell thalassemia (Hb SThal) than in patients with SS disease (Hb SS).
b. The incidence of sickle cell trait (Hb AS) in the African American population is approximately 8% and that of SC disease (Hb SC) in the African American population is <0.5%.
c. Retinopathy has not been reported in patients with sickle cell trait (Hb AS).
d. The ocular findings of SC disease (Hb SC) are not limited to the retina.
25. Which of the following statements is false?
a. Like diabetic retinopathy, the earliest pathophysiologic changes in proliferative (SC) reti-nopathy include capillary closure and drop out.
b. Like diabetic retinopathy, SC retinopathy may have both nonproliferative and proliferative forms.
c. Salmon patches, iridescent deposits, and black sunbursts are hallmarks of proliferative sickle cell retinopathy
d. Vitreous hemorrhage, parafoveal capillary non-perfusion, retinal detachment, and choroidal neovascularization are all potential causes of severe visual loss in sickle cell disease.
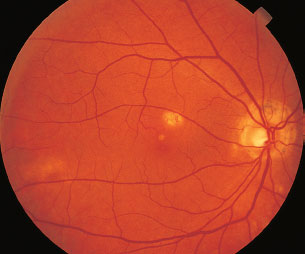
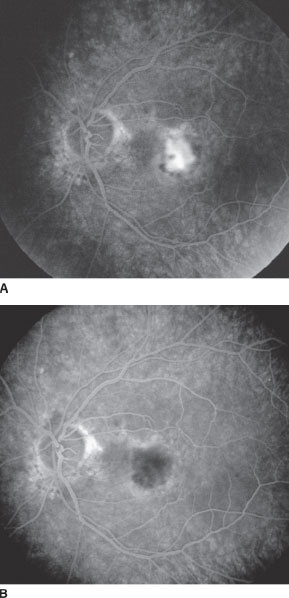
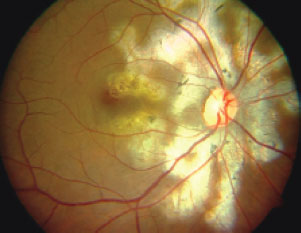
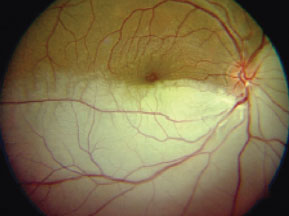
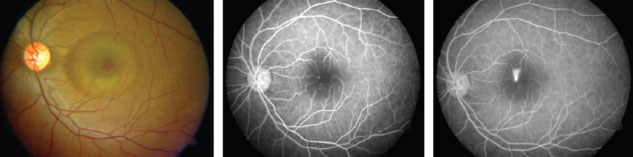
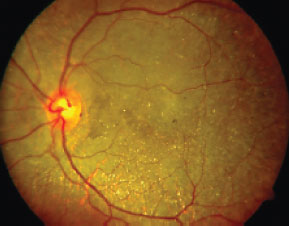
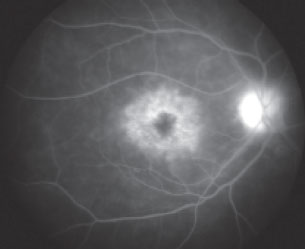
26. It is the end of summer, and a 50-year-old diabetic male is hospitalized for encephalitis. He denies recent travel history, but recalls being bitten by many mosquitoes while playing golf last week. He complains of blurred vision in his left eye (image below). Which of the following is most likely true regarding the etiology of this patient’s disease?
a. The etiology of this patient’s clinical findings is infectious with cats being the natural host.
b. These retinal findings are most likely related to diabetic retinopathy and unrelated to the encephalitis.
c. Vitritis would be an uncommon finding given the clinical scenario.
d. There is currently no proven systemic treatment for this patient.
27. Which of the following statements concerning branch retinal vein occlusion (BRVO) is false?
a. The superotemporal quadrant is the most commonly affected.
b. Risk factors for BRVO include glaucoma, retinal detachment, and hypertension.
c. Complications of BRVO include macular ischemia, retinal neovascularization, and rubeosis.
d. Both long-acting steroid and anti-VEGF intravitreal injections have been effective in managing macular edema secondary to BRVO.
28. Which of the following statements regarding the Branch Vein Occlusion Study (BVOS) is false?
a. The BVOS documented recovery of a final visual acuity of 20/40 or better in 50% more patients treated with argon macular grid laser (compared with those who were untreated).
b. Quadrantic scatter photocoagulation reduces the risk of vitreous hemorrhage in eyes with established neovascularization.
c. Quadrantic scatter photocoagulation reduces the risk of developing neovascularization if the area of retinal ischemia on angiography is at least five disc areas in size.
d. Large areas of nonperfusion were a significant risk factor for the development of neovascu-larization, but quadrantic scatter photocoagulation is not recommended in patients solely with areas of retinal nonperfusion (i.e., without retinal neovascularization).
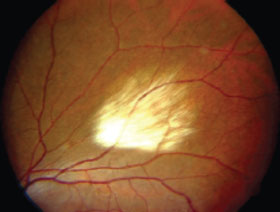
29. Which one of the following concerning solar retinopathy is false?
a. It is generally associated with sun gazing and, less commonly, arc welding.
b. The lesion is a photochemical and photothermal insult to the RPE.
c. Visual acuity loss is generally severe, in the hand motions to counting fingers range.
d. The lesion appears as a small yellow white spot in the center of the fovea that fades over time, often leaving permanent focal RPE changes.
30. What diagnosis should be considered in a 30-year-old male with a history of bilateral giant retinal tears, cleft palate, severe myopia, severe arthritis requiring a total hip replacement, and a family history of severe arthritis and blindness?
a. Ehlers-Danlos syndrome.
b. Marfan’s syndrome.
c. Stickler’s syndrome.
d. Weill-Marchesani syndrome.
31. The key feature on electroretinography distinguishing focal or nonprogressive retinal disease from a diffuse progressive degeneration is an abnormality in the
a. a-wave amplitude.
b. b-wave amplitude.
c. c-wave amplitude.
d. b-wave implicit time.
32. The electrooculogram (EOG) may be valuable in evaluating patients with potential retinal toxicity from
a. Amiodarone.
b. Chloroquine.
c. Phenothiazines.
d. Isoniazid.
33. Which of the following conditions is generally not associated with Purtscher or Purtscher-like retinopathy?
a. Systemic lupus erythematosus (SLE).
b. Thrombotic thrombocytopenic purpura (TTP).
c. Long-bone fractures.
d. Hepatorenal syndrome.
34. Which of the following is generally not considered a function of visual evoked cortical potential testing?
a. To help assess visual acuity in infants with a checkerboard stimulus.
b. To help assess RPE function when retinal function is relatively normal.
c. To help evaluate visual acuity potential in patients with dense cataracts.
d. To help identify visual field defects.
35. Which of the following statements is true regarding color vision testing?
a. Ishihara color plate testing is equally sensitive to Farnsworth Panel D-15 testing in classifying color deficiency, but can be performed significantly faster.
b. Patients with congenital color deficiencies demonstrate irregular patterns on the D-15 test, whereas patients with acquired optic nerve damage generally demonstrate more classic patterns.
c. Blue–yellow confusion errors are easily demonstrated with D-15 testing and generally signify congenital disease.
d. Farnsworth-Munsell 100-hue testing is very sensitive but can be time consuming and cause fatigue.
36. In which of the following subset of patients is central serous chorioretinopathy relatively (CSCR) uncommon?
a. African Americans.
b. Type-A middle-aged males.
c. Patients with elevated corticosteroid levels.
d. Patients with a family history of CSCR.
37. Which of the following statements regarding indocyanine green (ICG) angiography is false?
a. ICG angiography is useful in distinguishing between occult choroidal neovascularization and idiopathic polypoidal choroidal vasculopathy.
b. ICG angiography should not be performed in patients with a known allergy to iodide.
c. ICG angiography has a lower incidence of side effects than does fluorescein angiography.
d. ICG angiography is useful in detecting occult diabetic retinopathy.
38. Which one of the following statements concerning Leber’s congenital amaurosis (LCA) is false?
a. In LCA, the infant is typically blind and the electroretinogram is typically minimal or non-recordable at birth.
b. In LCA, the fundus examination is typically normal at birth.
c. Gene therapy with complementary DNA using an adenoviral-associated vector has demonstrated improvement in vision in patients with LCA.
d. The most common pattern of inheritance in LCA is autosomal dominant.
39. Preservation of visual acuity past the age of 45 years in a patient with a retinal degeneration and an X-linked inheritance pattern suggests the diagnosis of
a. Recessive cone–rod degeneration.
b. Gyrate atrophy.
c. Refsum’s disease.
d. Choroideremia.
40. Which of the following statements regarding gyrate atrophy is true?
a. It is inherited on an X-linked recessive basis.
b. There is a systemic deficiency in ornithine aminotransferase activity.
c. Serum abnormalities include hyperornithinemia and hyperlysinemia.
d. Life span is markedly decreased in this disorder.
41. Which of the following concerning fundus flavimaculatus is true?
a. The pisciform lesions seen in the posterior fundus represent lipofuscin-like deposits at the level of the RPE cells.
b. 50% of cases are autosomal recessive.
c. Visual acuity loss is usually severe and most patients become legally blind by the age of 50.
d. On angiography, about 15% of patients have the finding of a “dark choroid,” where the choroid is hypofluorescent.
42. Which form of congenital dyschromatopsia is accompanied by abnormally low visual acuity?
a. Protanopia.
b. Deuteranopia.
c. Tritanopia.
d. Rod monochromatism.
43. Which of the following statements is false regarding Refsum’s disease?
a. Both infantile and adult forms exist.
b. Night blindness can be an early symptom in patients.
c. Phytanic acid levels are typically elevated.
d. Phytanic acid oxidase activity is increased in cultured fibroblasts.
44. What proportion of patients with intracranial hemorrhage have Terson’s syndrome?
a. 10%.
b. 33%.
c. 50%.
d. 90%.
45. Which of the following regarding familial drusen is false?
a. The initial fundus manifestations generally appear in the third decade of life.
b. Mutations in the gene EFEMP1 encoding an extracellular matrix protein are responsible for Doyne’s honeycomb dystrophy.
c. Clinical presentation can be quite variable.
d. The ERG is generally markedly depressed.
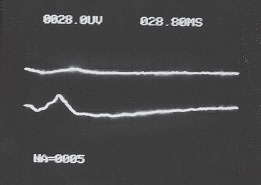
46. Which of the following conditions would explain the electroretinogram found in the picture below (assume that the top line represents the right eye and the bottom line represents the left eye)?
a. Ocular ischemic syndrome.
b. Retinitis pigmentosa.
c. Stargardt’s disease.
d. Proliferative diabetic retinopathy
47. Which of the following treatment modalities should be considered in a macular degeneration patient with the fundus as shown?
a. Monthly intravitreal injections of ranibizumab.
b. Combination of monthly intravitreal bevacizumab and photodynamic therapy.
c. Triple therapy: intravitreal bevacizumab, photodynamic therapy, and intravitreal steroid therapy.
d. Observation.
48. What gene is typically defective in the disease with characteristic fundus findings shown?
a. ABCR.
b. ABCC6.
c. VMD2.
d. TIMP3.
49. Which of the following is not generally present in patients with the disease entity characterized by the fundus photograph shown below?
a. Mild vitritis.
b. Choroidal neovascularization.
c. Discrete, small areas of chorioretinal atrophy.
d. Peripapillary atrophy.
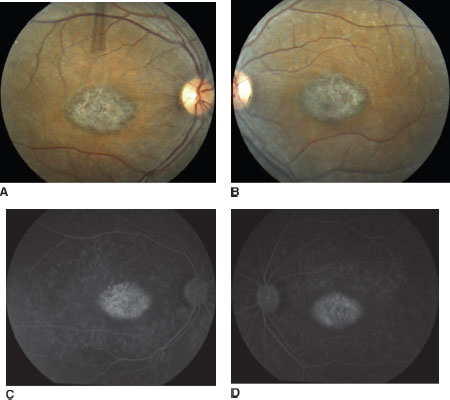
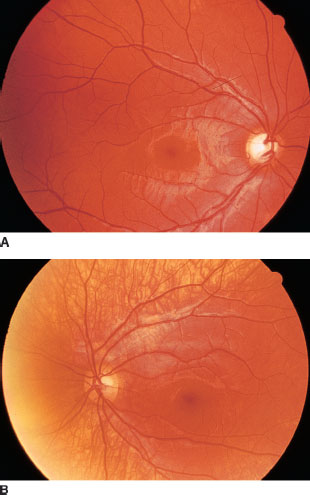
50. Which treatment modality was most likely utilized given the before (image A below) and after (image B below) fluorescein angiography images shown?
a. Photodynamic therapy.
b. Focal laser treatment.
c. Epimacular beta radiation therapy.
d. Intravitreal pegaptanib therapy.
