12 Jay S. Pepose and Mujtaba A. Qazi The treatment of dry eye disease in a refractive surgery patient can be a dialectically rewarding and challenging experience. Many candidates who present for refractive surgery manifest dry eye of varying degrees and causes. This cohort is preselected in a sense because sicca syndrome is a leading cause of contact lens intolerance.1 Without proper assessment and treatment of preexisting dry eye and associated ocular surface changes, a superimposed laser in situ keratomileusis (LASIK)-induced neurotrophic keratopathy2 can compound the preoperative condition.3–6 Typically, this occurs during the early postoperative period, when the patient is most acutely aware of visual and ocular symptoms, frequently anxious about possible long-term effects, and often not reticent to voice complaints. If their concerns about dry eye are not appropriately addressed both preoperatively and postoperatively, these patients may seek alternative medical, or possibly, legal opinions. It is our goal to provide a practical, evidence-based approach for the refractive surgeon and eye care professional caring for refractive surgery patients with dry eye. This chapter encompasses (1) preoperative assessment, testing and treatment of dry eye disease; (2) intraoperative management based on the compendium of effects of refractive surgery on both tear film homeostasis and the ocular surface; and (3) a logistical postsurgical management algorithm. Given the current trends regarding refractive surgery, we focus primarily on LASIK, laser subepithelial keratomileusis (LASEK), and photorefractive keratectomy (PRK). In a 2002 study, dry eye symptoms were present preoperatively in 38% of 450 consecutive patients undergoing myopic LASIK.7 The Japanese Dry Eye Association8 criteria for dry eye are as follows: Using these criteria, 35.2% of LASIK patients met both sets of dry eye criteria preoperatively and an additional 41.2% met one set.9 Thus, 76.4% of LASIK candidates in this series had dry eye or presumed dry eye, as defined. Other studies have reported low Schirmer’s 1 test scores in 43% of myopic patients who underwent PRK.10 The manifestations of dry eye disease include ocular fatigue, dryness, foreign body sensation, grittiness, irritation, burning, red eye, heavy eye feeling, and other symptoms.11 In most cases, these symptoms are chronic and intermittent. Dry eye symptoms are frequently worse as the day goes on and can be exacerbated by environments with low humidity, such as on long airplane rides. Activities that involve relative suppression of blinking, such as computer work, movie watching, or highway driving, can also aggravate ocular dryness.
Refractive Surgery and Dry Eye Disease
Key Points
♦ Preoperative Prevalence of Dry Eye Disease
♦ Preoperative Assessment
Patient History and Risk Factors
|
Dry eye disease is associated with a female predominance, with symptoms more common in middle age or later (Table 12-1). There may be associated xerostomia and evidence of autoimmune disease, such as polymyalgia rheumatica, systemic lupus erythematosus, scleroderma, or fibromyalgia (i.e., Sjögren’s syndrome). In patients with severe Sjögren’s syndrome, there may be reduced or absent reflex tearing and, often, a history of scant production of emotional tears. A subset of women with Sjögren’s syndrome may have an associated androgen deficiency,12 which appears to play a critical role in lacrimal and meibomian gland homeostasis. There may be an additional risk of dry eye in patients taking hormone replacement therapy, particularly estrogen alone.13
Clinicians should be particularly alert to patients who complain of contact lens intolerance, as this may be suggestive of dry eye disease and requires preoperative treatment. Of patients diagnosed with dry eye, 20 to 30% are contact lens wearers.14,15 Contact lens wear is associated with reduced corneal epithelial oxygenation, increased mucus production, and reduced blink frequency and efficiency. Contact lenses can also provide a depot for tear film cytokines to access the ocular surface. Long-term contact lens use may be associated with decreased corneal sensation, which may be compounded by the transient decrease in sensation typically seen following LASIK surgery.
A pertinent medical history includes conditions that may be associated with neurotrophic keratitis, such as herpes simplex keratitis, zoster ophthalmicus, fifth nerve palsy, diabetes mellitus, and multiple sclerosis. Patients with preexisting symptomatic neurotrophic keratitis would generally be considered at high risk for dry eye following LASIK surgery, as the condition could be worsened by the corneal denervation produced by flap creation and laser ablation. Patients with diabetes may also have decreased corneal sensation and goblet cell density, lower tear volume and quality, and a higher incidence of epithelial defects and erosions following LASIK surgery than age-matched nondiabetic controls.16,17
Blepharitis and meibomian gland dysfunction can lead to evaporative loss of tears. Acne rosacea may be accompanied by meibomian gland inflammation and atrophy. Frequently, the patient is unaware of the underlying rosacea blepharitis, and the ophthalmologist should have a heightened awareness of the clinical signs of this condition, described below.
Ocular Signs
Patients with aqueous tear deficiency have a decreased tear lake. There may be excessive debris in the tear film. In patients with dry eye disease, the Schirmer’s 1 test result is decreased (usually no more than 5 mm with proparacaine) and tear BUT is reduced to 5 seconds or less. The ocular surface may stain with vital dyes such as lissamine green and rose bengal, generally on the inferior cornea and conjunctiva (Fig. 12-1). More severe dry eye disease may also be associated with fluorescein staining of the cornea and bulbar conjunctiva, seen initially inferiorly and then progressing to include more of the interpalpebral ocular surface.
