Retina and Vitreous
Elise Héon
Nasrin Najm-Tehrani
Brenda Gallie
Wai-Ching Lam
Peter Kertes
Robert Devenyi
Carol Westall
Thomas W. Wilson
Alex V
The retina develops from the neuroectodermal cells of the optic cup around 4 weeks of gestation. Retinal development occurs in parallel with the development of other organ systems and therefore, explains why retinal diseases of childhood are often associated with disorders of the ear, kidney, or central nervous system. Primary care providers should be informed of the possibility of an underlying syndrome in all children with retinal disease. The retina matures from the center to the periphery.
The photoreceptors, essential to the processing of light, start to develop between 4 and 12 weeks of gestational age. The macula becomes recognizable between 24 and 26 weeks and the fovea will continue to mature after birth until 4 years of age. The retina is a fragile multilayered tissue where light is processed. The major step in the processing of light is called phototransduction, which takes place in the photoreceptors. The integrity of a photoreceptor requires a healthy surrounding, including the retinal pigmented epithelium (RPE) and inner sensory retina. Anomalies at any of these levels may lead to photoreceptor dysfunction and visual loss. This is usually the basis of the complex field of retinal dystrophies. Likewise, abnormalities of the choroid, the vasculature of which nourishes the outer retina, may also lead to retinal degener- ation. For most retinal and choroidal dystrophies, there is no treatment available, but this will change with the great influx of genetic knowledge about these conditions and the rapid progress of retinal gene and pharmacologic therapy.
Retinopathy of prematurity (ROP) is a potentially blinding disease affecting the retinal vessels in premature babies. It is characterized by arrest of the normal process of retinal vessel growth with resultant arteriovenous shunts and development of abnormal new vessels that may eventually lead to tractional retinal detachment and blindness. The disease is detected through a screening program for premature babies who are at risk and involves regular examination of the retina. The guidelines for inclusion in screening programs vary slightly between countries depending on local variations in incidence of ROP and neonatal care, but the infants at highest risk are those of low gestational age (<32 weeks) and low birth weight (<1,500 g). In these infants screening for ROP should start at 4 to 6 weeks after birth and continue at regular intervals until retinal vascularization has reached the temporal periphery (zone 3). The use of wide angle digital imaging has greatly improved our ability to observe and record the course of retinal maturation and document progression of disease, which allows for comparison between patient examinations and better communication between ophthalmologists and other health care providers. Fortunately, in the majority of cases ROP regresses spontaneously; however, in a small percentage the disease will progress with development of severe stages of ROP, with major visual consequences.