51. Which of the following is not a typical finding in patients with Usher’s syndrome?
a. Epiretinal membrane.
b. Deafness beginning in middle adulthood.
c. Retinitis pigmentosa.
d. Stable hearing levels over time.
52. In a patient with the fundus shown below, aside from the hemorrhage, what do the linear lesions shown in the macula most likely represent?
a. Retinal angiomatous proliferation.
b. Rupture of Bruch’s membrane.
c. Epiretinal membrane.
d. Geographic atrophy.

53. Which of the following conditions listed will generally not result in the fundus image shown below?
a. Retrobulbar injection.
b. Chronic renal failure.
c. Acute pancreatitis.
d. Proliferative diabetic retinopathy.

54. Which of the following is generally not associated with branch retinal arterial occlusion (BRAO)?
a. Mitral valve prolapse.
b. Oral contraceptive use.
c. Thrombocytopenia.
d. Intravenous drug abuse.
55. Which of the following concerning idiopathic juxtafoveal telangiectasis (IJT) is not true?
a. Of the subtypes, only one seems to fall within the spectrum of Coats’ disease.
b. Focal laser treatment in the forms not associated with Coats’ disease generally results in preventing visual loss.
c. Visual loss is generally due to choroidal neovascularization and geographic atrophy.
d. Fluorescein angiography, unlike optical coherence tomography (OCT), is generally normal.
56. Which one of the following concerning Coats’ disease (retinal telangiectasis) is false?
a. The male-to-female ratio is approximately 7:1.
b. It is primarily a disease of childhood, although adults may be affected.
c. Inheritance is autosomal dominant with incomplete penetrance.
d. Management options include photocoagulation and cryotherapy.
57. Which of the following constitutes the histologic definition of the macula?
a. The area of the retina with increased xanthophyll pigment concentration.
b. The area of the retina whose ganglion cell layer is more than one cell layer thick.
c. The area of the retina with the tallest retinal pigment epithelial cells.
d. The area of the retina within the temporal arcades.
58. Which is the outermost layer supplied by the central retinal circulation?
a. Ganglion cell layer.
b. Inner plexiform layer.
c. Inner nuclear layer.
d. Outer plexiform layer.
59. Which one of the following concerning fluores-cein angiography and the blood–ocular barrier is true?
a. Fluorescein is a high molecular weight compound normally confined to the intravascular space.
b. Fluorescein absorbs light in the yellow–green range (530 nm) and, once excited, emits light in the blue range (490 nm).
c. The “red-free” filter is the initial filter through which white light passes before entering the eye.
d. Autofluorescence images cannot be acquired after intravenous fluorescein injection.
60. Which of the following concerning the characteristics of hyperfluorescence patterns on fluorescein angiography is false?
a. Staining generally refers to the uptake of fluorescein by solid collagenous tissue.
b. Transmitted fluorescence, or a window defect, generally implies a focal defect in the retinal pigment epithelium.
c. Pooling implies collections of fluorescein within fluid-filled spaces.
d. True leakage consists of early hyperfluorescence that diminishes in late views.
61. Which of the following with regard to the classification of age-related macular degeneration (AMD) is false?
a. Nonexudative AMD accounts for 90% of all patients affected by this disorder.
b. Exudative AMD accounts for 90% of all patients with severe visual loss (worse than 20/200) who are affected by this disorder.
c. Patients with either pigment epithelial detachment or choroidal neovascularization should be considered to have exudative AMD.
d. In patients with nonexudative AMD, those with central geographic atrophy generally preserve the best visual acuity.
62. A randomized clinical trial has documented that vitreous surgery with gas–fluid exchange and prone positioning offers no long-term benefit relative to observation for which of the following conditions:
a. Idiopathic macular hole, stage 1.
b. Idiopathic macular hole, stages 1 and 2.
c. Idiopathic macular hole, stages 1, 2, and 3.
d. Idiopathic macular hole, regardless of stage.
63. The prevalence of a full-thickness macular hole in the fellow eye of a patient with an established full-thickness macular hole is approximately
a. <10%.
b. 15% to 25%.
c. 25% to 50%.
d. >75%.
64. The lesion that is felt to be an immediate precursor to a full-thickness macular hole is
a. A complete posterior vitreous detachment.
b. A macular cyst.
c. A sensory retinal detachment involving the fovea.
d. A subfoveal pigment epithelial detachment.
65. Which of the following concerning ocular toxicity of hydroxychloroquine and chloroquine is false?
a. Both hydroxychloroquine and chloroquine have been clearly associated with retinal toxicity and may also be associated with a vortex keratopathy.
b. Obese patients are generally at lower risk of developing toxicity than “leaner” patients.
c. Important tests in the evaluation for subclinical chloroquine retinopathy include color vision testing and threshold central visual field testing.
d. Vision loss from hydroxychloroquine toxicity generally does not recover and can progress even after discontinuation of hydroxychloroquine.
66. Which of the following drugs most likely resulted in the retinopathy shown in the image at the top of the next page?
a. Thioridazine.
b. Hydroychloroquine.
c. Talc.
d. Tamoxifen.

67. A 30-year-old presents with fundus findings demonstrated in the image below as well as peripheral retinal neovascularization. The patient is most likely:
a. A longstanding intravenous drug abuser.
b. A young female using oral contraceptives with a history of systemic lupus erythematosus.
c. A hepatitis C–positive patient with significant abdominal distention.
d. A patient treated with intravitreal ranibizumab for age-related macular degeneration.
68. Which disease should one suspect in a young boy with vascular attenuation, optic atrophy, peripheral pigmentary loss, seizures, and a history of progressive dementia?
a. Usher’s syndrome.
b. Retinitis pigmentosa.
c. Leber congenital amaurosis.
d. Batten’s disease.
69. Which of the following molecules is likely defective in a patient with the fundus photograph shown below?
a. Hexosaminidase A.
b. Alpha-galactosidase A.
c. Apolipoprotein B.
d. Ornithine aminotransferase.

70. The mother of a young Puerto-Rican child with the fundus similar to the one shown below should be queried as to:
a. Whether her son has asthma or breathing difficulty.
b. Whether her son bruises easily.
c. Whether her son has been abusing intravenous drugs.
d. Whether her son has developmental delay.
71. Which of the following disorders is considered a form of congenital stationary night blindness (CSNB)?
a. Oguchi’s disease.
b. Fundus flavimaculatus.
c. Retinitis punctata albescens.
d. Leber congenital amaurosis.
72. Symptoms of cone dystrophies can include all of the following, except:
a. Progressive loss of visual acuity.
b. Hemeralopia.
c. Anisometropia.
d. Photophobia.
73. Which of the following is not an area of firm vitreoretinal attachment?
a. The vitreous base.
b. The edge of retinal scars.
c. The edge of the optic nerve.
d. The vortex veins.
74. Which of the following statements regarding posterior vitreous detachments is false?
a. The prevalence of posterior vitreous detachment (PVD) is higher after intracapsular cataract surgery than after extracapsular cataract surgery.
b. Less than 20% of patients with a symptomatic PVD actually have a retinal tear.
c. More than 50% of patients with an acute symptomatic PVD and associated vitreous hemorrhage on clinical examination also have a retinal tear.
d. OCT has demonstrated that vitreous detachments often start at the optic disc and spread temporally.
75. Which of the following statements regarding lattice degeneration is true?
a. The prevalence of lattice retinal degeneration in the adult population is approximately between 5% and 10%.
b. More than 75% of all eyes with a rhegmatogeneous retinal detachment (RRD) exhibit lattice degeneration.
c. Lattice degeneration is bilateral in over 75% of cases.
d. Lattice degeneration is much less common in high myopes.
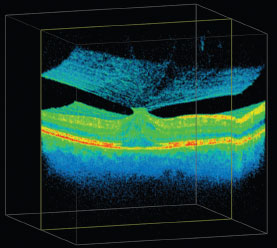
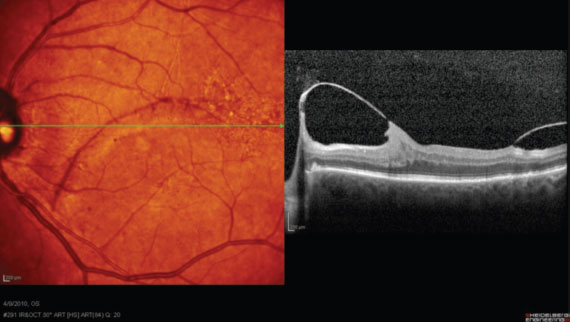
76. A patient with the 3D OCT findings below is seen in your clinic. Which of the following is least likely?
a. Spontaneous resolution may occur.
b. Complete posterior vitreous detachment likely occurred in the past.
c. Surgery may be indicated, depending on symptoms.
d. Angiography may demonstrate leakage of fluorescein dye from retinal vessels in the macular region as well as from the optic nerve.
77. A 17-year-old boy presents with complaints of difficulty reading his schoolwork. He is completely healthy. Visual acuities measure 20/80 in the right eye and 20/100 in the left eye. Fundus photographs and angiography are shown at the top of the next page. Which one of the following is false regarding his case?
a. One of his parents almost certainly has similar findings.
b. His ERG may be normal.
c. Examination of his peripheral retina may show yellow–white flecks.
d. His visual fields may be normal, but he can be counseled to expect further visual loss.
78. A 58-year-old man with essential hypertension is referred to a retinal specialist with “rule out cystoid macular edema” 4 weeks after uncomplicated phacoemulsification on his right eye. His best corrected acuity is 20/40 in the right eye and 20/200 in the left eye. Examination of the right eye shows a quiet pseudophakic anterior segment. The vitreous is clear bilaterally. There is a posterior subcapsular cataract in the left eye felt sufficient to account for his acuity. His fundi are shown below. Peripherally, he has bilateral inferior retinal detachments that shift with head position. No retinal breaks are seen. A fluorescein angiogram for the right eye is shown below (angiographic quality for the left eye was poor due to the cataract). Which one of the following regarding this man is true?
a. Therapy should include retrobulbar steroid and a topical nonsteroidal agent.
b. Therapy should include laser photocoagulation of the right macula.
c. Therapy should include oral steroids.
d. The patient should be promptly referred to his internist.
79. A 75-year-old woman presents to you complaining of painless decreased vision in her left eye worsening over the past 6 hours. She denies any other systemic problems and has no other medical history. Blood pressure, measured in your clinic, is 145/90. Ophthalmic examination reveals a visual acuity of 20/20 OD and CF at 6 ft OS. Ophthalmic examination reveals a normal right eye, an RAPD OS, and the left fundus as shown below. Which of the following would be the most appropriate next step?
a. Obtain a serum ANA, ACE, lysozyme, HLA-B27 haplotype testing, and place a PPD.
b. Obtain a serum erythrocyte sedimentation rate and C-reactive protein.
c. If the patient does not have a history of jaw claudication, initiate ASA 325 mg sublingually.
d. Obtain an FTA-Abs and VDRL.

80. A 20-year-old male presents with the findings in image shown at the top of the next column. Which of the following statements with regard to the condition shown above is true?
a. The condition is usually inherited in an autosomal dominant fashion.
b. The retinal pathology is typically in the outer plexiform layer.
c. A late petalloid leakage pattern seen with fluorescein angiography is pathognomonic.
d. Mutations of the gene responsible for this condition lead to Müller’s cell degeneration.
