Retained Lens Material
Robert C. Wang
Dwain G. Fuller
William L. Hutton
The loss of lens material using extracapsular techniques has become less frequent with modern methods. Phacoemulsifcation with multiple ultrasound settings and various irrigation/aspiration tips has simplified the removal of nuclear and cortical material. In high-risk cases such as pseudoexfoliation syndrome, the additional use of capsular tension rings has made lens extraction in these patients much safer than in the past.
Despite these advances, posterior capsular rupture and lens loss into the vitreous cavity still occur. Multiple complications can result, severely compromising final visual acuity. Corneal edema secondary to high phacoemulsification power and inflammatory glaucoma can impair vision and impede posterior segment evaluation. Loss of endothelial cells can cause permanent corneal edema, necessitating future corneal transplantation. Iris adhesions from secondary inflammation may also occur as can iris capture from sulcus or anteriorly placed intraocular lenses. Frequently, complicated surgery with the loss of lens material posteriorly results in cystoid macular edema. More significantly, vitreoretinal traction from disruption of the posterior capsule with vitreous presenting into the anterior chamber can result in retinal tears and detachments, which may lead to significant visual loss.
INCIDENCE
Extracapsular surgery, specifically modern phacoemulsification and small incision techniques has led to excellent visual results and rapid patient recovery. Posterior capsular rupture does still occur with a reported incidence of 1.9%.1 However, not all cases of posterior capsular rupture is associated with lens loss. With modern techniques, posterior capsular rupture tends to occur during the irrigation and aspiration phase, after which the majority of lens material has been removed. However, breach of the posterior capsule early in the procedure often leads to luxation of lens material into the vitreous cavity, starting a cascade of complications unless the problem is corrected. Zonular rupture may result in loss of an essentially complete lens posteriorly. Although the exact incident of retained lens material in all cases of posterior capsular rupture is uncertain, older data estimated the rate to be up to 4%.2 Possibly because of better techniques, a large case series has a lower reported incidence of 0.20%.3
IMMUNOPATHOLOGY OF RETAINED LENS MATERIAL
The anterior chamber and eye itself are unique in that they are relatively immune privileged. Under normal conditions, there is minimal ocular immune surveillance due, in part, by the blood–eye barrier. After eye injury, however, blood vessels become incompetent and an immunologic response occurs. Early in the response, there is the immediate but transient presence of neutrophils. Next follows a cell-mediated inflammatory response, mainly of T lymphocytes and macrophages. T cells are, however, antigen specific, binding to their specific antigen and releasing cytokines that are cytotoxic to target cells. Macrophages, however, are not antigen specific and attack targeted cells through their phagocytic properties. Additionally, macrophages have an important role in antigen presentation, cytokine secretion, and cytotoxicity.
The immunopathology of lens-induced uveitis remains to be completely elucidated. It is thought that the mechanism maybe a delayed hypersensitivity reaction rather than a rejection of antigenic tissue. Macrophages predominate in the inflammatory reaction from retained lens material. They appear to be activated, then mediate and amplify the immune reaction. Epithelioid and giant cells can be formed as well as phacolytic cells, (macrophages with ingested lens material). Histiologic studies of vitreous specimens in eyes with luxated lens material have shown no macrophage response three days after lens loss. The inflammatory response gradually increases, and by 90 days, 80% of cases demonstrated a macrophage response. The increase in response is linear up until 28 days. After 90 days, there seems to be a decrease in this response.4,5
MANAGEMENT BY THE ANTERIOR SEGMENT SURGEON
Loss of lens material can occur even in the hands of an experienced cataract surgeon. The surgeon’s quest for immediate patient satisfaction and prompt visual improvement can influence surgeons to proceed with aggressive attempts to remove dislocated lens material. Fishing in the vitreous cavity in the attempt to remove lens fragments is often an invitation for disaster. Similarly, aggressive attempts to irrigate lost lens material anteriorly can cause retinal tears and bleeding.
Cortical material is typically easier to manage and smaller in nature than nuclear material when lost. Small cortical particles that are lost posteriorly during the irrigation and aspiration phase can generally be left in place although the patient must be monitored for an inflammatory reaction and development of cystoid mocular edema (CME). Impending loss of larger cortical fragments can sometimes be prevented by injection of viscoelastic material under the fragment to inhibit posterior dislocation. This allows not only lenticular support, but also displaces the vitreous posteriorly to allow safe removal of the lens material with minimal vireo-retinal traction. Additionally, decreasing the irrigation rate maybe helpful in reducing hydration of the vitreous and minimize prolapse of the vitreous into the anterior chamber and posterior migration of lens particles.
