Ptyerygium
Peter Zloty
Michael W. Belin
Introduction
Pterygium is an ancient affliction, having been documented by physicians for at least 3 millennia. Hippocrates encountered and wrote about it. Desmarres, Arlt, Fuchs, and the other early greats in our field were challenged by the pterygium and its ability to blind if left alone, and its tendency to recur if resected.1 Even the earliest descriptions of the lesion describe the propensity of the pterygium to recur after removal. Surgical treatments have ranged from thread avulsion to complete excision. The surgical technique of redirecting rather than resecting the pterygium head is a tribute to its tenacity.
Numerous nonsurgical treatments have been used over the millennia ranging from eye drops containing urine or lead to caustic agents. In the modern era antimetabolites and radiation therapy have been utilized. Only a few treatments have stood the test of time. It is fair to say that no particular technique or regimen has been universally effective, though some were clearly worse than others. Fortunately, as technology and research have improved so have our treatments and results.
Incidence
The incidence of pterygium worldwide is clearly related to ocular sun exposure, particularly when the exposure occurs early in childhood. Outdoor exposure closest to the equator especially increases the incidence. Pterygium incidence is insignificant in the Polar latitudes and nearly 20% at the equator. Risk factors such as airborne particles, smoke, humidity, and allergens have been implicated.2 Comorbid individual patient factors include atopic disease, ocular rosacea, trachoma, vitamin A deficiency, traumatic injury, and race. Pterygium development is typically measured in decades so, consequently there is a blurring of direct causal relationships. For example, the commonly reported male gender predilection is probably related to outdoor work exposure and reflects cultural and practical considerations rather than true gender proclivity.3 Additional relative risk factors for the development of pterygium have been reported as follows: 44-fold greater relative risk of pterygium development for those living in the tropics (30-degree latitude on either side of the equator), 11-fold from working in sandy outdoor environments, 9-fold for those who never wore spectacles or sunglasses, and 2-fold for those who never wear hats.4 Although the precision indicated by these statistics may be overstated, the general trends indicated are meaningful.
In addition to natural sunlight, artificial ultraviolet light sources will increase the incidence of pterygium as well,5 and with appropriate eye protection and shielding the incidence returns to normal.6
No clear hereditary basis has ever been proven in environmentally case controlled studies. Although it is indeed true that certain people-groups such as Aboriginal Australians are almost universally affected, once again environmental exposure is the likely reason. Pterygia are rare in Japan and China, but a question arises: Is this a genetic variation or rather a suggestion that epicanthal folding of the lid may be protective? Sedan and Enroth proposed an autosomal dominant proclivity with incomplete penetrance. They suggest a hereditary component to the disease process that is stimulated by an abnormal reaction to environmental or atmospheric stimuli.4,7,8
Similarly, viral infection, particularly with the human papilloma virus, has been suggested as contributory, but has not been proven.7,9
Barraquer suggested tear film abnormality as the cause of pterygium, with dellen as the stimulus for progression.
Wong suggested that repeated irritation of the limbus induced an angiogenic factor which resulted in pterygium formation.21 This angiogenic factor would be derived from the proteins produced by the ultraviolet denaturation of corneal proteins.
Arlt, Von Graef, and others suggested that inflammation was the primary etiology, with trauma or erosions and micro-ulcerations of the limbus as the stimulus for conjunctival repair that progressed to pterygium growth.7,10,11,12,13,14
Although all of these theories have proponents and data to support them, environmental ultraviolet light exposure is currently the most credible. Further evidence of this includes the observation that patients with solar keratosis are more likely to have pterygium, as well as patients with light irides, and those who are unable to tan without burning.
The exact nature of how the ultraviolet light induces the pterygium is still under investigation. It is well known that UV-B is mutagenic in epidermal cells. In corneal limbal stem cells the p53 suppressor gene is affected by UV-B resulting in excessive production of transforming growth factor-beta. TGF-beta is a family that may comprise as many as 100 distinct proteins. These proteins have proliferative effects on many mesenchymal and epithelial cell types. TGF-beta is important in cellular differentiation and growth. It is frequently added to tissue cultures to enhance cell growth. In the limbal stem cells it leads to cellular migration, angiogenesis, cell growth, and up-regulation of collagenase. The result of this is the elastoid degeneration and other pathologic changes associated with pterygium.