81. A 45-year-old man complains of blurry vision in his right eye that has gradually worsened over the past 2 years. His right fundus is shown below. There are no other abnormalities that you detect in his right eye. Which of the following statements regarding the condition shown is true?
a. The condition is typically bilateral.
b. Patients with this condition generally have a good visual prognosis.
c. Amazingly, the lesions shown generally do not create any visual field deficits.
d. The condition generally is not chronic.
82. Which of the following statements regarding the condition shown (image at the top of the next page) is true?
a. Most cases of this condition are bilateral.
b. Visual acuity in patients with this condition is generally <20/200.
c. The prevalence of this condition is increased in patients with diabetes.
d. The condition is common in young Asian males.
83. A 20-year-old Jewish man complains of blurry vision bilaterally and difficulty driving at night. The fundus of his right eye (shown below) is very similar to the that of his left eye. Which of the following statements regarding the condition shown is false?
a. The condition can be inherited via several inheritance patterns.
b. Night blindness is one of the earliest symptoms of the disorder.
c. An ERG would typically show reduction of both a-wave and b-wave amplitudes.
d. The presence of bone spicules and chorioreti-nal atrophy is virtually pathognomonic for the condition.
84. An 8-year-old boy is having difficulty seeing in his left eye. His ophthalmic (including fun-duscopy) examination is normal except for his left fundus. A peripheral photograph of his left fundus is shown at the top of the next column. Which of the following statements is true regarding the patient’s condition?
a. Although not so in this specific case, most cases of this condition are bilateral.
b. The condition is typically inherited in an X-linked recessive pattern and has a high male preponderance.
c. The condition can generally be managed with a single session of laser photocoagulation or cryotherapy.
d. Although it can occur, retinal neovascularization is not common.
85. A 10-year-old boy is found to have the fundus appearance shown below. Which of the following statements is true regarding the patient’s condition?
a. The condition is typically unilateral and idiopathic.
b. The ERG is generally normal, and the EOG is abnormal in eyes with this condition.
c. Visual acuity is generally 20/200 or worse at the stage shown.
d. To date, the gene responsible for this condition has not been identified.

86. Which of the following statements regarding the condition shown below is true?
a. The condition can be a precursor for malignant transformation.
b. The condition typically leads to rhegmatogenous retinal detachments.
c. The condition has been associated with nystagmus and amblyopia in the past.
d. The condition requires cryotherapy or laser in symptomatic patients in order to prevent retinal detachments.
87. Which of the following statements regarding the condition shown below is true?
a. The most likely diagnosis is an ophthalmic artery obstruction.
b. An ESR and CRP should be drawn to rule out giant cell arteritis in patients who present with this condition.
c. The most likely diagnosis is iatrogenic subretinal silicone oil after pars plana vitrectomy.
d. Sphingolipidoses are usually the cause of this condition.
88. Which of the following statements regarding the condition shown below is true?
a. A defect in the gene for fibrillin is the most common systemic disease associated with the condition.
b. Photodynamic therapy (PDT) currently has no known role in the treatment of this condition.
c. Fluorescein angiography of the eye shown above will most likely demonstrate early hypofluorescence followed by late staining.
d. Up to half of all patients with this condition will have no systemic medical condition.

89. A 25-year-old woman complains of blurry vision in her right eye over the past 3 days. She denies any past medical or ocular history. Anterior segment exam is normal bilaterally. Her right fundus and angiogram are shown below and at the top of the next page. Which of the following statements is true?
a. The condition shown is generally unilateral.
b. Visual prognosis is generally poor.
c. The condition can be associated with a fatal vasculitis.
d. The vast majority of patients have a viral prodrome before visual loss occurs.

90. Which of the following statements regarding the pathology shown below is true?
a. Visual acuity in this patient is probably normal.
b. If this eye is from a type 2 diabetic patient, early vitrectomy may be indicated.
c. If this eye is from a type 1 diabetic patient with severe proliferative diabetic retinopathy, early vitrectomy may be beneficial.
d. Hypertension is the most frequent cause of this condition in adults.
91. Which of the following statements regarding the condition shown in the next column is true?
a. The condition shown is a posterior staphyloma.
b. AIDS patients presenting with this condition must obtain neuroimaging.
c. This particular patient will likely need a prolonged course of steroids to help preserve visual acuity.
d. Folic acid is used in patients being treated for this condition to protect against thrombocyto-penia and leukopenia.

92. A 39-year-old retinal surgeon complains of the onset of blurry vision in his left eye over the past week. Ophthalmic examination is normal bilaterally, except for the left fundus, which is shown in the next page. To confirm your diagnosis, you decide to obtain a fluorescein angiogram, part of which is depicted at the top of the next page. Which of the following statements is true?
a. The leakage pattern shown on the late frame of the angiogram occurs in most cases and is pathognomonic.
b. More than half of all eyes with this condition eventually develop permanently reduced visual acuity.
c. Given his occupational needs, early focal photocoagulation in this patient would be the treatment of choice.
d. Reduced fluence photodynamic therapy may be of benefit if his symptoms do not resolve.
93. Which of the following most likely represents the condition shown below?
a. Retinitis punctata albescens.
b. Fundus albipunctatus.
c. Oguchi’s disease.
d. Enhanced S-cone syndrome.
94. A 28-year-old Asian female with perilimbal vitiligo complains of blurry vision bilaterally, which has dramatically worsened over the past 2 days. She denies any past medical or ocular history or any recent history of trauma. Her left fundus is shown below. Two frames from a fluorescein angiogram (FA) are also shown below. Which of the following statements is true?
a. The patient most likely has sympathetic ophthalmia.
b. The patient most likely has endophthalmitis.
c. Most patients with this condition develop Sugiura’s sign.
d. The prognosis of this condition is generally poor.
95. A 50-year-old man complains of fever, malaise, and visual loss in his right eye 2 weeks ago. The right eye fundus is shown below. Which of the following statements is false?
a. Given his history, the most likely etiologic agent for his condition is Bartonella henselae.
b. Oral ciprofloxacin is an effective treatment for this patient.
c. The patient may have a painful lymphadenopathy as well.
d. This patient will likely have a chronic recurrent course with poor visual prognosis.
96. Which of the following conditions in a patient with a history of limbal opacities is most likely to represent the fundus shown below?
a. Hydroxychloroquine retinopathy (retinal crystals and cornea verticillata).
b. Bietti crystalline corneoretinal dystrophy.
c. Cystinosis.
d. Synchysis scintillans.
97. A 65-year-old man undergoes uncomplicated phacoemulsification and PCIOL implantation in his right eye. Two months later, he complains of blurry vision in his right eye, but his vision remains 20/20 in that eye. An FA is performed and is shown below. Which of the following statements regarding the patient’s condition is false?
a. The patient has Irvine-Gass syndrome.
b. The patient’s condition will most likely spontaneously resolve.
c. Angiographic evidence of this condition is more common than clinical evidence.
d. The peak incidence of this condition is generally within 2 weeks after surgery.
98. A 70-year-old Japanese man complains of visual loss in his left eye. His right eye reveals a few scattered macular drusen. Fluorescein and ICG angiography frames are shown at the top of the next page. Which of the following statements regarding this man’s condition is true?
a. The condition shown usually occurs in women.
b. Retinal neovascularization commonly occurs as shown by ICG angiography.
c. This condition often shows serosanguinous detachments of the retina.
d. Multiple confluent drusen are common in this condition.
99. Mutations in what gene could result in the angiogram shown below, assuming that the left eye had a very similar appearance?
a. Peripherin/RDS.
b. Rhodopsin.
c. Ornithine aminotransferase.
d. Guanylate cyclase activator 1A.

100. A 95-year-old female complains of longstanding severe visual loss in both eyes. Her right eye looks very similar to her left. What would your best recommendation for treatment be?
a. Monthly bilateral intravitreal ranibizumab.
b. Reduced fluence photodynamic therapy.
c. Submacular surgery.
d. Referral to a low vision specialist.
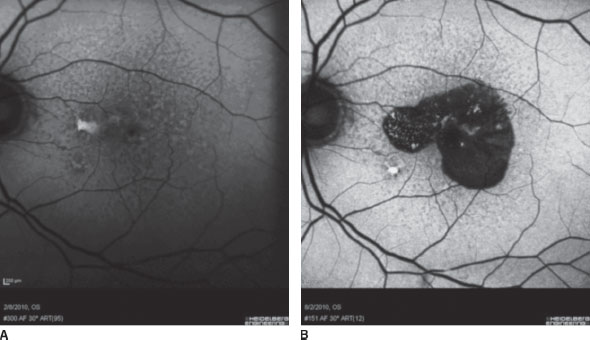
101. An 80-year-old female with a history of exudative age-related macular degeneration was receiving intravitreal ranibizumab therapy. After four injections, her choroidal neovascularization regressed and her vision improved from 20/800 pretreatment to 20/60. After her fifth injection, her vision worsened from 20/60 to 20/200. What does the autofluorescence image below most likely represent?
a. A tear in the retinal pigment epithelium.
b. Extension of geographic atrophy from her macular degeneration.
c. The development of subfoveal hemorrhage after intravitreal injection.
d. Recurrence of her choroidal neovascularization refractory of anti-VEGF therapy.

102. A red-free image and an autofluorescence image of a 20-year-old healthy female are shown in images A and B at the top of the next column. Which of the following statements regarding the condition shown is false?
a. This condition rarely affects non-Caucasians.
b. Most patients have some type of visual field defect.
c. Oral acetazolamide has been shown to improve visual field defects in some cases.
d. The condition may be associated with pseudoxanthoma elasticum.
103. A 52-year-old man with a history of hypertension, hyperlipidemia, type 2 diabetes, and previous history of lung cancer (treated with prior chemotherapy with no known metastasis) complains of gradually worsening vision in his right eye. His blood pressure in your clinic measures 170/80. His fundus photograph and autofluorescence image of his right eye are shown at the top of the next page in left column. After your examination, the next appropriate step would be:
a. Referring him to his internist for better hypertension control.
b. Immediately referring him back to his oncologist and obtaining neuroimaging.
c. Obtaining serum ESR and CRP levels.
d. Obtaining serum HLA-A29 testing.
104. A 29-year-old HIV+ male with a CD4 count of <50 cells/mL complains of decreased vision in his right eye and was found to have the presentation at the top of the right column. Which of the following statements is false?
a. Frosted branch angiitis can be associated with this condition.
b. After his CD4 count rises, he is at risk for developing CME and cataracts.
c. More than one-third of patients with his condition develop retinal detachment within 1 year.
d. Serum IgG titers of the etiologic agent causing this condition are diagnostic.
105. An 80-year-old female presents with sudden loss of vision in her right eye. She specifically complains of difficulty seeing superiorly with her right eye. On clinical examination, she was noted to have macular edema and the fundus as shown below. Which of the following statements is true?
a. She most likely has an altitudinal defect bilaterally.
b. Diabetes and glaucoma are significant risk factors for developing this condition.
c. Long-acting dexamethasone implants have been shown to improve vision in patients with this condition.
d. Given her extensive retinal ischemia, panretinal photocoagulation (PRP) is indicated to prevent the development of retinal neovascularization.
106. A 42-year-old man with the fundus images shown below complains of decreased vision in his right eye. The most likely diagnosis is:
a. Central serous chorioretinopathy.
b. Exudative age-related macular degeneration.
c. Punctate inner choroidopathy.
d. Acute macular neuroretinopathy.
107. A 78-year-old man with a history of nonexudative macular degeneration presents for evaluation, and an autofluorescence image of his left eye is shown below on the left. Six months later, he returns and complains of sudden loss of vision in his left eye, and his vision has worsened from 20/50 to count fingers at 6 ft. An autofluorescence image of his left eye is shown below on the right. Which of the following statements is false?
a. His vision loss due to extension of his geographic atrophy is clearly demonstrated on the autofluorescence image at his 6-month follow-up.
b. Intravitreal bevacizumab may benefit this patient.
c. He is at risk for developing similar findings in his fellow eye.
d. The large subfoveal lesion would likely hypofluoresce on fluorescein angiography.
108. A 50-year-old hypertensive man was treated with laser treatment for the condition shown. Fluorescein angiograph (left) and ICG angiograph (right) are shown at the top of the next page. Which of the following statements regarding this condition is false?
a. This condition is most commonly unilateral and associated with hypertension.
b. ICG angiography can often be helpful in differentiating this condition from exudative age-related macular degeneration.
c. This condition can present with subretinal, intraretinal, or preretinal hemorrhage.
d. Macular edema resulting from this condition is best treated with photodynamic therapy to the lesion causing the edema.
