FIGURE 39.1 Lateral neck reconstruction with an anterolateral thigh free flap. A. A 17-year-old male with melanoma. B. Planned skin resection. C. Resection. D. Reconstruction with anterolateral free flap.
HISTORY
The majority of defects involving loss of the skin of the neck or scalp are usually the result of the resection of cancers of the skin, trauma, or burns. For cancer of the skin, reconstruction is initiated once surgical margins are clear. This often can be accomplished in a delayed manner, such as within a few days after Mohs surgery, or more immediately in the operating room after frozen sections are negative. Traumatic loss of the scalp, unless the underlying dura is exposed, should be reconstructed with the goals of minimizing the number of scalp incisions, creating a stable wound that will allow eventual expansion of the scalp tissue, and placing any incisions necessary for acute coverage so that they do not interfere with the blood supply of regional flaps (Fig. 39.2) or the secondary placement of tissue expanders. Prior radiation therapy to the surgical field can negatively affect local wound healing. Thus, in addition to understanding the TNM stage of the cancer, the surgeon should obtain the history of any previous treatment with radiation therapy and anticipate the possible need for postoperative radiation therapy.
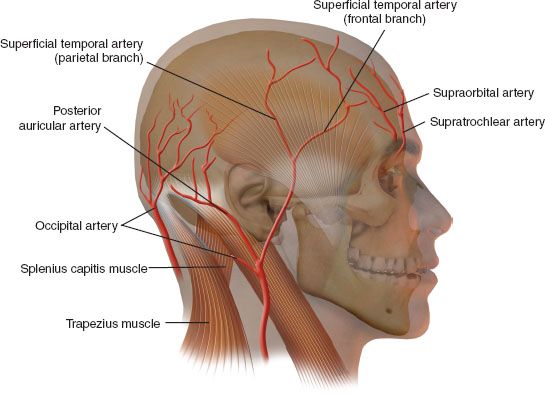
FIGURE 39.2 Regional blood supply for scalp reconstruction. Scalp flaps should be designed to capture regional axial blood supply in their base. Optimal, secondary reconstruction usually requires tissue expansion.
PHYSICAL EXAMINATION
The physical examination should focus on defining the extent of the defect. The following questions should be addressed:
• What are the expected dimensions (i.e., surface area and volume) of the defect?
• What critical underlying structure will be exposed (i.e., bone, periosteum, vessels, facial nerve)?
• What regional blood supply will remain after the resection (i.e., what identifiable arteries will be resected, such as the superficial temporal, supraorbital, facial artery) that would support regional flaps?
• Will a neck dissection be needed, and if so, where will the incisions for the neck dissection be placed so that they do not interfere with flap design?
INDICATIONS
The indications for reconstruction of the lateral neck defect are any defect that cannot be closed primarily or where the risk of skin breakdown and great vessel exposure is significant.
CONTRAINDICATIONS
Free tissue transfer is often a better choice for reconstruction if the surgical site has received prior radiation. Comorbidities, such as severe cardiovascular or peripheral vascular disease, may guide one to choose a regional flap instead of a microvascular flap. Transposing or rotating regional flaps that have been previously in an irradiated field likely place the reconstruction at risk for wound dehiscence. In a similar manner, if a surgical extirpative site is expected to receive postoperative radiation therapy, regional flaps or free flaps (vs. the use of skin graft) likely reduce the risk of osteoradionecrosis since the bone is being covered with well-vascularized tissue.
PREOPERATIVE PLANNING
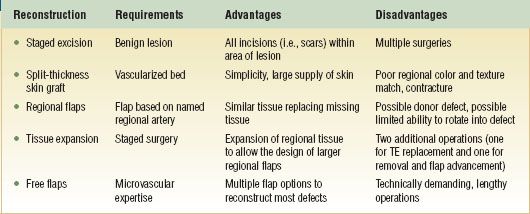
Once the extent of the expected defect has been anticipated and defined, preoperative planning now involves determining the various ways to reconstruct the defect with an understanding of the respective requirements, advantages, and disadvantages of each method (Table 39.1). Whether the defect is caused by a malignant lesion (i.e., cancer of the skin), a benign lesion (i.e., nevus), or a traumatic injury will also affect the choice of reconstruction. Methods of reconstruction will include staged excisions, adjacent tissue transfer (i.e., rotation–advancement flaps with a random blood supply), regional flaps, regional flaps combined with tissue expansion, and free flaps. To ensure the greatest vascularity, one should design the chosen regional flap so that its base contains a regional artery. This can be confirmed with a Doppler examination if there is any doubt about the regional blood supply.