Retinoblastoma is the most common malignant tumor of childhood, but it is quite rare at an incidence of 1 in 15,000 live births. Retinoblastoma can be hereditary or nonhereditary. If left untreated, it can be fatal. For retinoblastoma and ROP, one must remember that the earliest diagnosis will produce the most favorable outcome.
 Figure 8.1 Macular Hypoplasia Macular hypoplasia can be seen as an isolated autosomal dominant or autosomal recessive disorder. It may also be seen in association with albinism, aniridia, or other developmental disorders of the eye. The hypoplasia is characterized by the absence of the usual reflection from the macular mound and a poorly developed fovea. Retinal vessels coursing through the central macula are common. In the absence of proper macular differentiation, the blood vessel pattern may not develop properly. Visual acuity is difficult to predict on the basis of macular appearance, but the presence of anomalous vessels that do not respect the horizontal meridian portends a worse prognosis. |
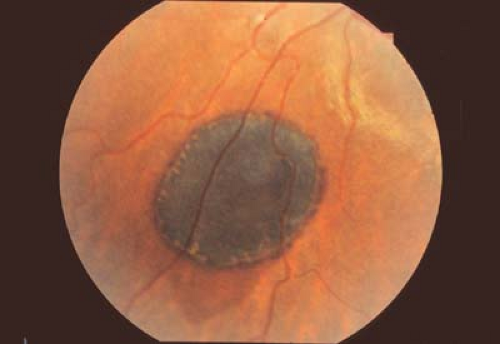 Figure 8.2 Congenital Hypertrophy of the Retinal Pigmented Epithelium (CHRPE) Congenital hypertrophy of the pigment epithelium may be isolated or associated with systemic disorders such as neurofibromatosis (see Chapter 23: Phakomatoses) or familial adenomatous polyposis (FAP). When FAP is associated with benign soft tissue and bony tumors, the condition is called Gardner syndrome. When brain tumors are present, the patient is said to have Turcot syndrome. FAP is associated with a very high risk for colonic cancer. Patients with more than two CHRPE lesions in one eye, bilateral CHRPE, or a family history of colon cancer should be screened with periodic colonoscopy starting in childhood. CHRPE lesions are usually asymptomatic unless the macula is involved. Lesions can be of various size and shape. They may have a hypopigmented ring (shown here) or a “tail.” |
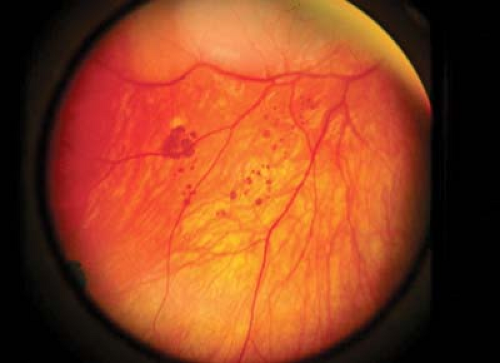 Figure 8.3 Bear Tracks These congenital hyperpigmented areas of the retinal pigmented epithelium are clustered in a pattern that has similarity to the footprints of a bear. They tend to cluster in one quadrant, usually unilaterally, and increase in number and area covered from posterior to anterior. Unlike congenital hypertrophy of the pigment epithelium (Fig. 8.2), they are not associated with systemic disease and usually do not have hypopigmented edges or tails. There may be one or more clusters, each typically with a larger lesion surrounded by one or more smaller lesions. |