109. A 65-year-old man presents with gradually decreasing vision in his left eye and spectral domain OCT of his left eye is shown below. Which of the following statements regarding this condition is false?
a. This condition is associated with mutations in the COLA1 gene.
b. Optic disc leakage would likely be present on fluorescein angiography in this patient.
c. Pars plana vitrectomy and internal limiting membrane peeling can often improve vision in patients presenting with this condition.
d. This condition may spontaneously resolve with time.
110. The right eye and left eye of a young boy with a history of seizures and cerebral calcification are shown below. Which of the following statements regarding this condition is true?
a. This condition is generally inherited in an autosomal recessive fashion.
b. Mental retardation is almost always present.
c. Lesions from this condition are always present at birth.
d. Unilateral glaucoma is common in this condition.
111. Which of the following potentially fatal systemic tumors is generally not associated with the lesion shown in the fundus photograph shown at the top of the next column?
a. Renal cell carcinoma.
b. Cerebellar hemangioblastoma.
c. Pheochromocytoma.
d. Colon adenocarcinoma.

112. The right eye of a patient is very similar to his left eye shown below. His children and his father also exhibit very similar fundus features. Which of the following statements regarding the condition he most likely has is true?
a. He most likely has a family history of breathing difficulty.
b. He most likely has esotropia.
c. Most commonly, the nasal retina fails to vascularize, leading to tractional detachment.
d. The X-linked variant of this condition is linked to the locus of Norrie’s disease.

113. Which of the following statements regarding bevacizumab is false?
a. It has been approved for the treatment of colon cancer, but is used intravitreally for the management of age-related macular degeneration.
b. Although it was developed by the same company that developed ranibizumab, it is significantly less expensive to administer than intravitreal ranibizumab.
c. It likely has a longer half-life when administered intravitreally compared to that of ranibizumab.
d. Although it is commonly used by retinal specialists, it has been shown to be less efficacious in the treatment of age-related macular degeneration than ranibizumab as of 2010.
114. Which of the following descriptions of severity of retinopathy of prematurity (ROP) is incorrect?
a. Stage 1: presence of a flat demarcation line between vascularized and nonvascularized retina.
b. Stage 2: presence of a demarcation line with height, width, and volume (ridge).
c. Stage 3: presence of a ridge with fibrovascular proliferation.
d. Stage 4: total retinal detachment with funnel.
115. Which of the following statements regarding retinopathy of prematurity is correct?
a. Plus disease is characterized by retinal neovascularization at the posterior pole.
b. Eyes with ROP only in zone III generally have a good prognosis.
c. Threshold disease is defined as more than eight contiguous clock hours of extraretinal neovascularization or 12 cumulative clock hours of extraretinal neovascularization in association with plus disease and location of retinal vessels in zone I or zone II.
d. Spontaneous regression of ROP occurs in <50% of patients.
116. Which of the following systemic disorders is not associated with CRVO?
a. Diabetes.
b. Glaucoma.
c. Hypertension.
d. Cataracts.
117. Which of the following statements regarding phakomatoses is true?
a. An ophthalmologist treating a retinal hemangioma may expect temporary worsening of exudation following successful treatment.
b. Both congenital arteriovenous malformations of the retina (racemose angioma) and cavernous hemangiomas of the retina are distinguished from the vascular malformations of von Hippel’s disease by the lack of exudation and subretinal fluid.
c. The most common complication of retinal cavernous hemangioma is increased episcleral venous pressure.
d. Sturge-Weber syndrome is inherited in an autosomal recessive fashion.
118. Which of the following factors supports an etiologic connection between Histoplasma infection and the presumed ocular histoplasmosis syndrome (POHS)?
a. Over 90% of patients with POHS have a positive histoplasmin skin reaction.
b. The highest prevalence of POHS is among the populations of the southwest states such as New Mexico, Arizona, and California.
c. In biopsies of patients with vitritis, Histoplasma organisms have been recovered from the human vitreous.
d. Systemic treatment with antifungal agents leads to resolution of the ocular findings.
119. Which of the following is not a method of treatment of choroidal neovascularization secondary to ocular POHS?
a. Intravitreal bevacizumab.
b. Systemic antifungal medications.
c. Photodynamic therapy.
d. Argon laser photocoagulation.
120. The best predictor of future contralateral visual loss in a patient with a disciform macular scar from POHS is the presence or absence of
a. A focal macular scar in the better eye.
b. Peripapillary scarring in the better eye.
c. Active vitritis in the better eye.
d. Symmetric peripheral punched-out lesions of each eye.
121. Which of the following concerning angioid streaks is true?
a. They always extend in continuity from the optic nerve head.
b. They appear as window defects on fluorescein angiography.
c. The typical pattern forms concentric circles around the optic nerve head.
d. Histopathologically, they represent discontinuities in a thickened, abnormal choroid.
122. Which of the following statements regarding idiopathic epiretinal membranes is false?
a. They are bilateral in 20% of patients.
b. They are found in 20% of patients over the age of 75.
c. The majority of patients with idiopathic epiretinal membranes maintain vision better than 20/50.
d. They are more common in women.
123. What radiation dosage level may be considered a threshold for the development of radiation retinopathy?
a. 500 rad.
b. 1,000 rad.
c. 3,000 rad.
d. 5 Gy.
124. Which of the following concerning the distribution of photoreceptors in the normal human retina is true?
a. The ratio of rods to cones is approximately 4:1.
b. There are far more cones than rods in the central 18° of the macula.
c. Cone density is maximal in a ring 20° to 40° eccentric to the foveola.
d. Nearly half of all cones lie outside the macula.
125. Which of the following statements regarding giant retinal tears and retinal dialyses is false?
a. A giant retinal tear is a circumferential retinal break of 90° or greater (three clock hours or more).
b. Eyes with retinal dialyses usually have associated posterior vitreous detachments (PVDs).
c. Idiopathic giant retinal tears are the most common form of giant retinal tears, and they mostly occur in males.
d. Retinal dialyses generally occur either at or slightly posterior to the ora serrata.
126. Which of the following statements regarding electroretinograms (ERG) is true?
a. A blue flash of light in a dark-adapted patient will generate an ERG with rod input only.
b. A blue flash of light in a light-adapted patient will generate an ERG with cone input only.
c. Increasing the intensity of the stimulus flash in a scotopic ERG will result in a decrease in both implicit time and amplitude of the b-wave.
d. In order to truly isolate cone function, it is necessary to present a light stimulus as flicker flash at a minimum of 5 Hz.
127. Which of the following statements concerning electrooculography (EOG) is true?
a. The corneal surface or vitreal space is positive relative to sclera.
b. Amplitudes generally diminish with light adaptation and increase with dark adaptation.
c. Amplitudes are typically measured by alternating vertical gaze from up to down.
d. An EOG is generally considered abnormal if the dark-peak to light-trough is <3.5.
128. Both electrooculography (EOG) and electroretinography (ERG) are similarly depressed for all of the following conditions, except:
a. Choroideremia.
b. Gyrate atrophy.
c. Oguchi’s disease.
d. Best’s disease.
129. Which of the following is not a reported complication from intravitreal injection?
a. Retinal detachment.
b. Anaphylaxis.
c. Retinal pigment epithelium tear.
d. Transmission of HIV.
130. The most common pattern of congenital dyschromatopsia is:
a. Deuteranomaly.
b. Protanomaly
c. Protanopia.
d. Deuteranopia.
131. Which of the following statements regarding retinitis pigmentosa is true?
a. The vast majority of severe hearing loss associated with retinitis pigmentosa (RP) is acquired.
b. Usher’s syndrome describes any combination of pigmentary retinopathy and partial or complete acquired deafness.
c. Many patients with Usher’s syndrome may have cerebellar and/or vestibular abnormalities.
d. Unilateral retinitis pigmentosa is generally inherited in an X-linked recessive fashion.
132. Which of the following is not true with regard to a patient presenting with the condition shown at the top of the next column?
a. Visual acuity is almost always normal in patients presenting with this finding.
b. A central core of white glial tissue occupies the position of the normal cup.
c. Serous retinal detachments can occur in approximately one-third of affected patients, but the source of the subretinal fluid is unknown.
d. These ocular findings have been associated with basal encephalocele in patients with midfacial anomalies.
133. A relative lightening of the fundus and RPE after 4 hours of dark adaptation is a feature of which of the following disorders?
a. Fundus albipunctatus.
b. Oguchi’s disease.
c. Retinitis pigmentosa
d. Fundus flavimaculatus.
134. Foveal hypoplasia may be associated with all of the following disorders, except:
a. Albinism.
b. Congenital cytomegalovirus disease.
c. Aniridia.
d. Persistent hyperplastic primary vitreous
135. Which of the following statements regarding diabetic retinopathy is false?
a. Diabetic retinopathy is rarely found in individuals under the age of 10.
b. After 20 years of type 2 diabetes, nearly 99% of patients had some degree of diabetic retinopathy.
c. Diabetic macular ischemia is a common cause of moderate vision loss in patients with diabetic retinopathy.
d. Patients with proliferative diabetic retinopathy are at increased risk of myocardial infarction and cerebrovascular accidents.
136. The finding most frequently associated with degenerative retinoschisis is
a. Peripheral cystoid degeneration.
b. Bullous retinoschisis.
c. Reticular retinoschisis.
d. Rhegmatogenous retinal detachment.
137. Which of the following statements regarding retinoschisis is true?
a. Typical degenerative retinoschisis is associated with an increased risk of retinal detachment.
b. The majority of patients with retinoschisis are hyperopic and have bilateral retinoschisis.
c. The absolute scotoma caused by posterior extension of retinoschisis is highly symptomatic.
d. Retinoschisis is almost always associated with retinal dialysis.
138. In a patient with leukocoria, all of the following findings are more likely to indicate persistent fetal vasculature (PFV) and not retinoblastoma except:
a. Unilaterality.
b. Presence of microphthalmos.
c. Presence of cataract.
d. Presence of calcification.
139. Which one of the following concerning asteroid hyalosis is false?
a. It is more common with aging and is more commonly bilateral.
b. It is generally associated with no decrease in visual acuity.
c. The vitreous is otherwise normal.
d. The particulate matter seen clinically consists of calcium soaps.
140. Findings consistent with exudative detachment rather than rhegmatogeneous retinal detachment include all of the following, except:
a. Shifting fluid.
b. A lack of “tobacco dust.”
c. Smooth, domed appearance of the retina.
d. Undulation of the retina with eye movements.
141. The key prognostic factor in predicting postoperative visual acuity following surgical repair of rhegmatogeneous retinal detachment is:
a. The size of the largest retinal break.
b. The number of retinal breaks.
c. The presence and duration of macular detachment.
d. The presence or absence of myopia.
142. All of the following conditions may increase the risk of rhegmatogenous retinal detachment (RRD), except:
a. Lattice degeneration.
b. Retinal holes
c. Meridional complexes.
d. Cobblestone degeneration.
143. Which of the following is not a risk factor for the development of age-related macular degeneration (AMD)?
a. A history of smoking.
b. A family history of AMD.
c. Advanced age.
d. A history of type 2 diabetes.
144. Which of the following statements regarding AREDS supplementation is false?
a. There may be an increased risk of developing lung cancer in smokers taking betacarotene.
b. Patients with a strong positive family history of AMD should consider taking AREDS supplementation even if they do not yet have AMD.
c. Cupric oxide was included in AREDS supplementation to prevent zinc-induced anemia.
d. Patients taking AREDS supplementation demonstrated a decreased risk of developing AMD even 10 years after starting supplementation.
145. What is the most common complication of vitrectomy surgery?
a. Cataract.
b. Endophthalmitis.
c. Retinal detachment.
d. Vitreous hemorrhage.
146. What is the most common fungus causing chronic postoperative endophthalmitis?
a. Candida.
b. Histoplasma.
c. Aspergillus.
d. Propionibacterium acnes.