Management of dislocated nuclear lens material or, more typically, the lens in toto is much more difficult. Major loss of nuclear material or the entire lens occurs early in the procedure from either loss of a continuous curvilinear capsularrhexis with posterior capsular rupture or zonular dehiscence. Commonly, the anterior segment surgeon has little time to stabilize the larger lens piece as it sinks posteriorly out of view. Unfortunately, nuclear material in the vitreous cavity is associated with an increased risk of inflammation, glaucoma, and corneal decompensation. If the nuclear material is still within the iris or lens capsular plane, stabilization with a combination of a viscoelastic and a secondary instrument inserted underneath the particle can allow enough time to prevent posterior dislocation. Occasionally, the lens can then be lifted and placed in the peripheral anterior chamber angle, allowing time to make a limbal incision to remove the larger lens fragment. Care must be taken to facilitate a complete vitreous removal from the anterior chamber and entry incision wound. Typically, the vitreous cutter can be inserted safely to just below the iris plane to faciliate vitreous clean up and reduce the risk of vitreoretinal traction during intraocular lens insertion. If enough capsular support remains, placement of the intraocular lens in the bag or sulcus is desirable. Otherwise, placement of anterior chamber intraocular lens may be elected. Although, there is evidence that final visual acuity with posterior chamber lenses may be slightly better statistically than with anterior chamber lenses.6,7,8,9
If lens material is lost below the iris/lens plane, aggressive retrieval is not advisable. Attempts to aspirate lens material with the phacoemulsification tip in the vitreous cavity is not recommend and is fraught with complications.10 If one has immediate access to a vitreoretinal surgeon, pars plana retrieval at the time of the complication may be possible.3,9 Some authors have advocated a pars plana approach by the cataract surgeon to stabilize dislocated nuclear material with either a secondary instrument or viscoelastic material.11 Unfortunately, many anterior segment surgeons may not have extensive training in pars plana manipulation and its potential complications. Additionally, despite promising reports, case series are still small, and it is difficult to determine if aggressive retrieval of lens material through a pars plana approach by a anterior segment surgeon should be recommended at this time.
A preferred approach would be to place the intraocular lens if possible, remove those particles readily accessible, and then close the eye. In those circumstances where there is a vitreoretinal surgeon readily available and the operating room is suitability equipped, definitive removal of dislocated lens material can be accomplished. However, in most instances it is best to discuss the problem with the patient and refer the patient the next day for further evaluation.
We recommend that at the conclusion of a complicated cataract surgery a subconjunctival injection of a short-acting steroid to minimize the inflammatory response and cystoid macular edema. Frequent postoperative topical steroids, antibiotics, and cycloplegics should be initiated.
POSTOPERATIVE EVALUATION
Early postoperative evaluation can be difficult due to the presence of corneal edema. Additionally, intraocular pressure may be elevated because of lens material, or more typically, remaining viscoelastic material. Incision wound integrity should be carefully inspected, particularly if the intraocular pressure is low. The presence of vitreous strands incarcerated into the cataract wound can act as a source for endophthalmitis or cystoid macular edema. Intraocular lens placement with a poorly supported capsule can lead to phacodonesis and possible intraocular lens dislocation into the vitreous cavity. Cortical material can become very flocculent and mimic a pseudo-hypopyon in the anterior chamber.
Despite these potential problems, early evaluation of the posterior segment is invaluable in assessing retinal complications after surgery and determining the timing of definitive surgery. Frequently, the view is compromised because of corneal edema, miotic pupils, and lens particles. Ultrasonography can readily identify the amount of nuclear and cortical material present in the posterior segment. Cortical material typically produces a snowstorm appearance on ultrasonography, with larger pieces demonstrating irregular borders deposited inferiorly (Fig. 1). Nuclear material typically is found inferiorly and not suspended in the vitreous and is acoustically denser with more regular borders (Fig. 2). Ultrasonography can also identify areas or vitreal-retinal traction, retina tears, or retina detachment not otherwise easily discernable on funduscopic examination.
 Fig. 1 Contact B-scan ultrasonogram demonstrates snowstorm appearance of the vitreous from greater amounts of lens material than suspected on clinical examination. |
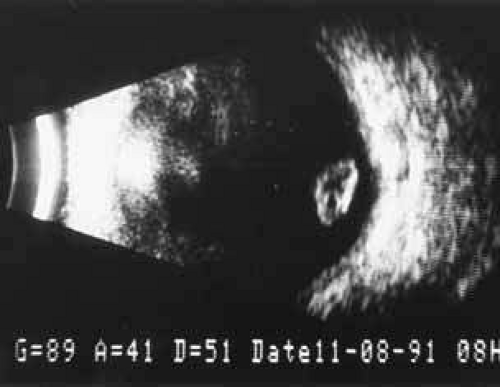 Fig. 2 Contact B-scan untrasound shows nuclear fragment in the inferior periphery of the vitreous cavity in an eye with chronic low-grade inflammation and macular edema. |
SEQUELAE OF RETAINED LENS FRAGMENTS
BULLOUS KERATOPATHY
Corneal edema can occur after phacoemulsification even without the presence of retained lens material (Table 1). Loss of endothelial cells from high phacoemulsification power can result in persistent, pseudophakic bullous keratopathy. Additionally, retained lens material and uveitis can result in elevated intraocular pressure contributing to further corneal decompensation. Treatment consists of management of the underlying condition. Topical steroid therapy aids in decreasing the inflammatory response. A multitude of topical pressure lowering agents now exist to control elevated intraocular pressure. Oral carbonic anhydrase inhibitors can be added to topical regimens to lower intraocular pressure in recalcitrant cases. However, in 10% of cataract surgeries complicated by retained lens material, corneal edema will persist often requiring a penetrating keratoplasty.9,12,13,14,15
TABLE 1. Complications From Retained Lens Fragments Following Phacoemulsification
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|
|---|