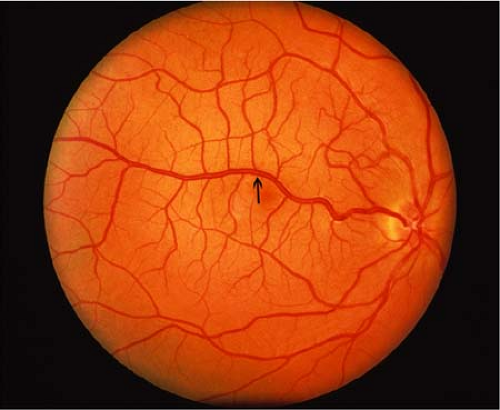 Figure 8.4 Congenital Retinal Macrovessel This rare benign vascular anomaly (arrow) is not associated with leakage or systemic disease (as might be seen in the capillary hemangioma of von Hippel-Lindau disease, Chapter 23: Phakomatoses, Fig. 23.12). Even though these vessels may appear in areas of retina not usually vascularized in this fashion, as shown here, unlike the anomalous vessels of macular hypoplasia (Fig. 8.1), congenital macrovessels are typically associated with normal retinal development and function. |
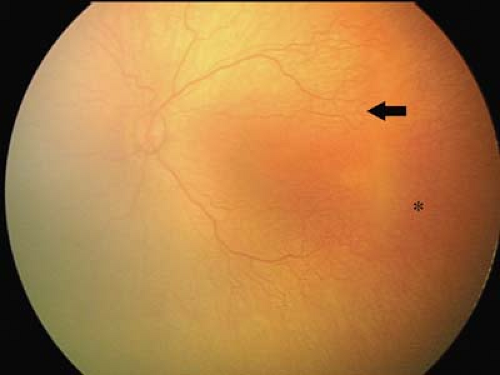 Figure 8.5 Immature Retina The retina is often not fully vascularized until 36 weeks gestation. The nasal retina vascularizes before the temporal periphery. In this premature child, the retinal vessels taper without clear demarcation of the peripheral avascular retina (asterisk). The choroidal vessels visible through the thin avascular retina are easily mistaken for retinal vessels by the inexperienced examiner. The macular area is featureless, the foveal reflex is blunted, and the fovea cannot be located easily. In this case, an arteriovenous loop is visible joining the superior temporal retinal arteriole to the venule (arrow). The extent of vascularization of the retina is just as far as the border of zone 1 and zone 2. According to the International Classification of Retinopathy of Prematurity, the zones of retinopathy of prematurity in the developing retina are as follows: • Zone 1 is a circle centered on the optic disc, the radius of which is twice the distance between the disc and the fovea. • Zone 2 is a circle centered on the optic disc, the radius of which is equal to the distance between the disc and the nasal ora. • Zone 3 is the remaining crescent-shaped area bounded by the outer boundary of zone 2 and the ora serrata, the widest part of which is in the temporal retina. This crescent tapers as it approaches the nasal ora. |
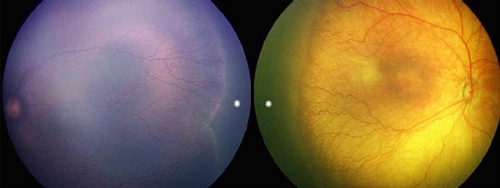 Figure 8.6 Stage 1 Retinopathy of Prematurity in Zone 2 These images demonstrate a demarcation line between vascularized and nonvascularized (asterisk) retina. The left image is that of a darkly pigmented fundus. The right image is that of a Caucasian infant. There is a “hold up” in the normal growth of the retinal vessels. The white line demarcating the extent of retinal vascularization is flat and thin. The vessels posterior to the demarcation line are dilated rather than tapered, and there is prominence of branching just behind the demarcation line. Although no treatment is indicated and the prognosis for resolution is excellent, careful follow-up, perhaps no later than 2 weeks, is required. |
