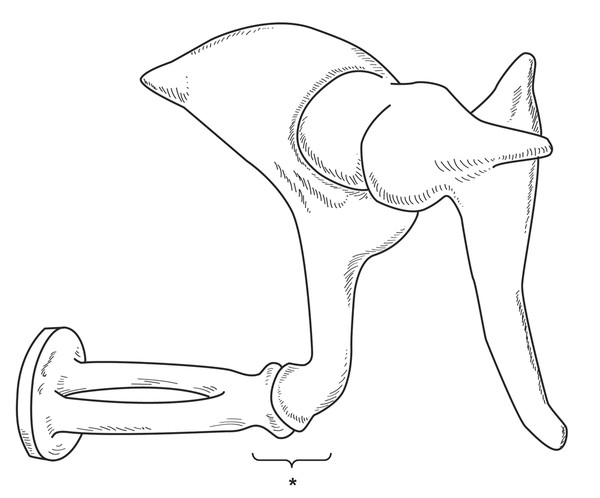
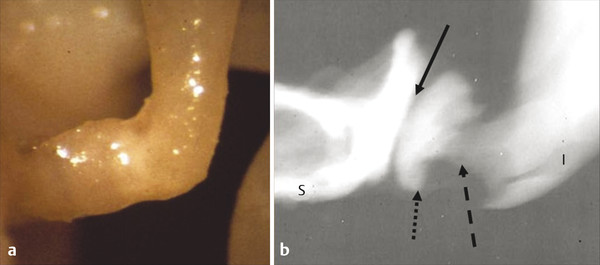
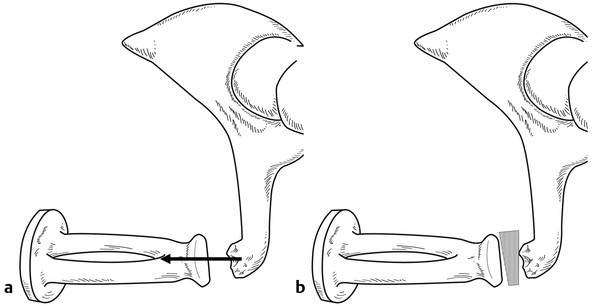
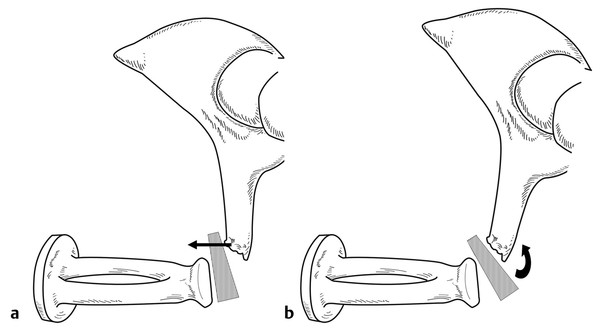
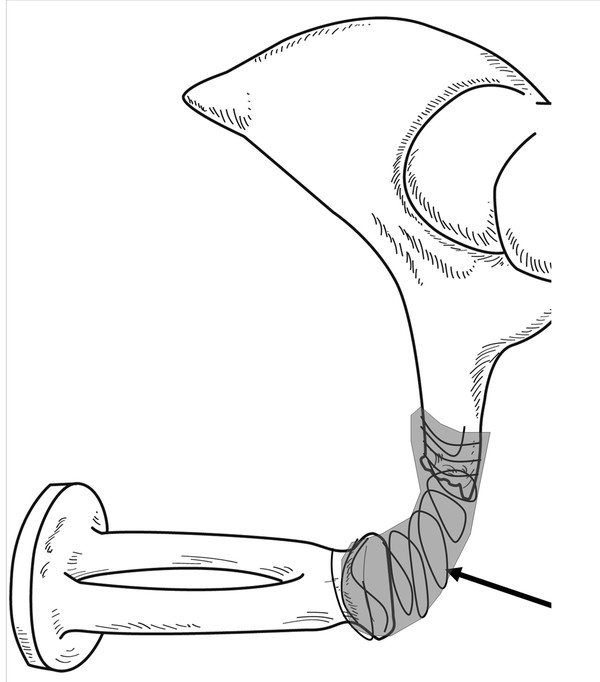
Anatomy The incudostapedial joint connects the incus and stapes and represents the smallest interosseous joint in the human body. Like any other joint, it comprises hyaline cartilage, a synovial membrane, and an articular capsule. The diarthrodial joint is formed by the convex lenticular process of the incus on the one side and by the concave stapes head on the other side, thus forming a ball and socket joint. The lenticular process connects to the long process of the incus in a 90-degree angle (range, 75–105 degrees) and is composed of a thin stem deriving from the long process of the incus and a cap that forms the functional articular surface towards the stapes.1 In fact, the incudostapedial joint capsule not only envelops the lenticular process, but it also incorporates part of the long process into the joint complex (▶ Fig. 27.1; ▶ Fig. 27.2).2 Fig. 27.1 The incudostapedial joint complex. This is a key factor in controlling ambient atmospheric pressure variations in the middle ear as it can decouple the stapes from the rest of the ossicular chain. Fig. 27.2 Anatomy of the incudostapedial joint. The 90° angle is shown in a temporal bone specimen (left). On X-rays (right), the stem (dashed arrow) and the cap (dotted arrow) of the lenticular process next to the joint space (solid arrow) become visible. The articular surfaces of stapes (S) and incus (I) form the functional zone of the incudostapedial joint. Like any other joint of the ossicular chain, the incudostapedial joint has two main functions. First, the joint facilitates sound conduction from the incus to the stapes, for which a stiff and soundproof connection between the lenticular process and the stapes head is necessary. Second, the joint allows gliding movements between the articular surfaces. It is through this gliding movement that the stapes is decoupled from the rest of the ossicular chain, and, hence, the inner ear is decoupled from the large movements of the tympanic membrane, which are caused by changes of ambient atmospheric pressure.3 Among all the delicate structures of the ossicular chain, the long process of the incus is the most vulnerable for developing chronic otitis media with or without cholesteatoma.4 As the ossicles have, unlike other bones, no capacity for self-regeneration, any discontinuity of the ossicular chain can only be repaired by surgical intervention,2 and any attempt to repair the incudostapedial joint must take into account the specific characteristics of this area of the ossicular chain. However, the micro-mechanism of the incudostapedial joint, with its gliding joint movement and possible decoupling of the stapes and inner ear, is currently not replicated by any reconstruction technique. The choice of the reconstructive technique depends on the extent of the defect, which can be just a slightly eroded joint (with a preserved soft tissue bridge between the incus and stapes), or a missing lenticular process, or an increased erosion of the long process of the incus. In principle, the surgeon has two possibilities for treating a damaged incudostapedial articulation. With smaller defects, the original ossicular chain can be rebuilt by the reconstruction of the defective part of the long process of the incus (bridging technique). With larger defects, the sound conducting apparatus must be restructured by bypassing the incus and insertion of a prosthesis (interposition technique). The bridging