Etiology and Pathophysiology
A pterygium is a slow growing triangularly shaped, slightly elevated lesion, usually on the nasal side of the cornea.15 (Figures 35.1,35.2,35.3) The location nasally may relate to light rays converging on this locus from a refractive effect of the dome of the cornea. Temporal lesions occur as well, usually, but not always, in association with a nasal lesion and not solely (Fuchs’s Dictum)16
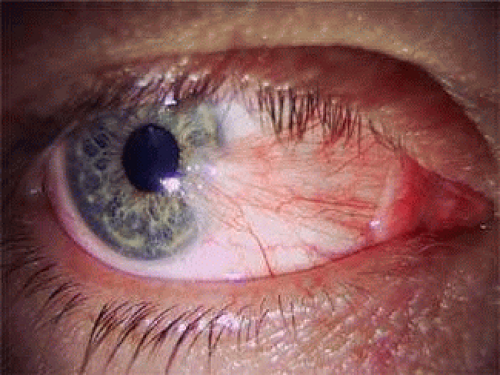 FIGURE 35.1 The primary pterygium is a benign overgrowth of the fibrovascular tissues of the conjunctiva and Tenon’s membrane. The exclusivity of nascent pterygia in the palpebral fissure attests to the environmental nature of their origination. |
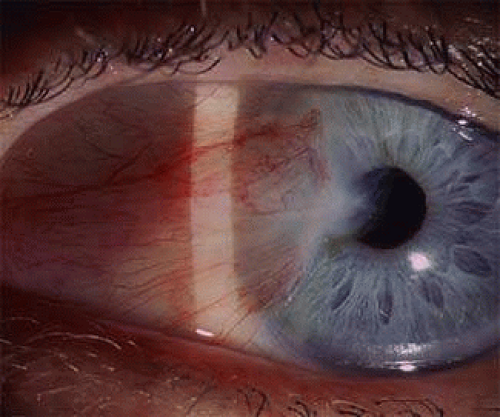 FIGURE 35.2 Many pterygia remain stationary; their location demarcated by iron that has precipitated in the anterior cornea at the head of the lesion (Stocker lines). |
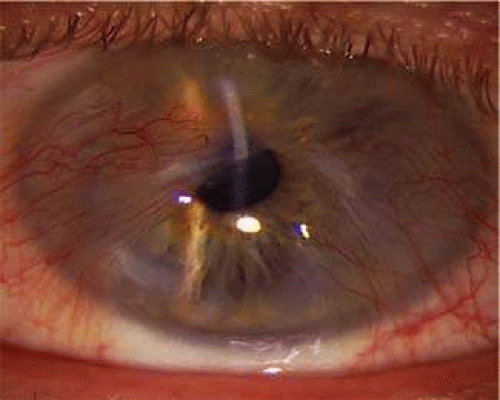 FIGURE 35.3 Nasal pterygium meeting a temporal pterygium over the visual axis. |
The histology of pterygia reveals nothing pathognomonic. The cellular abnormalities are nonspecific and are similar to actinic effects seen in other epithelial tissues. Impression cytology of pterygium conjunctiva shows cells with more metaplasia and cellular atrophy than healthy conjunctiva. The cellular components of pterygium are fibroblasts, T lymphocytes (CD3), monocytes, macrophages, plasma cells, macrophages, and mast cells.17 The fibroblasts from pterygium do not behave normally when placed in tissue culture. They proliferate rapidly and are less dependent on growth factors compared to healthy conjunctiva.18
Pterygium tissue contains type II collagen, normally found in conjunctiva but not cornea, suggesting a genesis not primarily from corneal tissues. Limbal stem cells have been implicated. Microscopic evaluation shows few cellular differences between primary and recurrent pterygia, except for the presence of fibrovascular scar tissue. An important distinction pointed out by some investigators is the fact that recurrence is due to inflammation and angiogenesis and not ultraviolet radiation.19,20,21 Therefore some investigators suggest that a comparison to keloid in the skin would be more appropriate.22 In this context the term recurrent pterygium may be a misnomer.23
The various phases of pterygium growth affect the histological appearance. Stationary pterygium show a subepithelial fibrosis that stops at the apex of the pterygium, with fibrils that are perpendicular or oblique to the direction of the apex and are disorganized and irregular. Advanced pterygia show histological evidence of parallel fibrils replacing Bowman’s membrane and the anterior corneal stroma with epithelial basement membrane directly on the fibrous tissue.