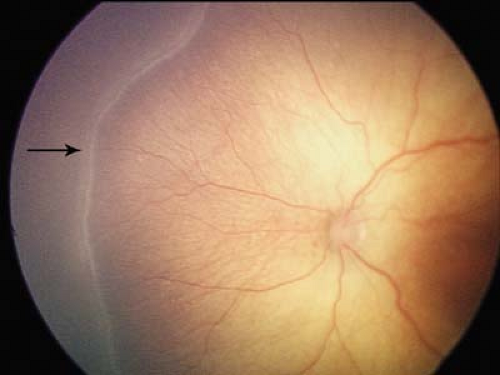 Figure 8.7 Stage 2 Retinopathy of Prematurity (ROP) With progression of ROP the demarcation line will become elevated, gain volume, and form a ridge (arrow). The distinction between stage 1 and stage 2 is much better appreciated in a three-dimensional view of the retina, using scleral depression to look at the ridge in profile (i.e., tangentially). It may be more difficult to distinguish between stage 1 (Fig. 8.6) and 2 on two-dimensional imaging. Note the associated vascular changes including peripheral vessel dilation, tortuosity, and hyperacute branching. Also note the few peripapillary intraretinal hemorrhages as sometimes seen in active disease following examination. |
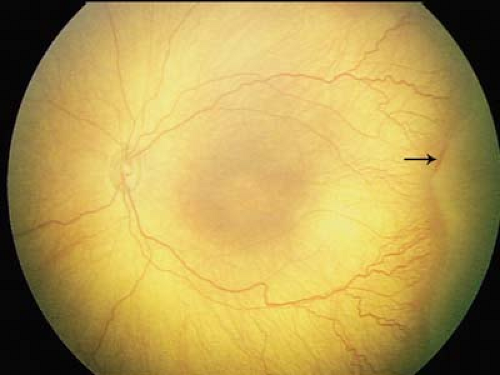 Figure 8.8 Stage 3 Retinopathy of Prematurity—Mild With further progression of disease, there is development of neovascularization within the extra-retinal proliferation. As a result, the extra-retinal proliferation changes color from white to pink and becomes broader. The neovascularization is above the plane of the retina and can extend posteriorly over the retinal surface or centrally into the vitreous. The extra-retinal proliferation can become more irregular in outline with development of neovascularization. There is notable vascular dilation and tortuosity close to the extra-retinal proliferation, which may extend posteriorly to the posterior pole. Stage 3 may be mild, moderate, or severe as defined by the number of clock hours and the degree of neovascularization. Hemorrhage can be seen here along the anterior border of the extra-retinal proliferation (arrow). |
 Figure 8.9 Stage 3 Retinopathy of Prematurity— Moderate As stage 3 becomes more advanced, the neovascularization is more marked and the extra-retinal proliferation more pink in color. The retinal vessels are obscured as they lead up to the extra-retinal proliferation by the posterior extension of extraretinal (i.e., preretinal) neovascularization over the surface of the retina. Note also the increasing dilation and tortuosity of the retinal vessels. |
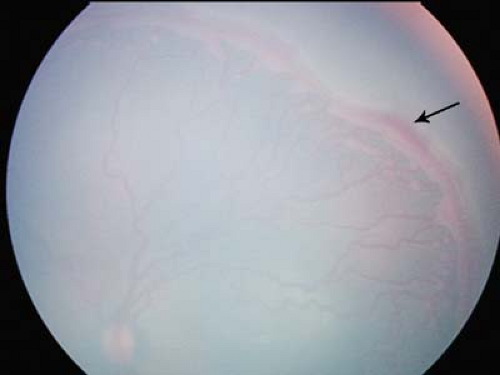 Figure 8.10 Stage 3 Retinopathy of Prematurity (ROP)—Severe This image shows severe stage 3 ROP as characterized by a broad neovascularized extraretinal ridge with a ragged posterior border with clearly visible popcorns (Fig. 8.12). There is hemorrhage along the anterior border of the ridge (arrow). The stage 3 ROP extended for 360 degrees (12 clock hours) in this baby. The retinal vessels in the posterior pole around the optic disc are clearly dilated and tortuous. |
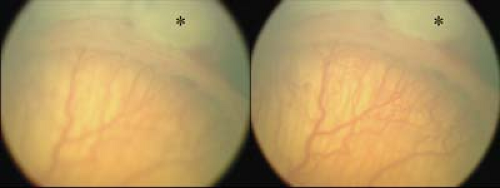 Figure 8.11 Stage 3 Retinopathy of Prematurity (ROP)—Severe These images show high magnification of severe stage 3 ROP. In the left image the photographer has focused on the extraretinal neovascularization, which is above the plane of the retina: The retinal vessels leading up to the extra-retinal proliferation are not in focus. In the right image of the same area the photographer has focused on the retinal vessels behind the extra-retinal proliferation, and therefore the neovascular extra-retinal proliferation is out of focus. The white area anterior to the extra-retinal proliferation (asterisks) shows the near confluent diode laser treatment to the vascular retina. |