technique derives from the former type II tympanoplasty according to the Wullstein classification. Although the original type II describes a direct contact between the tympanic membrane and the incus rudiment, this modification restores the continuity of the ossicular chain. The interposition technique, on the other hand, corresponds to the tympanoplasty type III Wullstein classification.5 To date, none of the various surgical techniques to treat a damaged incudostapedial articulation have received universal acceptance. With the bridging technique, the small defect of the long incus process is reconstructed so that the malleus-incus complex with its joint is still operational for sound conduction. The main advantages of the bridging technique are the preservation of the normal tri-ossicular configuration, allowing the full sound energy to be collected from the complete tympanic membrane via the malleus’s handle. Thus, the bridging technique preserves a rather physiological constitution of the ossicular chain and represents the most straightforward way for handling a damaged incudostapedial joint. Most often, autologous materials, synthetic prostheses, and bone cement are used for this technique. With the interposition technique, the sound is transmitted from parts of the eardrum via an interposition graft directly to the head of the stapes. Hence, interposition techniques are independent of a functional malleoincudial joint, which is bypassed. Prostheses made of autologous bone and synthetic materials are the constitutive materials. The significant advantages of using autologous materials for reconstruction are the ease of availability, the absent risk of transmitting disease, their biocompatibility, and their cost-effectiveness. Potential disadvantages include displacement, absorption, and time required to sculpt the prosthesis.6 When the incudostapedial joint is only dislocated, a joint stabilization with perichondrium or temporalis fascia has been described,7 but no long-term results are available. If only the lenticular process is missing, with the majority of the long process of the incus hovering on top of the stapes head, the gap can be bridged with an interposition graft. Here, a piece of (cortical) bone pushed into the gap between the incus and stapes represents the most effective option as it leads to a very firm sound connection. Alternatively, a piece of tragal or conchal cartilage, (depending on the approach), can be used as an interposition graft. In the course of time, however, cartilage might show inferior acoustic results due to softening (▶ Fig. 27.3).8 Fig. 27.3 Ideal situation for a bridging technique: Only the lenticular process is missing, but the long incus process is fully preserved. Hence, the action of the force runs through the stapes axis (left image) and the gap can be bridged with an interposition graft, preferably a piece of bone (right image). If the erosion of the long process of the incus has increased to a degree, where its edge is no longer on top of the stapes head circumference, then a simple bony interposition graft poses the risk of tilting and, subsequently, ineffective transmission with a piston-like movement between the incus and stapes (▶ Fig. 27.4). As a solution, a 1-mm thick piece of cartilage can be cut in a U-shape and a small 1-mm diameter groove drilled centrally into the undersurface of its apex. Although the small groove encompasses the stapes head, the two cartilage legs clasp the remaining part of the long process of the incus, thus preventing dislocation. The lateral surface of the cartilage has direct contact to the tympanic