Immunohistochemical studies of pterygia suggest that the pterygium cells probably originate from the limbal stem cells. Though typically nonmigratory, the daughter cells may have become stimulated by ultraviolet light, in addition to other factors to migrate below the basal membrane of the conjunctiva and corneal epithelium. These migrating keratoblasts then infiltrate and destroy Bowman’s membrane and differentiate into cells with fibroblastic activity.24
The corneal involvement proceeds into Bowman’s layer with cellular conjunctival ingrowth along subepithelial corneal nerves. Fissures continue to develop forming islets of epithelium within the corneal stroma (finger in glove effect). Bowman’s layer eventually disintegrates. Cysts appear at the advancing edge and can be seen on slit lamp biomicroscopy (Fuch’s patches) (Fig. 35.4). The tissues will usually have a dragged appearance as blood vessels and conjunctiva show a tractional effect on the ocular surface. The location of a pterygium in any position other than a nasal or temporal position is exceedingly rare. The growth often becomes arrested, with stabilization and even regression of the elevation and vascular injection. The pterygium may become dormant for the remainder of the patient’s life or resume growth later.15
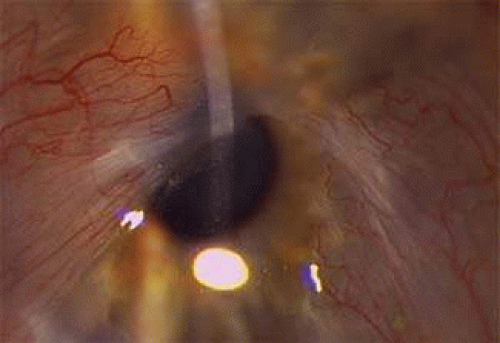 FIGURE 35.4 Enlarged image of Fig. 35.3 demonstrating Fuch’s patches over the pupil. |
All of the previously listed lesions will have an appearance that can be confused with a true pterygium as described histologically. The differential diagnosis is aided by the fact that, in the absence of a lid abnormality, any lesion that does not have a nasal or temporal genesis is probably not a pterygium.
A pseudopterygium usually has an antecedent history of trauma; it may be located anywhere on the cornea and will be attached only at its apex. A muscle hook or forceps passed under the pseudopterygium is a diagnostic maneuver that can be done at a slit lamp, demonstrating its nature. The instrument will easily pass below a pseudopterygium at the limbus but will not with a pterygium.15 Fibrovascular scarring and proliferation associated with Terrien’s marginal degeneration will be at the vertical meridia rather than horizontal.15 A carcinoma-in-situ may appear to be a pterygium at its early stage, but it typically grows wider and does not advance in the pattern of a pterygium (Fig. 35.5). Squamous cell carcinoma and Amelanotic malignant melanoma may also look similar in early stages, but will often have leukoplakia or grow atypically.25
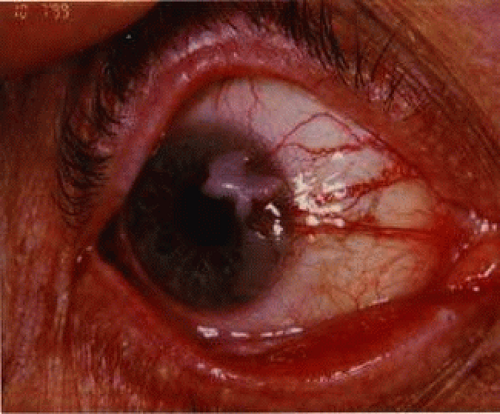 FIGURE 35.5 Carcinoma in situ mimicking a pterygium. Note the irregular raised apex and sentinel vessels. |
There has been a considerable controversy about the nature of pingueculum (Fig. 35.6) and its ability to metamorphize into a pterygium. Fuchs first suggested that pingueculum were the precursor lesions of pterygium. The theory had merit due to the clinical observation that pingueculum were frequently seen in the fellow eyes of pterygium patients and because of the histologic similarities of the two lesions. Confounding this theory is the observation that pingueculum are common in regions where pterygium is rare (i.e., Japan), and they tend not to recur after excision. It is likely, therefore, that the same environmental conditions that induce pingueculum induce pterygium, but the two lesions are distinct.