147. The EVS has documented which one of the following?
a. Intravenous ceftazidime reduces the duration of severe visual loss in acute postoperative bacterial endophthalmitis, but does not improve long-term visual outcome.
b. Intravenous ceftazidime reduces the duration of severe visual loss and improves long-term visual outcome in patients with acute postoperative bacterial endophthalmitis.
c. Intravenous amikacin reduces the duration of severe visual loss in acute postoperative bacterial endophthalmitis, but does not improve long-term visual outcome.
d. Neither intravenous ceftazidime nor amika-cin offers any therapeutic advantage in acute postoperative bacterial endophthalmitis.
148. Findings of the CVOS include each of the following, except:
a. Grid pattern photocoagulation does not significantly reduce cystoid macular edema (CME) associated with CRVO.
b. Grid pattern photocoagulation does not significantly alter visual outcome in patients with CME associated with CRVO.
c. Roughly 25% to 30% of patients with at least 10 disc areas of nonperfusion will develop iris or angle NV within 3 years.
d. Prophylactic scatter laser showed a trend toward reducing the incidence of iris or angle N V, but baseline differences in the treatment versus no treatment groups eliminated any statistical significance.
149. Which of the following statements regarding optical coherence tomography (OCT) is false?
a. OCT uses a combination of infrared light and sound waves to create images.
b. Images created with OCT have much better resolution than standard 10 MHz B-scan ultrasound.
c. OCT image quality will decrease as the amount of vitreous hemorrhage increases.
d. Ultrahigh resolution OCT can create images with resolutions of 2 to 3 mm.
150. Regarding the surgical treatment of proliferative vitreoretinopathy, which one of the following is false?
a. Silicone oil and SF6 gas are equally effective tamponade agents.
b. Silicone oil and C3F8 gas are equally effective tamponade agents.
c. When silicone oil is used as tamponade in PVR, there is no significant difference in outcomes between eyes undergoing primary (i.e., their first) vitrectomy and previously vitrectomized eyes.
d. When C3F8 is used as tamponade in PVR, there is no significant difference in outcomes between eyes undergoing primary (i.e., their first) vitrectomy and previously vitrecto-mized eyes.
 Answers
Answers1. a. The membrane may be thought of as an elastin sandwich—the bread is collagenous zones and basement membrane on either side.
2. d. The vitreous typically occupies 80% of eye volume, and is most firmly attached to the vitreous base. Vitreomacular traction syndrome generally results with an incomplete PVD with traction on the macula.
3. a. The retinal vasculature generally supplies only 5% of the oxygen required by the fundus. The remainder is supplied by the choroidal circulation. Bipolar cells generally synapse with ganglion cells. The macula, histologically, generally has ganglion cells that are two or more layers thick.
4. c. Treatment is generally reserved for (a) occupational or other demands for rapid recovery of binocular function (unless the lesion has significant proximity to the fovea in which laser treatment can cause permanent vision loss), (b) persistent serous detachment (>4 months), (c) prior episodes of CSCR that have been associated with permanently decreased visual acuity, and (d) permanent visual loss due to CSR in the contralateral eye.
5. a. The image shows a retinal capillary hem-angioma fed and drained by prominent dilated tortuous retinal blood vessels. Superior to the lesion is an area of chorioretinal atrophy subsequent to prior cryotherapy of another retinal capillary hemangioma. These lesions are found in von Hippel-Lindau disease. Café-au-lait spots are characteristic of neurofibromatosis and are not seen as part of von Hippel-Lindau disease.
6. b. Intraocular lens implantation at the time of extracapsular cataract extraction does not change the incidence of CME.
7. c. Eales’ disease is an idiopathic retinal vasculitis in young boys or men (most commonly from India) and is generally bilateral. The original syndrome was defined as retinal vasculitis in a young man with associated epistaxis, constipation, and positive reaction to dermal purified protein derivative (PPD). A potentially lethal cerebral vasculitis also has been recognized as an occasional finding. Neovascularization can be treated with scatter photocoagulation and visual prognosis is generally good with prompt appropriate therapy.
8. d. Fourier-domain OCT offers significantly increased resolution with the added benefit of shorter scan times.
9. b. In Stargardt’s disease, defects in the ATP-binding cassette transporter of the retina (or ABCR) protein lead to an excess of alltrans retinol in the outer segment discs (which are part of the photoreceptor rods).
10. b. Breaks within Bruch’s membrane result in this clinical appearance of angioid streaks. A number of systemic disorders are associated with angioid streaks, including pseudoxanthoma elasticum (“P”), Ehlers-Danlos syndrome (“E”), Paget’s disease of bone (“P”), sickle cell disease and sickle cell trait (“S”), and idiopathic (“I”) causes— remember these by the acronym “PEPSI.” About 50% of cases of angioid streaks are idiopathic.
11. c. The vortex veins drain into the superior ophthalmic vein.
12. b. Urinary discoloration occurs in almost all patients injected with fluorescein sodium. Reduced fluorescein doses should be administered in patients with renal compromise. Finally, pregnant women should generally not receive fluorescein angiography (although its potential teratogenicity has not been identified).
13. d. Acute hypertensive episodes (rather than chronic hypertension) can lead to fibrinoid necrosis of choroidal arterioles. The choroid responds to chronic systemic hypertension in a complex fashion that is usually silent clinically. Hypertensive choroidopathy can also be associated with acute elevations in intraocular pressure.
14. d. The prevalence is 1.4% for intravitreal triamcinolone. Note, however, this also includes cases of pseudoendophthalmitis. Excluding pseudoen-dophthalmitis, the prevalence is 0.6%.
15. d. Pericyte loss occurs early in diabetic retinopathy Capillary closure also may be seen. Basement membrane thickening is found not just in the eye but systemically in diabetics as well. Medial hyperplasia is a feature of hypertensive vasculopathy
16. a. Autofluorescence helps evaluate RPE function. If the RPE is damaged, this is generally represented by loss of autofluorescence (generally appearing darker on autofluorescent images).
17. c. The diffuse pattern of macular edema is generally associated with more widespread vascular insult, often ischemic, and is more difficult to treat than most cases of focal edema. CSME is defined as any thickening within 500 μm from the fovea. Extensive IRMA implies widespread severe injury to small arterioles, with the resulting ischemic state commonly being the immediate predecessor of neovascularization. Retinal tears in patients with proliferative diabetic retinopathy can easily occur as a result of vitreoretinal adhesions formed at areas of neovascularization. Tractional rhegmatogenous retinal detachment (TRRD) is very common in patients with proliferative diabetic retinopathy
18. d. Shorter eyes have greater resistance to fluid efflux from the suprachoroidal space. The percentage of retinal surface area treated is a very important factor and represents the combined effect of total treatment area and the size of the eye.
19. b. The early worsening seen in the DCCT was temporary and had no long-term implications regarding the progression of retinopathy. Patients who had early worsening were more likely to recover and actually improve than patients in the conventional treatment group. The benefit of intensive control was seen in all subgroups of patients stratified by severity of retinopathy at the study’s outset. The DCCT only evaluated type 1 diabetics. The benefit of intensive treatment took up to 3 years to be realized for proliferative retinopathy and 5 years for patients with macular edema. Apparently, diabetic retinopathy builds “momentum,” requiring years of intensive control to arrest.
20. d. All of the others are either difficult to treat successfully (cystoid macular edema) or are associated with significant retinal damage from previous insult (foveal nonperfusion and extensive foveal hard exudates).
21. a. The vitreous acts as a scaffold for the growth of neovascularization and will exert traction once it has developed, leading to hemorrhage and retinal detachment.
22. d. The ETDRS found that twice as many untreated patients lost vision. It is not accurate to conclude that laser treatment is likely to improve vision in diabetic macular edema. A 60% reduction in progression to severe visual loss in patients with so-called high-risk characteristics was reported in the DRS. Disc neovascularization (NVD) greater than one fourth to one-third of a disc area is considered high risk, whether or not it is associated with vitreous hemorrhage. This is in distinction to neovascularization elsewhere (NVE), which must be associated with bleeding to qualify as high risk. Furthermore, to meet the DRS criteria for high-risk disease, NVE also must comprise at least half a disc area. Any NVD associated with hemorrhage is high risk.
23. c. Decreased night vision results from destruction of extramacular rods. Angle-closure glaucoma may occur after particularly heavy treatment associated with choroidal effusions. Regression of neovascular fronds may be associated with contracture and secondary rhegmatog-enous or traction retinal detachment. Laser can cause temporary or permanent dysfunction of the long ciliary nerves passing through the outer choroid and cause difficulties with corneal sensation and accommodation. The latter probably occurs far more often than suspected. PRP also can aggravate macular edema, further compromising near acuity. Iris atrophy is not a potential adverse effect of panretinal photocoagulation.
24. c. Although rare, cases of retinopathy have been reported in association with sickle cell trait (Hb AS) only. In addition, sickle cell disease can be associated with angioid streaks and comma-shaped conjunctival capillaries. The incidence of proliferative retinopathy is as follows: SC disease (Hb SC)—33%; sickle cell thalassemia (Hb SThal)—14%; SS disease (Hb SS)—3%.
25. c. Salmon patches, iridescent deposits, and black sunbursts are hallmarks of nonproliferative sickle cell retinopathy. Both diabetic retinopathy and sickle cell retinopathy are felt to be caused by a similar mechanism: capillary nonperfusion with subsequent retinal ischemia, leading to the production of a vasogenic, diffusible substance. In sickle cell retinopathy, elevated blood viscosity may occlude venules and arterioles, as well as capillaries. With SC disease, obstruction of the central macular blood supply may occur due to thrombosis of a cilioretinal or macular branch artery. This complication is very unusual in other forms of sickle hemoglobinopathies. Conversely, neovascularization is a relatively uncommon feature of SC retinopathy. If choroidal neovascu-larization occurs, it is usually related to angioid streaks. As in diabetes, contracture of neovascular fronds may lead to retinal detachment.
26. d. This patient has West Nile Virus (WNV) chorioretinitis. Fluorescein angiogram shows the classic linear pattern of chorioretinal lesions with central hypofluorescence and peripheral hyperfluorescence. Microaneurysms are present from underlying diabetic retinopathy. WNV is a single-stranded RNA virus of the family Flaviviridae, was first isolated in the West Nile district of Uganda in the 1930s, and first appeared in the United States in 1999. Birds are the natural host, and the virus is transmitted from them to humans through the bite of an infected mosquito. Onset can occur anytime between July and December with peak transmission in late summer. Presenting ocular symptoms include ocular pain, photophobia, conjunctival hyperemia, and blurred vision. A characteristic multifocal chorioretinitis (often in linear array) is seen in the majority of patients, together with nongranulomatous anterior uveitis and vitritis. There is no currently proven treatment for WNV infection. Systemic antivirals such as ribavirin have been found to be active against WNV in vitro but are clinically ineffective. Treatment of anterior uveitis with topical corticosteroids is certainly indicated, but the efficacy of systemic and periocular corticosteroids is unknown for the chorioretinal manifestations of WNV infection.
27. b. Retinal detachment is not associated with the development of BRVO. The most common systemic disease association with BRVO is systemic hypertension, although glaucoma has been associated with BRVO as well. The supertemporal quadrant is most commonly affected in BRVO (almost two-thirds of cases). Complications of BRVO can be divided into acute and chronic categories. Macular edema, macular nonperfusion, and hemorrhage may occur acutely. Macular edema, subretinal fibrosis, and posterior neovascularization can be delayed causes of visual loss following BRVO. Rubeosis iridis occurs in <1% of cases with BRVO. Long-acting steroids (e.g., dexamethasone) and anti-VEGF agents have been shown to be efficacious in preserving visual acuity in patients with macular edema secondary to BRVO and central retinal vein occlusion (CRVO).
28. a. The BVOS showed that nearly twice as many eyes treated for macular edema with photocoagulation recovered 20/40 or better vision (60% vs. 34%). Quadrantic scatter photocoagula-tion treatment is generally not undertaken until signs of neovascularization are evident because the long-term incidence of severe visual loss in patients with extensive nonperfusion is low (only a subset of these actually develop neovascularization). This risk increases once neovascularization occurs. Greater than five disc diameters of ischemia was found to be associated with a 31% risk of developing neovascularization.
29. c. Visual acuity in solar retinopathy is generally not reduced below 20/200 and is frequently only minimally reduced.
