and Yi Ning J. Strube2
(1)
Wright Foundation for Pediatric Ophthalmology and Adult Strabismus Medical Center, Los Angeles, CA, USA
(2)
Queen’s University, Kingston, Ontario, Canada
Keywords
Rectus muscle resectionSingle-suture resectionDouble-suture resectionWright plicationWright mini-plicationModified rectus tuckAnterior segment circulationThe two most useful rectus muscle tightening procedures are the rectus muscle resection and the rectus muscle plication. Rectus muscle tucking has not proven reliable, as it tends to loosen over time. A tuck is a muscle-to-muscle union. Because the muscle fibers are longitudinal and the transverse fibers are weak, the sutures tend to pull out and slip. The rectus muscle plication, however, involves securing posterior muscle to sclera, and this procedure is as stable as a resection.
14.1 Rectus Muscle Resection
Muscle resections can be done as a single-suture or double-suture procedure. The single-suture technique is preferred by the authors because it is simple, fast, and accomplishes the same anatomic goals as the double-suture technique. One key to the single-suture technique is to place a security knot in the center of the muscle to prevent unraveling of the suture if one of the sutures is inadvertently cut or broken. Proponents of the double-suture technique prefer two sutures for greater security against a lost muscle and for better support of the middle of the muscle.
14.2 Single-Suture Resection: Fornix Approach
Plications and resections can be performed through either a fornix or limbal incision. Figures 14.1, 14.2, 14.3, 14.4, 14.5, 14.6, and 14.7 demonstrate the technique for single-suture resection using a fornix approach.
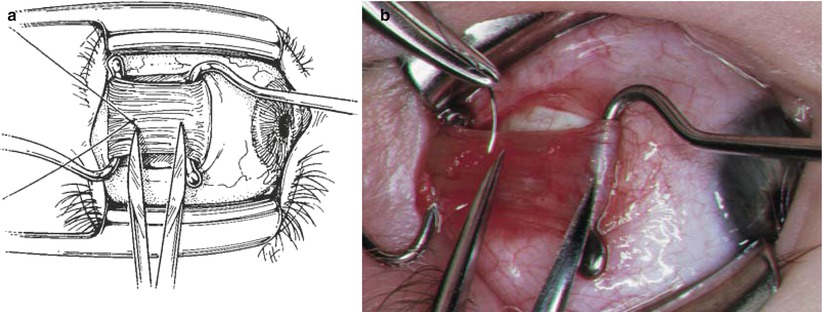
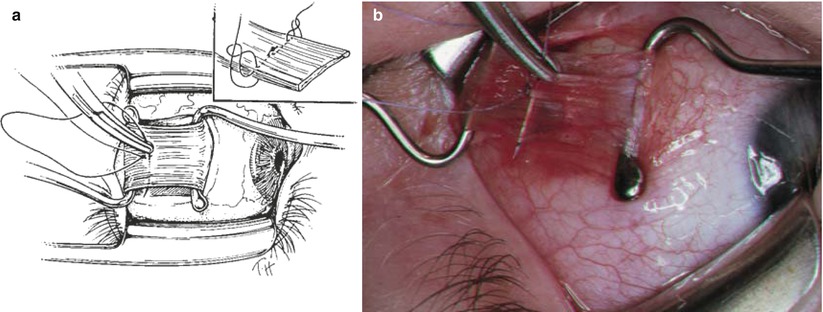
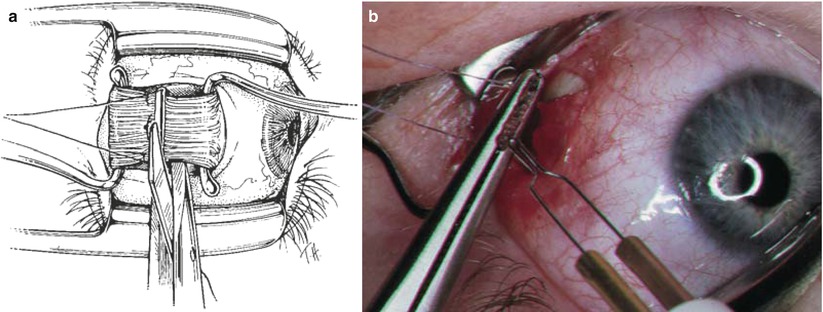
Fig. 14.1
The left lateral rectus (LR) muscle is isolated in the standard manner through a fornix incision (Surgeon’s view). A posterior dissection, including the intermuscular septum and check ligaments, is performed to approximately 3 mm posterior to the planned muscle resection (see Figs. 10.9 and 10.10 for posterior dissection technique). The anterior Tenon’s capsule is removed in front of the muscle to expose bare sclera
Fig. 14.2
(a) Two large Jameson hooks are inserted under the muscle belly. One hook is placed at the insertion (handle directed nasally), and the other is placed posteriorly deep in the fornix (handle directed temporally). Keep the posterior hook against sclera and avoid the temptation to pull the hook up to obtain more muscle. Pulling the hook off sclera does not gain access to posterior muscle; it only stretches the anterior muscle, which is already exposed. A security knot is placed through the center of the muscle belly. (b) The photograph shows that the calipers are placed at the center of the Jameson hook and posteriorly, to mark the location of the security knot. A 5–0 Vicryl double-arm suture is used to secure a central 2-mm area of muscle (full muscle thickness). Notice that the needle is placed approximately 0.5–1 mm posterior to the desired resection point. This places the security knot behind the resection point, which helps to protect the knot. The sutures are tied together in a tight square knot. If one of the sutures inadvertently breaks, this knot will secure the muscle and prevent the suture from completely unraveling
Fig. 14.3
(a) One of the needles connected to the security knot is passed at half-muscle thickness, entering just anterior to the knot. This pass extends half thickness until it exits at the muscle edge. A full-thickness locking bite is then placed through 2 mm of the muscle edge, directly behind the half-thickness suture. Using the other end of the suture, the same suture pass is performed on the other half of the muscle to secure both sides of the muscle. The inset shows the suture path with locking bites at each edge of the muscle, and a security knot in its center. (b) The photograph shows the needle being passed at half-thickness through the superior aspect of the lateral rectus muscle, just anterior to the security knot. Keep the needle pass parallel to the hooks, because the tendency is to slant the pass anteriorly, reducing the resection
Fig. 14.4




(a) The muscle has been secured with 5-0 Vicryl suture, by placing locking bites at each edge of the muscle, as well as a central security knot. The muscle is then cross-clamped with a Hartman clamp, anterior to the sutures. Next the muscle is excised anterior to the Hartman clamp, flush to the surface of the clamp. (b) The photograph shows cautery being applied to the muscle stump. Note the sutures being pulled posteriorly in order to avoid the cautery. Be careful, because the sutures will melt and weaken if they get close to the cautery. After cautery, the muscle is released from the Hartman clamp (Note: The authors do not routinely clamp and cauterize the lateral rectus muscle, as it does not hemorrhage significantly after being resected)
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