membrane on top and, hence, allows for additional direct sound transmission (the original Wullstein type II tympanoplasty).9 Fig. 27.4 If the edge of the eroded long incus process is out of the stapes head circumference, then the action of the force runs parallel to the stapes action (arrow on left image). Hence, a bony interposition graft poses the risk of tilting and thus ineffective sound transmission (arrow on right image indicates the movement of the graft). If the long process of the incus is too short for bridging, then autologous materials can be positioned between the stapes and tympanic membrane for a direct sound transmission. The correct size of this prosthesis is crucial. If the graft is too short, a loose contact with loss of acoustic energy will result. If the graft is too long, the stapes will be pushed inward, leading to a stiffening of the annular ligament, with a reduction of sound transmission, mostly in the lower frequencies. When available, the autologous incus body, unless extensively involved or eroded by cholesteatoma, represents the gold standard as material for partial ossicular reconstruction as it combines optimal biostability with good acoustic transfer function (see Chapter 28). The incus body must be transformed into a prosthesis with a 1-mm groove in its lower end for placing it on top of the stapes head. The short process is shortened and can be provided with a small oblique groove to engage the malleus’s handle. However, although an autograft of the repositioned incus might provide continuity of the ossicular chain, the fixation to the remnants of the ossicular chain remains a critical issue.2 In addition, the sculpted auto-incus can partially erode or fuse to one of the bony walls around the oval window niche.10 Synthetic alloplastic prostheses have been inserted into the middle ear since the origin of ossiculoplasty in the 1950s, and numerous materials (e.g., plastics, ceramics, various types of metals, etc.) and innovative forms have been proposed. Any middle ear prosthesis must fulfill high demands in terms of biocompatibility and acoustic-mechanic properties to enable optimal sound transmission (see Chapter 29). Following these demands, middle ear prostheses made of titanium or hydroxyapatite appear most suitable and are commonly used by otologic surgeons worldwide.11 A small defect might be filled with medical glue (e.g., fibrin tissue adhesive)12 or cement (e.g., hydroxyapatite, glass ionomeric).13 Prior to using the cement, any soft tissue or unstable bony debris has to be removed from the ossicles to obtain a smooth, dry, and solid bony surface. After the components are mixed, the cement keeps an ideal pasty consistency for a couple of minutes (working time) before it completely hardens. Notably, the various commercially available cements are distinguished from one another based on their handling characteristics and setting times.13 Bone cement and other alloplastic materials may also be combined in such a way that a wire prosthesis or an absorbable suture is initially positioned between the stapes head and the long incus process; the bone cement is then modeled around the assembly with the wire or suture acting as a guide (▶ Fig. 27.5). Fig. 27.5 If bone cement is to be used as bridging material, a wire or a suture (arrow) positioned between stapes and long incus process may give extra support for the cement during the modelling process.
27.1.2 Physiology
27.2 Surgical Technique
27.2.1 Autologous Materials
Bridging Technique
Interposition Technique
27.2.2 Synthetic Prostheses
Bridging Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