30. c. The description is classic for Stickler’s syndrome, or hereditary arthroophthalmopathy. It is inherited in an autosomal dominant fashion and is characterized by progressive myopia with a high incidence of retinal detachment and abnormal epiphyseal development with premature degenerative changes to various joints. Most cases are secondary to premature termination codons in COL2A1—the gene for type II collagen that is a major constituent in both cartilage and vitreous.
31. d. Although the b-wave amplitude can be decreased in focal or stationary retinal disease, the b-wave implicit time is increased only in diffuse, progressive retinal disease.
32. b. An abnormally low light-peak–to–dark-trough ratio on EOG has been found to occur in retinal toxicity from hydroxychloroquine and chloroquine.
33. d. All of the other answers have been associated. Hepatorenal syndrome is generally not associated with Purtscher retinopathy. Chronic renal failure has also been associated with Purtcher-like retinopathy.
34. b. The electrooculogram (EOG ) can help assess RPE function when retinal function is normal. Visual evoked cortical potential (VECP) testing can be abnormal whenever there is a defect in the visual pathway anywhere from the retina to the cortex.
35. d. Blue–yellow errors generally signify acquired disease. D-15 testing is more sensitive than Ishihara color plate testing in classifying color vision deficiencies. Patients with congenital disease generally demonstrate classic patterns of error on the D-15 test, whereas patients with acquired disease (e.g., from optic nerve damage or retinal damage) generally demonstrate more irregular patterns.
36. a. African Americans have a lower incidence of CSCR compared to other races. Type-A middle-aged males and patients with elevated corticosteroid levels are at increased risk of developing CSCR.
37. d. ICG angiography is very useful in helping distinguish between occult CNV and polypoidal lesions. It can also be quite helpful in patients with CSCR. Although it generally is much better tolerated than fluorescein angiography, it should not be used in patients with a known history of iodide allergy as ICG contains 5% iodide. ICG is not useful in diabetics as these patients have pathology that is generally limited to the retina (as opposed to deeper in the choroid).
38. d. Most forms of Leber’s congenital amaurosis are autosomal recessive. Gene therapy using an adenoviral vector has shown some promise in helping patients with this debilitating disease.
39. d. The other syndromes are autosomal recessive. With choroideremia, central acuity is spared until later in life relative to X-linked RP.
40. b. Gyrate atrophy is an autosomal recessive deficiency in ornithine aminotransferase activity. This deficiency causes an increase in serum ornithine levels and a decrease in serum lysine levels. Gyrate atrophy generally does not affect intelligence or lifespan.
41. a. Although the inheritance in Stargardt’s disease/fundus flavimaculatus is generally autoso-mal recessive, autosomal dominant pedigrees also have been documented. Approximately 80% of patients with Stargardt’s disease have a dark cho-roid. Most patients do not become legally blind (e.g., severe visual loss in both eyes).
42. d. Rod monochromats (true color blindness) typically have nystagmus, visual acuity in the 20/200 range, and see the world in shades of gray. Blue-cone monochromats have variable nystagmus and acuities in the 20/40 to 20/200 range.
43. d. Diagnosis of Refsum disease is made by demonstrating elevated plasma levels of phytanic acid or reduced phytanic acid oxidase activity in cultured fibroblasts. Refsum disease is characterized by ataxia, polyneuropathy, anosmia, pigmentary retinopathy, deafness, and cardiac myopathy. Dietary restriction of phytanic acid precursors may slow retinal degeneration.
44. b. Up to one-third of patients with intracranial hemorrhage will have intraocular hemorrhage (the presence of both simultaneously is termed Terson’s syndrome).
45. d. Familial drusen are an autosomal dominant disorder that begins with asymptomatic retinal changes generally observed in the third decade of life. Doyne’s honeycomb dystrophy and Malattia Leventinese are two forms caused by mutations in the EFEMP1 gene on chromosome 2. The ERG is usually normal or mildly decreased.
46. a. The ERG shows significant attenuation of both the a and b waves consistent with ocular ischemic syndrome. The other entities listed are generally bilateral diseases.
47. d. Patients with severe disciform scarring, as shown in this question, demonstrate little benefit with intravitreal anti-VEGF therapy or photodynamic therapy given the extensive damage to the macula.
48. b. The image reveals peau d’orange, angioid streaks, and choroidal neovascularization classic for pseudoxanthoma elasticum, which is generally autosomal recessive and caused by a mutation in the ABCC6 gene. Mutations in the ABCR gene are associated with fundus flavimaculatus. VMD2 and TIMP3 gene mutations are associated with Best disease and Sorsby macular dystrophy, respectively.
49. a. The condition in this image most likely represents presumed ocular histoplasmosis syndrome (POHS), which is characterized by punched out chorioretinal lesions in the retina, peripapillary atrophy, and choroidal neovascularization. Vitritis is not present in POHS.
50. a. Figure B shows significantly reduced choroidal perfusion typical of standard fluence photo-dynamic therapy. The other treatments listed will generally not give you a circular area of hypoper-fusion as shown.
51. b. Usher’s syndrome is the presence of congential hearing loss and retinitis pigmentosa. The hearing loss generally remains stable over time. Epiretinal membrane formation is common in patients with Usher’s syndrome.
52. b. This is a fundus photograph of a patient with pathologic myopia. Characteristic findings include peripapillary atrophy, a tilted optic disc, lattice degeneration with associated retinal holes, and lacquer cracks. Lacquer cracks are breaks in Bruch’s membrane that appear yellowish white.
53. d. The fundus image shown is one of Purtscherlike retinopathy, which can result from various etiologies. Although cotton wool spots can occur with proliferative diabetic retinopathy (PDR), PDR is almost always associated with other retinal findings as well, including retinal neovascularization, dot-blot hemorrhages and microaneurysms.
54. c. Branch retinal artery occlusion (BRAO) can be caused by embolization or thrombosis of the involved vessel with emboli from cholesterol, fibrin-platelet complexes from arteriosclerotic vessels, and calcific emboli. Uncommon causes of emboli include fat emboli, cardiac myxoma, talc emboli in intravenous drug abusers, and septic emboli from endocarditis. Oral contraceptive use, mitral valve prolapse, vasculitides, and connective tissue disorders also have been associated with BRAO. Thrombocytopenia is not associated with BRAOs.
55. d. Group 1 is likely a forme fruste of Coats’ disease, is unilateral, and generally occurs in males, but Groups 2 and 3 are bilateral and occur in both sexes. Microscopically, the structural abnormalities in IJT are similar to diabetic microangiopathy, rather than a true telangiectasia. Unlike diabetes, there is no stimulus for retinal neovascularization. Exudation in type I may respond to laser photocoagulation. Choroidal neovascularization (CNV) can lead to visual loss, but geographic atrophy also occurs in IJT (though rare). OCT can appear “normal” with IJT, but fluorescein angiography generally shows telan-giectasia in the early frames and leakage on late frames.
56. c. Retinal telangiectasia (Coats’ disease, Leber’s miliary aneurysms) is defined by the presence of an exudative retinal detachment with associated vascular anomalies. This condition is not hereditary and is not associated with systemic vascular abnormalities. Usually, only one eye is involved, and there is a significant male predominance.
57. b. Clinically, the macula is 5 to 6 mm in diameter, centered between the temporal vascular arcades. In this region, ganglion cells form two or three sublayers within the ganglion cell layer.
58. c. The retinal vessels supply the nerve fiber layer, the ganglion cell layer, the inner plexiform layer, and the inner third of the inner nuclear layer. The choroidal vasculature supplies the outer two-thirds of the inner nuclear layer, the outer plexiform layer, the outer nuclear layer, the photoreceptors, and the retinal pigment epithelium.
59. d. In fluorescein angiography, white light from the camera first passes through a blue filter. The blue light (wavelength 490 nm) is absorbed by the fluorescein molecules in the retinal and choroidal vasculature, stimulating them to emit yellow–green light (530 nm). A yellow–green filter is placed to block the blue light reflected from the eye, allowing the yellow–green light into the camera. Fluorescein molecules (not bound to albumin), with a molecular weight <600 Da, can easily pass through the spaces between endothelial cells of the choriocapillaris but normally cannot leak through the tight junctions of the RPE or retinal vascular endothelium (blood– retinal barrier). Anaphylactic shock is thought to occur at a rate of <1 in 100,000 procedures. Autofluorescence images can only be acquired before fluorescein injection.
60. d. Leakage appears as an area of early hyperfluorescence that gradually increases in size and intensity throughout the angiogram.
61. d. Findings in the nonexudative form of AMD include pigmentary changes, drusen, and areas of geographic atrophy. Patients with central geographic atrophy generally have a guarded visual prognosis.
62. a. The first study of surgery for macular holes evaluated patients with the earliest stage, stage I. The natural history of the disorder, with up to 50% experiencing spontaneous improvement, is at least as favorable as, if not superior to, surgical intervention.
63. a. Because a significant proportion of early holes spontaneously resolve, only a small fraction, 5%, develop bilateral full-thickness defects.
64. c. Idiopathic macular holes are believed to arise due to both tangential and anteroposterior vitreous traction. The earliest change is loss of the normal foveal depression due to elevation of the fovea itself off the RPE, thus constituting a tiny sensory retinal detachment. This appears clinically as a yellow dot or ring (stages IA and IB, respectively).
65. b. Although hydroxychloroquine is thought to be less toxic, both hydroxychloroquine and chlo-roquine have a significant risk of retinal toxicity leading to atrophic bull’s-eye maculopathy. Color vision testing and threshold central visual field testing (with a 10-2 red target visual field) are important in assessing subclinical retinopathy. The EOG is not the most sensitive parameter in detecting chloroquine retinopathy, although it does reflect pathophysiology (RPE damage) when abnormal. Obese patients are at higher risk of toxicity because of their likely higher dosage of medication. Because of their slow excretion, toxic effects of chloroquine and hydroxychloroquine may progress despite cessation of the drug. Any abnormalities caused by these medications are probably permanent, although mild deficits may be reversible.
66. a. Thioridazine (Mellaril) is more likely to cause retinal pigment stippling or widespread atrophy of the pigment epithelium and choriocapillaris as shown in this image.
67. a. Chronic intravenous drug abusers can develop talc retinopathy (as shown) with talc emboli leading to multiple branch retinal artery occlusions as well as peripheral retinal neovascularization.
68. d. Juvenile neuronal ceroid lipofuscinoses, or Batten disease, is the most common type of neu-ronal ceroid lipofuscinoses (NCL) in the United States. Juvenile visual loss can often manifest as a patient’s first symptom. Death usually occurs by the fourth decade.
69. a. The fundus above shows a classic cherry-red spot found in patients with Tay-Sachs disease, the most common ganglioside storage disease. Ganglioside accumulates within parafoveal ganglion cells leading to the cherry-red spot appearance. Mutations in the alpha-galactosidase A gene result in Fabry’s disease, which is associated with retinal vascular tortuosity and dilatation. Apolipoprotein B is not made in patients with abetalipoproteinemia leading to vitamin A deficiency and retinal degeneration. Patients with mutations in ornithine aminotransferase develop gyrate atrophy.
70. b. Hermansky-Pudlak syndrome is a rare autosomal recessive form of oculocutaneous albinism that can be lethal and must be recognized. It is associated with easy bruising and bleeding secondary to platelet dysfunction and is more common in Puerto-Ricans.
71. a. Oguchi disease and fundus albipunctatus are forms of congenital stationary night blindness with abnormal fundus findings. Fundus flavimaculatus (or Stargardt’s disease) is a condition with abnormal lipofuscin deposition in the RPE. Functional problems in this syndrome are not limited to night blindness and vision loss can be progressive. Retinitis punctata albescens is a phenotype of retinitis pigmentosa (RP) with deep retinal white dots or flecks. Leber congenital amaurosis is a form of infantile RP, not CSNB.
72. c. Cone dystrophies generally lead to progressive loss of color vision and visual acuity. Patients with cone dystrophy may also complain of difficulty with night driving, as urban night driving is generally performed with background illumination at low photopic intensities. Hemeralopia (day blindness) and photophobia (sensitivity to light) are common symptoms as well.
73. d. Other areas of firm vitreoretinal attachment include the major retinal vessels/arcades. The vortex veins represent a firm point of attachment between the choroid and sclera.