SURGICAL TECHNIQUE
Staged Excisions
Staged excisions are most suited for large benign lesions, usually congenital nevi, of the neck or scalp. The first surgery involves removing approximately 60% to 80% of the original lesion and placing the entire excision within the borders of the original lesion. For lesions of the neck, one should try to place the final orientation of the scar in a natural skin crease (Fig. 39.3). After the first surgery, some spreading of the scar can be expected.

FIGURE 39.3 Staged neck excision. A. Vertically oriented nevus to be excised in stages. The goal is to place the final closure in a natural skin crease. B. First stage. C. Six months after first stage. D. One month after second stage.
The advantages of a staged excision should be compared to the possibility of doing tissue expansion. Many staged excisions of lesions of the scalp will be associated with some scar alopecia at the closure site. Thus, tissue expansion is often offered as an additional way to remove the lesion with the possibility of less scar spreading. However, expansion requires approximately 2 to 3 months between surgeries while the expander is being inflated, and some patients either do not want or cannot make weekly appointments for expansions.
Skin Grafts
Skin graft reconstruction of the neck or lateral scalp is usually done only as a temporizing measure. Skin grafts are placed acutely with the goal of creating a healed wound but with the long-term expectation that they will be removed and replaced with local tissue (Fig. 39.4). Grafts are usually harvested as split-thickness grafts with an approximate thickness of 0.014 inch in adults. In children, grafts are thinner with thicknesses that ranging from 0.008 to 0.014 inch. Because of the similar color match, the scalp is an excellent source of skin grafts for the face or neck. Skin grafts must be placed on an underlying bed of well-vascularized tissue. Periosteum will support a split-thickness skin graft. Cranial bone must be partially decorticated to allow granulation prior to placing a skin graft. A vacuum-assisted closure (VAC) can be used to promote granulation tissue prior to placing a skin graft (Fig. 39.4). For scalp defects once the skin graft has healed and there is no longer an open wound, tissue expanders are placed with the goal of replacing the skin grafts with the surrounding scalp once it has been expanded.
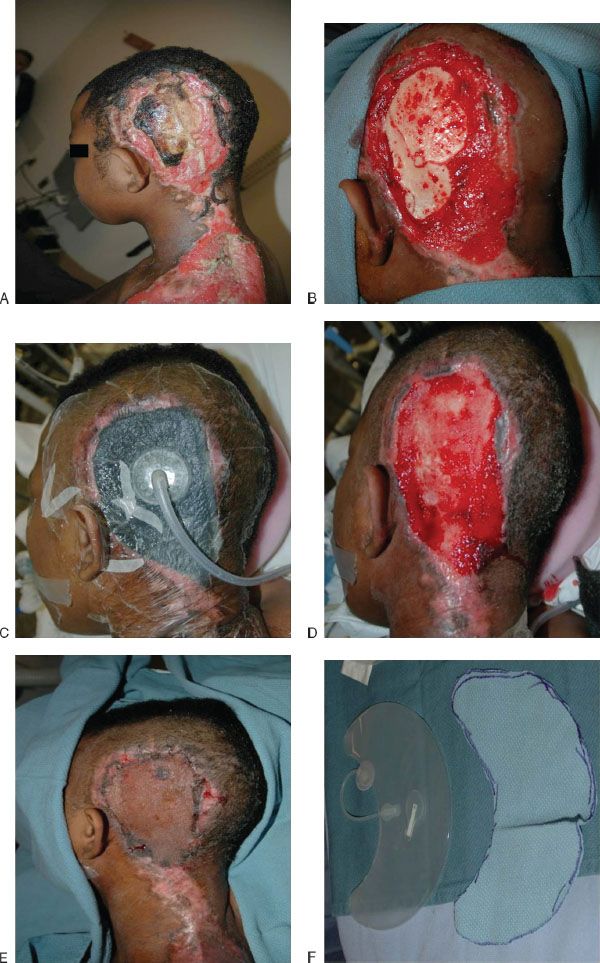

FIGURE 39.4 Multistage scalp reconstruction with skin grafts, VAC, and expanded scalp flaps. A. Full-thickness burn of lateral scalp to bone. B. Outer table drilled to allow cortical bleeding. C. VAC in place. D. Three weeks of VAC therapy. E. One week after split thickness skin graft. F. Tissue expander to be placed with template. G. After 2 months of expansion. H. Tissue expander removed with scalp flap raised. I. Scalp flap rotated to replace excised skin graft. J. Lateral view, 3 years postinjury. K. Posterior view, 3 years postinjury.
Regional Flaps
Regional flaps of the lateral skull are designed on the regional blood supply, in particular the supraorbital, superficial temporal, and/or postauricular artery (Fig. 39.2). These are rotation–advancement or transposition flaps that are designed to cover the defect. At the same time, their movement often leaves a donor defect that needs skin grafting (Fig. 39.5
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