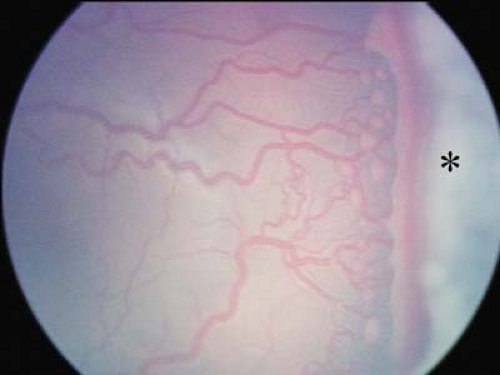 Figure 8.12 “Popcorn” Retinopathy of Prematurity (ROP) “Popcorn” ROP is a term used to refer to isolated clumps of new vessels posterior to the ridge. They are clearly seen to be on the surface of the retina and obscure the underlying retinal vessels. Development of “popcorn” may be seen in association with stage 2 ROP. The clumps may coalesce and eventually result in progression to stage 3. Popcorns can also occur later in the course of ROP and be associated with the regression phase and peripheral advancement of stage 2. In this image, the popcorns are seen posterior to an area of severe stage 3 associated with some bleeding along the neovascular extra-retinal proliferation. Near confluent laser treatment was applied to the avascular retina (appearing here as white areas, asterisk) and resulted in regression of the disease. |
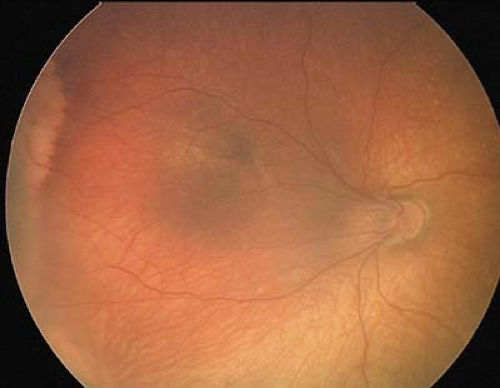 Figure 8.13 Stage 4a Retinopathy of Prematurity (ROP) Following diode laser treatment in this eye with severe ROP, regression of the acute neovascular process was achieved. However, there is significant cicatricial change with resultant straightening of the temporal vascular arcades and temporal ectopia (“dragging”) of the fovea. In the more peripheral inferotemporal retina (bottom left section of image), the retina is elevated (and out of focus). Stage 4a ROP is defined by this partial retinal detachment not involving the macula. In this case, the retinal detachment improved spontaneously without any treatment. |
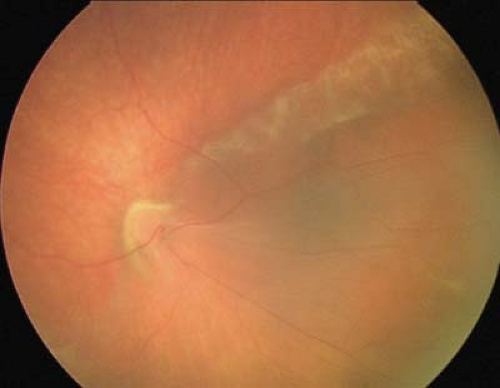 Figure 8.14 Stage 4b Retinopathy of Prematurity (ROP) In stage 4b ROP, the partial retinal detachment involves the macula. Note the significant cicatrization and temporal dragging of both temporal and nasal vessels and tractional retinal detachment, which has involved the fovea. The macular architecture is almost unrecognizable and the fovea can no longer be clearly identified. The visual prognosis for stage 4b ROP is very poor, with significant risk of progression to further retinal detachment over time without surgical intervention. |
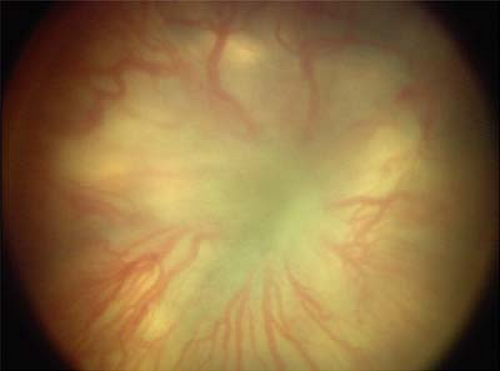 Figure 8.15 Stage 5 Retinopathy of Prematurity (ROP) In stage 5 ROP, the retina is completely detached. Note the marked dilation of the retinal vessels and obscuration of the optic disc due to the funnel-shaped total retinal detachment. The retina has a glassy appearance. Progressive fibrosis will result in closure of the funnel over time. This degree of severity of disease is no longer amenable to laser treatment, and surgical treatment to release tractional retinal detachment by vitrectomy is often not successful. The visual prognosis is dismal. |
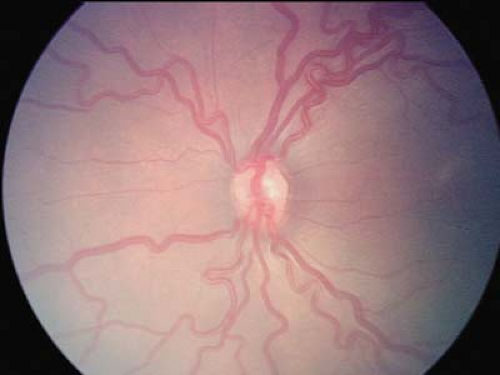 Figure 8.16 Retinopathy of Prematurity (ROP)—Plus Disease
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|