74. d. Removal of the lens and posterior capsule allows the hyaluronic acid in the vitreous to diffuse into the anterior chamber and out of the eye, leading to higher prevalence of PVD after intracapsular cataract extraction. Hemorrhage or vitreous cells (“tobacco dust”) are suggestive of retinal breaks. OCT (especially spectral domain imaging) has shown that PVDs often originate in the perifoveal macula.
75. a. Although 5% to 10% of the general population has lattice degeneration, only a small subset will develop a retinal detachment. Lattice degeneration is present in 20% to 30% of eyes with an RRD. Important histologic features of lattice degeneration include discontinuity of the internal limiting membrane and a pocket of liquefied vitreous overlying the degeneration. Vitreoretinal condensation and adherence occur at the margin of the lesion. Other features include sclerosis of the vessels and variable degrees of retinal atrophy. Lattice degeneration is more common in myopes and is bilateral in one-third to one-half of affected patients.
76. b. This patient has vitreomacular traction syndrome (VMT). The incomplete separation and abnormal adherence of the vitreous that remains attached to the posterior pole leads to traction on the macula. Leakage on angiogram can occur at the fovea or optic nerve. While this may resolve spontaneously with complete separation of the vitreous, surgery is often indicated if the vision is significantly decreased or distorted.
77. a. The fundus images show a symmetric pigmentary maculopathy with an evolving “bull’s-eye” appearance. In a young man with no history of treatment with hydroxychloroquine or chloroquine, the differential diagnosis is limited to a few macular dystrophies. The two most commonly associated with bull’s eye maculopathy are cone dystrophy and Stargardt disease (juvenile macular degeneration). The fluorescein shows the “dark choroid” classically seen in Stargardt disease. This is usually inherited on an autosomal recessive basis, meaning his parents are likely carriers with no detectable ophthalmoscopic changes. ERG and visual fields are typically preserved or minimally affected. The pisciform yellow–white flecks are abnormal lipofuscin deposition in the RPE. Typically, both eyes of affected patients stabilize at around 20/200 visual acuity.
78. d. The patient’s history and clinical findings are classic for an unusual paraneoplastic syndrome, bilateral diffuse uveal melanocytic proliferation. The syndrome is seen in patients with cancer, often undiagnosed. In men, lung and colon primaries predominate. In women, neoplasms of the reproductive system (ovarian, uterine) have been reported. The hallmarks of the syndrome, as defined by Gass, include focal red patches at the level of the RPE in the posterior pole (which hyperfluoresce) multiple pigmented and nonpigmented melanocytic “tumors” as well as diffuse proliferation of choroidal melanocytes, exudative retinal detachment, and rapidly developing cataract. Visual loss is initially secondary to cataract and may precede the diagnosis of the cancer. Subsequent photoreceptor loss leads to inexorable, severe visual loss. This is reflected in the ERG as a rod greater than cone degeneration (scotopic greater than photopic loss). The underlying cause is not known but is felt to be due to hormonal effects of the primary carcinoma on preexistent uveal nevus cells. The angiogram shows multiple window defects, reflecting widespread RPE damage corresponding to the red patches and some of the melanocytic deposits. Unfortunately, no treatment is effective at stopping the visual decline. Because there is no serologic test, the diagnosis is made on a completely clinical basis.
79. b. The history and the fundus findings are consistent with a diagnosis of anterior ischemic optic neuropathy, a condition presenting with acute painless visual loss and typically with optic disc edema and pallor. Anyone with AION should be ruled out for arteritic AION (AAION) secondary to giant cell arteritis (GCA), as this is a potentially fatal condition. The best initial way to rule out GCA is with an ESR and CRP, as up to 20% of patients with AAION can present with no systemic symptoms (e.g., jaw claudication, scalp pain, fever, and malaise). ESR and CRP (when both are abnormal) have a 97% specificity for AAION. The gold standard for diagnosing GCA is a temporal artery biopsy. Steroids can be initiated prior to the biopsy (which should be performed within 1 week).
80. d. The condition shown is congenital X-linked retinoschisis (XLRS), a condition that is inherited on an X-linked recessive basis. Splitting of the retina occurs at the nerve fiber layer. Foveal schisis as shown is almost always observed. There is no leakage observed with fluorescein angiogra-phy. Mutations in the adhesion protein retinoschisin, which is responsible for XLRS, result in Müller’s cell degeneration.
81. a. The condition shown is serpiginous chorio-retinopathy, a bilateral condition that usually spreads outward from the optic nerve and/or macula in a serpentine fashion. Serpiginous chorioretinopathy is chronic and recurrent with poor visual prognosis and scotomata affecting the areas of involvement. Treatment with potent immunosuppressives may slow down the disease in some cases, but generally the visual prognosis is poor, especially with macular involvement.
82. c. The condition shown is asteroid hyalosis, a benign condition that is usually unilateral (75% of cases), with good visual acuity. There is a clear association of this condition in diabetic patients. It usually occurs in patients over age 50, and vit-rectomy may sometimes be used to help visualize other retinal conditions (e.g., diabetic retinopa-thy) that are difficult to assess because of the asteroid hyalosis.
83. d. The condition shown is retinitis pigmentosa. Although it can be inherited via several inheritance patterns, X-linked inheritance usually has the worst prognosis. ERG should be performed on all suspected patients to confirm the diagnosis, as the presence of bone spicules and chorioretinal atrophy can occur in a variety of conditions, including severe uveitis, syphilis, chloroquine toxicity, etc.
84. d. The condition shown is Coats disease. Coats disease is not inherited and is generally unilateral. The diagnosis of Coats disease requires the presence of retinal telangiectasia (small anomalous vessels) as shown. It can recur and must be watched carefully, with difficult cases requiring multiple photocoagulation or cryotherapy treatments. Retinal detachments can be late sequelae of the disease. The yellow material is lipid exudate. Posterior retinal neovascularization is not common.
85. b. The condition shown is Best disease (or vitelliform dystrophy). It is inherited in an auto-somal dominant fashion and is secondary to a mutation in the vitelliform macular dystrophy (VMD2) gene (bestrophin) on chromosome 11. Visual acuity in the “sunny side up” stage shown is generally good. The ERG is usually normal, whereas the EOG is generally abnormal in Best disease.
86. c. The condition shown is a myelinated nerve fiber layer (MNFL), a benign condition. It has been associated with nystagmus and amblyopia, but retinal detachment is not associated with MNFL.
87. b. The condition shown is a hermiretinal artery occlusion, manifested by nerve fiber layer edema. Atherosclerotic emboli are often the cause, and GCA is discovered in 1%–2% of cases.
88. d. The fundus photograph shown demonstrates angioid streaks, which can be associated with several diseases (think “PEPSI”). Up to half of all cases are idiopathic, however. Angiography generally shows a window defect representing the breaks in Bruch’s membrane, through which choroidal neovascularization can migrate. Both PDT and intravitreal anti-VEGF therapy have been shown to be of benefit in subfoveal choroidal neovascularization secondary to angioid streaks.
89. c. The condition shown is acute posterior multifocal placoid epitheliopathy (APMPPE). It is usually bilateral, and has a good visual prognosis. Up to one-half of patients have a viral prodrome. Fluorescein angiography often demonstrates early hypofluorescence (indicated blockage of the choroidal pattern) with late hyperfluorescence (as shown in the angiogram frames). While APMPPE is generally benign, it can be rarely associated with a fatal cerebral vasculitis.
90. c. The fundus photograph reveals preretinal/vit-reous hemorrhage overlying the fovea, with likely significantly decreased visual acuity. The most common cause of vitreous hemorrhage is diabetic retinopathy in adults. The Diabetic Retinopathy Vitrectomy Study (DRVS) demonstrated the benefit of early vitrectomy (within 1 to 6 months after vitreous hemorrhage) in type 1 diabetic patients or those patients with vitreous hemorrhage and severe proliferative diabetic retinopathy.
91. b. The condition shown is toxoplasmic retino-choroiditis (a posterior staphyloma generally would not have satellite lesions). The lesions appear inactive and old in this patient and antibiotic therapy and steroids are of no use in this patient (unless the condition recurs). Immunocompromised patients (including AIDS patients) presenting with toxoplasmic retino-choroiditis must obtain neuroimaging to rule out cerebral lesions. Folinic acid (not folic acid) is used in combination with pyrimethamine to protect against iatrogenic thrombocytopenia and leukopenia.
92. d. The condition shown is central serous chorio-retinopathy (CSCR), a condition usually affecting males between the ages of 30 and 50 years, typically with type A personalities. The smokestack presentation shown in the angiogram only occurs in approximately 10% of cases of CSCR. Most eyes with this condition recover visual acuity within 6 months. Early focal photocoagulation in this particular patient (a retinal surgeon) would be contraindicated, given the lesion’s proximity to the center of the macula and the potential for a permanent visual scotoma with focal photocoagulation. Waiting for spontaneous remission would be the most appropriate treatment option. If spontaneous remission does not occur within 6–10 weeks, then reduced fluence photodynamic therapy can be considered as it has been shown to be quite successful in patients with this condition.
93. b. The condition shown is fundus albipunctatus. It can be differentiated from retinitis punctata albescens because of the normal vasculature (typically attenuated in retinitis punctata albescens, an RP variant). Familial drusen would appear similar, although the lesions would not be as uniform in size and would form grape-like clusters. Patients with this condition may have good visual acuity and night blindness may be their only symptom.
94. c. Based on the history, the fundus appearance, and the FA, the patient most likely has Vogt-Koyanagi-Harada syndrome (VKH), which is a bilateral condition characterized by granulomatous panuveitis. VKH is a systemic condition with both neurologic and dermatologic manifestations. The FA clearly demonstrates multiple areas of hyperfluorescence with late leakage into the subretinal space. Sugiura’s sign, or perilimbal vitiligo, occurs in 75% of cases. Given the lack of trauma and the overall health of the patient prior to examination, both sympathetic ophthalmia and endophthalmitis are unlikely. VKH generally has a good prognosis when effectively and rapidly treated with steroids and immunosuppressives.
95. d. The condition shown is neuroretinitis, which, along with a painful lymphadenopathy, can be a manifestation of cat-scratch disease caused by Bartonella henselae. Neuroretinitis, however, can have a variety of different infectious and immunologic causes, and consequently, a thorough history should be obtained from the patient. Both erythromycin and ciprofloxacin can be used to treat cat-scratch disease. The visual prognosis is generally good with the disease being self-limited.
96. b. The condition described is Bietti crystalline corneoretinal dystrophy, which is characterized by limbal corneal opacities and tapetoretinal dystrophy. Plaquenil retinopathy typically causes a bull’s-eye maculopathy. Synchysis scintillans is a condition of cholesterol crystals within the vitreous. Cystinosis typically causes corneal crystals. Fleck retina of Kandori is a disorder similar to fundus albipunctatus with characteristic night blindness.
97. d. The patient has Irvine-Gass syndrome (e.g., cystoid macular edema developing after cataract surgery). The incidence of Irvine-Gass is higher after intraoperative complications, but most cases spontaneously resolve. Peak incidence is 6 to 10 weeks postoperatively.
98. c. The condition shown is idiopathic polypoidal choroidal vasculopathy. In people of Chinese and Japanese origin, it is usually unilateral and generally affects males. In Caucasians, it is more often bilateral and generally affects females. It is characterized by serosanginous detachments of the RPE and retina and can also have associated choroidal neovascularization.
99. a. The angiogram above is from a patient with butterfly pattern dystrophy, which is associated with mutations in the peripherin/RDS gene.
100. d. The patient has bilateral subfoveal disciform scars secondary to advanced exudative age-related macular degeneration. Despite the intraretinal fluid present on spectral domain OCT (SD-OCT), intravitreal anti-VEGF therapy is of very limited benefit in these cases, and no treatment has been clinically proven in this setting. Referral to a low vision specialist is the most appropriate treatment at this point.
101. a. The autofluorescence image represents a tear in the RPE, which can occur after intravitreal injection. The sharp demarcation between the darker area and the lighter area represents the location of the RPE tear.