Inspissated and stenosed meibomian glands (Fig. 12-2) can lead to abnormalities of the lipid layer. Bacterial colonization may further alter the outer tear lipid layer through the action of bacterial lipases. Signs of acne rosacea include telangiectasia and sebaceous gland hyperplasia on the nose and malar region (Fig. 12-3). This may be accompanied by eyelid telangiectasis (Fig. 12-4), conjunctival injection (a result of increased tear cytokines and decreased tear clearance18), and meibomianitis. Incomplete lid closure, lagophthalmos, exophthalmos, ectropion, incomplete blink, and large interpalpebral fissure width with excessive sclera showing should be warning signs of potential associated dry eye. Conjunctivochalasis can also be associated with dry eye and may increase the risk of poorer microkeratome suction or gear jamming during the microkeratome pass.19
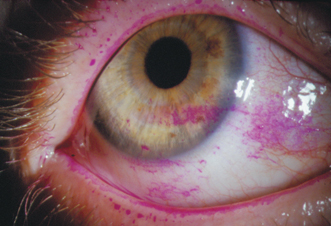
Figure 12-1 Rose bengal staining of mucus, debris and devitalized epithelial cells is observed in the inferior cornea and bulbar conjunctiva of a patient with Sjögren’s syndrome.
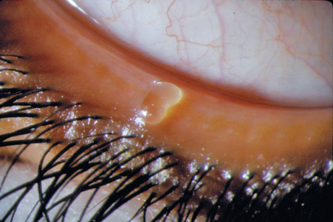
Figure 12-2 Approximately 30% of patients with dry eye disease have concurrent eyelid disease,15 which contributes to ocular discomfort and rapid aqueous evaporation. Plugged and inspissated meibomian glands are seen here, with collarette accumulation at the lash bases.
Just as older age is a risk factor for dry eye disease, it also is a risk factor for development of an epithelial defect during LASIK surgery (odds ratio 2.39 per decade). Other risk factors include thicker corneas, not breaking microkeratome suction on the reverse pass, and overuse of anesthetic drops preoperatively.20 It is possible that the shearing force of the microkeratome overwhelms the adhesion between the corneal epithelium and basement membrane in patients with dry eye disease because of a higher coefficient of friction, just as there may be greater compression and appositional force against the microkeratome in patients with thicker corneas. Patients with map-dot-fingerprint dystrophy (Fig. 12-5) have duplication of corneal basement membranes associated with abnormalities in anchoring fibrils and the basement membrane adhesion complex. This dysadhesion between corneal epithelium and the thicker, multilaminated basement membrane also greatly increases the risk of epithelial defects or sloughing during the micro-keratome pass, and these dystrophic patients are better candidates for PRK than LASIK.21 Epithelial defects are associated with a 24-fold increase in the incidence of diffuse lamellar keratitis following LASIK surgery.22

Figure 12-3 Small blood vessels are visible in the nasal and malar skin in this patient with acne rosacea, giving a ruddy or blushed complexion. Over time there can be hypertrophy of sebaceous tissue, progressing to swelling and growth of the nasal (rhinophyma) and central facial skin.

Clues suggestive of dry eye may be obtained during diagnostic testing for refractive surgery. Multiple white spots on topographic maps (Fig. 12-6) may reflect localized areas where the placido rings are markedly distorted because of a dry ocular surface, obviating computerized analysis in those regions. Taking advantage of topographic changes in surface regularity and asymmetry seen in patients with dry eye disease, rapid sequential topographic image analysis serves as the basis for a new noninvasive test for dry eye.23,24 Wide variation in sequential wavefront measurements, increased higher-order aberrations,25–27 and fluctuation in visual acuity measurements may also be suggestive of dry eye. It is best to treat these patients,19,28 rehabilitate the ocular surface, and retake the topographic and wavefront measurements before primary refractive surgery or retreatment.
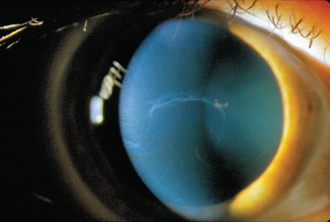
Figure 12-5 Geographic opacities in the cornea, reflecting duplication of the epithelial basement membrane in anterior basement membrane dystrophy, increase the risk for epithelial defects during and after LASIK surgery, especially in patients with dry eye disease.
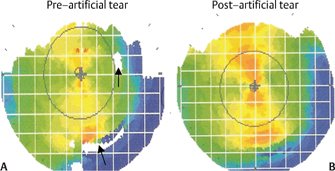
Figure 12-6 Areas of placido disk distortion (arrows) due to focal corneal drying (A) in an axial topographic map become more regular following application of an artificial tear drop (B).
♦ Effect of Dry Eye Disease on Refractive Surgery Outcomes
Preexisting dry eye disease with supravital dye staining of the ocular surface represents a risk factor for chronic dry eye postoperatively.6,9,29 Chronic dry eye after LASIK is associated more frequently with female gender, preoperative dry eye symptoms, preoperative corneal staining, diminished preoperative tear volume and stability, decreased corneal sensation, higher attempted correction, and greater ablation depth. Tear secretion and corneal sensation are significantly more depressed following LASIK in long-term contact lens wearers than nonwearers.5 There was a report of a LASIK patient who had a retained contact lens embedded in the superior cul-de-sac for 10 years that was discovered intraoperatively at the time of LASIK enhancement.30 This case emphasizes both the decreased corneal sensation that can be associated with chronic contact lens use, and the utility of searching for retained contact lenses using double-lid eversion.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