102. c. Optic disc drusen (ODD) as shown demonstrate autofluorescence (which is shown in the image above). ODD rarely affects non-Caucasians and most patients with ODD have some type of visual field defect. ODD can be associated with pseudoxanthoma elasticum and retinitis pigmen-tosa. No treatment has been shown to improve visual field defects in patients with ODD.
103. b. This patient had a large chorioretinal metastasis secondary to his lung cancer. Urgent referral to his oncologist and obtaining neuroimaging (in conjunction with the patient’s oncologist) is appropriate given that any chorioretinal metastasis is by definition considered a CNS metastasis. The most common primary tumors in patients with chorioretinal mets are lung CA in men (40% of cases) and breast CA in women (almost 70% of cases). Uveal metastases imply a poor prognosis.
104. d. This patient has CMV retinitis, which often occurs in HIV+ patients with low CD4 counts. Treatment is with systemic ganciclovir, intravitreal ganciclovir, or foscarnet. Raising his CD4 count with highly active antiretroviral therapy (HAART) can also eliminate the need for specific anti-CMV treatment. Given that many individuals are seropositive for CMV, serum IgG titers are generally not helpful.
105. c. This patient has a hemiretinal vein occlusion, which is generally unilateral and associated with glaucoma (and not diabetes). Long-acting intravitreal dexamethasone implants, intravitreal anti-VEGF agents, and focal laser treatment have been shown to improve vision in these patients. PRP should be reserved for patients that actually demonstrate retinal neovascularization.
106. a. This patient has multifocal central serous chorioretinopathy as demonstrated by multiple scattered areas of staining (which represent old areas of CSCR) along with new areas of leakage in his left eye.
107. a. This gentleman has developed exudative AMD with choroidal neovascularization and a large, dense area of subretinal hemorrhage that appears dark on autofluorescence image. His visual loss is not because of extension of geographic atrophy (GA) as none is seen on autofluorescence at his initial visit, and GA is unlikely to progress so dramatically within 6 months.
108. d. The condition shown is a retinal arterial macroaneurysm, which is usually unilateral and associated with systemic hypertension in two-thirds of cases. Focal laser treatment for macular edema can be helpful in patients with this condition.
109. a. This patient has vitreomacular traction syndrome, which is not associated with any genetic defects. Optic disc leakage would occur in this patient as he clearly has traction on both his parafoveal area as well as his optic disc. Pars plana vitrectomy surgery is often helpful in these patients. Vitreomacular traction can also spontaneously improve if a complete PVD occurs.
110. c. This patient has Sturge-Weber syndrome, which is one of the phakomatoses that is not genetically transmitted. It is associated with a tomato catsup fundus (the right eye in this case) with associated ipsilateral glaucoma and ipsilateral port-wine stain. Mental ability can vary widely. Lesions from Sturge-Weber syndrome are present at birth.
111. d. The image is a classic retinal capillary hemangioblastoma. Von Hippel-Lindau disease occurs when this lesion is found in patients with associated CNS and/or visceral involvement, including renal cell carcinoma, pheochromocytoma, CNS hemangiomas, and meningiomas. Colon cancer is generally not associated with von Hippel-Lindau disease.
112. d. This patient has familial exudative vitreoretinopathy, which is usually bilateral and associated with exotropia because of the temporal dragging of the macula secondary to the lack of retinal vascularization within the temporal retina. Individuals usually inherit this condition in an autosomal dominant fashion (although the X-linked variant is associated with the Norrie’s disease gene locus). Individuals with FEVR are full-term and generally have normal respiration.
113. d. Intravitreal bevacizumab is more commonly used than intravitreal ranibizumab as of 2011, and there have been no long-term large studies supporting that either agent is superior to the other. The National Eye Institute’s Comparison of Age-Related Macular Degeneration Treatment Trial (CATT) aims to answer this question.
114. d. Stage 5 ROP is total retinal detachment with a funnel. Stage 4 is subtotal RD (4A with extrafoveal RD and 4B with RD including the fovea). All of the other stages listed are correct.
115. b. Plus disease is characterized by retinal vascular dilatation and tortuousity in the posterior pole. Threshold disease is defined correctly in answer c, except for the number of clock hours (five contiguous and eight cumulative). Spontaneous regression occurs in 85% of infants with ROP.
116. d. The most common disease associations for CRVO include atherosclerotic heart disease, hypertension, diabetes, and glaucoma. Less common associations include paraproteinemias, syphilis, sarcoidosis, increased intraorbital pressure, and hypersensitivity and other vasculitides. Cataracts are not independently associated with CRVO.
117. a. In fact, treatment may be associated with a total exudative detachment (which typically resolves). Both congenital retinal arteriovenous malformations and retinal capillary hemangiomas (von Hippel’s disease) are associated with subretinal fluid and exudate. Cavernous hemangiomas bleed but usually do not leak. Retinal cavernous hemangioma most commonly causes vitreous hemorrhage, which is presumed to be secondary to traction. Sturge-Weber syndrome is not a genetically transmitted disorder.
118. a. Endemic areas include the states of Ohio and Mississippi River valleys. POHS is not associated with vitritis. Histoplasma organisms have been found in the choroid of patients with POHS. Systemic antifungal treatment does not lead to resolution of the ocular findings.
119. b. At present, effective methods of treatment for CNV secondary to POHS are intravitreal anti-VEGF therapy, photodynamic therapy, and argon laser photocoagulation (for extrafoveal CNV lesions). Systemic antifungals have not been shown to be effective for CNV.
120. a. The likelihood of contralateral choroidal neovascularization (CNV) in a patient with a disciform macular scar from POHS is increased if there are focal macular scars in the better eye.
121. b. Angioid streaks represent discontinuities in abnormally thickened and calcified Bruch’s membrane. They do not always extend in continuity from the optic nerve head, and they appear to radiate from the optic nerve head, rather than forming concentric circles around it. Because the overlying RPE is often atrophic, angioid streaks may appear as window defects on fluorescein angiography. Systemically, angioid streaks are associated with Paget’s disease of bone, Ehlers-Danlos syndrome, pseudoxan-thoma elasticum, sickle cell (SC) anemia, and idiopathic causes (think “PEPSI”). Up to 50% of patients with angioid streaks have no identifiable systemic illness. High myopia is not associated with angioid streaks but may feature lacquer cracks, which are similar histopathologically.
122. d. Idiopathic epiretinal membranes have no gender predisposition. All of the other statements are true.
123. c. Radiation retinopathy may occur with doses of about 3,000 rad (30 Gy) or greater, although it can occur in patients with 15 Gy of external beam radiation.
124. d. The ratio of rods to cones is at least 12 to 15:1. Some investigators claim a ratio as high as 20:1. Rod density is maximal in a ring 20 to 40 degrees eccentric to the fovea, whereas cone density is greatest in the fovea. Although the cone density is greater in the macula than in the peripheral retina, the number of rods and cones in the macula is roughly equal, and nearly half of all cones lie outside the macula.
125. b. PVDs are generally absent in eyes with retinal dialyses. The converse is true in eyes with giant retinal tears.
126. a. The scotopic ERG represents the ERG with rod input only. It is generated with a dim white or blue flash below the cone threshold in a dark-adapted state. Some rod function is represented even in a light-adapted ERG. Rod input can be minimized or eliminated by using only the longest wavelengths (orange–red), or more practically, by using a flicker stimulus. With increasing stimulus intensity, the b-wave amplitude increases and the implicit time (the time from stimulus to b-wave peak) decreases. Rods can respond to flickering stimuli of rates of up to 20 Hz. Only cones can respond at higher frequencies, with a maximum of about 70 Hz.
127. a. In EOG, amplitudes generally increase with light adaptation and diminish with dark adaptation. Amplitudes are typically measured by alternating lateral gaze from left to right. The EOG is considered abnormal if the light-peak– to–dark-trough ratio (the Arden ratio) is <1.85.
128. d. In Best’s disease, the ERG is generally normal, whereas the EOG is abnormal.
129. d. All of the other answers (including anaphylaxis) have been reported as potential complications of intravitreal injection.
130. a. Deuteranomalous trichromats are the most common. They are X-linked recessive and found in 5% of the male population.
131. c. Some patients with RP will develop moderate hearing loss with age, but most cases of severe hearing loss are congenital. Usher’s syndrome only refers to the association of pigmentary retinopathy and congenital deafness. Usher’s syndrome types I and III feature vestibular dysfunction. Patients with profound deafness are more likely to have cerebellar atrophy. Unilateral RP is generally sporadic and many of these cases are now thought to be diffuse unilateral subacute neuroretinitis (DUSN).
132. a. This is an example of morning glory syndrome. Visual acuity can range anywhere from 20/20 to no light perception but in general is approximately 20/100 to 20/200.
133. b. The Mizuo-Nakamura effect occurs in Oguchi’s disease and X-linked cone dystrophy. The eponym refers to a relative lightening of the RPE and fundus after 3 to 4 hours of dark adaptation.
134. b. Congenital CMV is not associated with foveal hypoplasia.
135. b. The Wisconsin Epidemiologic Study of Diabetic Retinopathy (WESDR) showed that 99% of type 1 diabetes patients and 60% of type 2 diabetes exhibited some degree of retinopathy.
136. a. In virtually all cases of typical degenerative retinoschisis, peripheral cystoid degeneration can be found, usually adjacent to the schisis cavity.
137. b. Greater than 70% of patients with retinoschisis are hyperopic, and this condition is bilateral in 50% to 80% of cases. However, in typical retinoschisis, complications such as hole formation and retinal detachment (RD) are rare. With retinoschisis posterior to the equator, the scotoma, although absolute and readily identifiable on perimetry, is rarely noted by the patient.
138. d. PFV should be included in the differential diagnosis of leukocoria and differentiated from retinoblastoma. PFV is unilateral in >90% of cases and is associated with microphthalmia and cataract. Retinoblastoma is often bilateral and has no significant associations with microphthalmia or cataracts. Calcification is generally found in retinoblastoma and not in PFV.
139. a. Asteroid hyalosis is monocular in 75% of cases.
140. d. Signs suggestive of rhegmatogenous retinal detachment include (a) lower IOP compared with the other eye, (b) “tobacco dust” (small clumps of RPE cells floating in the vitreous), and (c) corrugated appearance of the retina that undulates with eye movements. A smooth, domed appearance and shifting fluid are more suggestive of exudative detachment.
141. c. Degeneration of photoreceptors limits recovery of vision. Seventy-five percent of patients with macular detachment of <1 week’s duration will recover vision >20/70. In contrast, those patients with macular detachment of 8 days’ or greater duration have only a 50% chance of regaining acuity of at least 20/70.
142. d. Lattice degeneration and meridional complexes (redundant retinal folds in the same meridian as a ciliary process, usually occurring superonasally) increase the risk of RRD. Cobblestone degeneration has occasionally been observed to limit the spread of retinal detachment and does not predispose to RRD.
143. d. A history of type 2 diabetes is not independently associated with the development of AMD. All of the other answers listed are risk factors for developing AMD.
144. b. Patients without AMD should not take AREDS supplementation as this was not studied in the AREDS landmark trial.
145. a. Cataract occurs in 90% of patients over the age of 50 years within 2 years of having vitrec-tomy surgery.
146. a. Candida is the most common cause of fungal postoperative endophthalmitis. Candida is also the most common cause of fungal endogeneous endophthalmitis. Propionibacterium acnes, while a common cause of chronic postoperative endophthalmitis, is not a fungus.
147. d. The choice of parenteral antibiotics was controversial. Many surgeons outside the study group felt that intravenous vancomycin would have been a better choice for gram-positive coverage than amikacin, which leaves some staphylococcal species poorly covered. Thus, some retina specialists continue to advocate the use of intravenous vancomycin. More recent evidence demonstrates better penetration with newer agents such as fourth-generation fluoroquinolones. The EVS clearly demonstrated that neither amikacin nor ceftazidime offers any therapeutic advantage when given systemically.
148. a. Clinical and angiographic edema did respond to grid laser treatment. There was no significant effect on long-term visual acuity, so the treatment is no longer recommended.
149. a. OCT only uses light waves to create images. Ultrahigh resolution OCT uses a different laser to create images with much greater resolution.
150. a. The Silicone Oil Study Group found that reattachment rates and visual outcomes were both worse using SF6 as the tamponade agent, compared with either C3F8 or oil.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