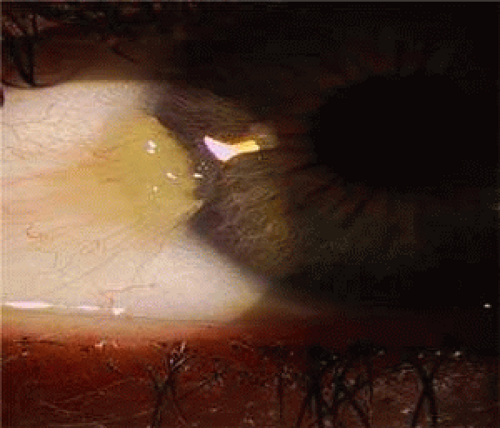 FIGURE 35.6 Pingueculum tissue heaped up on corneal surface mimicking a true pterygium. |
Clinical Course
Many pterygia remain stationary; their location demarcated by iron that has precipitated in the anterior cornea at the head or cap of the lesion (Stocker lines; see Fig. 35.2). These Stocker iron lines are derived from tear film components, notably lactoferrin, and suggest a stable, slow-growing nature of the particular lesion. Pterygia that progress onto the midperipheral cornea will induce visual changes especially under low light conditions where the effect of the irregular astigmatism becomes more manifest. Irregular astigmatism and even frank corneal striae formation induces visual distortion before actual obstruction of the visual axis occurs. Irregular astigmatism is induced when the different meridians of curvature of the cornea are not 180 degrees apart or multiple meridia develop. The distortion from pterygium-induced irregular astigmatism will not correct well with glasses or soft contact lenses. Usually irregular astigmatism is treated with rigid gas permeable contact lenses, but these will fit poorly due to the interference from the lesion. Finally, continued progression into the center of the cornea will obstruct vision.
Nonsurgical Treatments
Most experienced pterygium surgeons have encountered unusually aggressive pterygia and realize that pterygia can be quite malicious. The occasional pterygium surgeon should not make the mistake that a pterygium is a simple nuisance easily dispensed with, but rather understand that it is a condition that can be marked by significant complexity and substantial morbidity if recurrence is encountered, often with a lesion that is worse in recurrence than it was primarily.
Younger patients seem to have worse and more frequent recurrences than older patients. Most recurrences typically present within 6 to 8 weeks of surgery.26
Because pterygium is a slow-growing lesion that can be made worse with an operation, it is useful to ponder the question: “Is surgery always the best choice for an advancing pterygium?” If the patient is aged and dealing well with the pterygium, or if the patient is too ill or merely refuses an operation, are there methods that can assist the clinician in minimizing the effects of the pterygium short of surgery?
Because actinic radiation is integral to the disease progression, ultraviolet-light blocking sunglasses are probably useful and should be recommended. Both UV-A and UV-B protection have been recommended, though it is likely that once the lesion has developed it is too late to truly effect the lesion by limiting the ultraviolet light.27
If the lesion is inflamed, steroid eye drops can be prescribed to reduce the inflammation. Historically, subconjunctival injections of dexamethasone have been attempted, without significant success. Topical indomethacin was extensively investigated for this purpose, also with limited success. Nonsteroidal agents further carry a risk of epithelial toxicity and corneal melting and so probably should be avoided. Because the surface is irregular, tear film stabilizing agents and artificial tears should be recommended to the patient. Ocular astringents will have a temporary cosmetic effect and the patient may wish to use them sporadically.
Topical Cyclosporine A is used in patients to improve tear film mediated ocular surface disease. It may also have an anti-inflammatory and anti-angiogenic effect. A therapeutic effect often takes 6 or more weeks to be achieved. Data are needed to determine if cyclosporine A will effect the natural history of pterygium. Cyclosporine A appears to give symptomatic relief for many patients regardless of whether or not it effects the disease process. It is prescribed as a pharmacy formulated 0.1 to 0.5% emulsion three times daily. A commercial formulation available is Restasis® (Cyclosporine 0.05%, Allergan Pharmaceuticals, Irvine, CA).
Oral Doxycycline is often used to limit collagenolytic enzymes on the ocular surface and decrease inflammation through a mechanism apart from, and in addition to, that which is provided by corticosteroids. Of concern is that it is also a photosensitizing agent and therefore may make the effects of ultraviolet radiation on the eye more acute. If cautioned to wear UV sunglasses, a dose of 50 mg twice daily can safely be prescribed, and may help to limit inflammation on the ocular surface.
Oral and topical steroids are important in the treatment of ocular inflammation. Steroid injections, however, may stimulate conjunctival repair mechanisms and probably should be avoided in pterygium since other forms of application, notably drop therapy are available. New generation topical coticosteroidal agents that are less likely to induce intraocular pressure elevations are preferred for long-term use (Rimexolone 1% or Loteprednol 0.5%).
Punctal plugging will also improve and stabilize the tear film. Plugging the tear ducts increases tear volume, and in the absence of inflammatory tear film disorder, will avoid the expense and possible toxicity of frequently administered artificial tear drops.
Topical and systemic antihistamine type agents and mast cell stabilizers may decrease any coexisting ocular allergies. If the patient has atopic disease, or there is substantial allergic symptoms with the pterygium, such as itching and redness of the eye, these agents should be recommended.
Treatments Adjunctive to Surgery
Medications and treatments considered adjunctive in the operative or perioperative period may be also be useful in delaying or obviating the need for surgery. New agents and novel applications of older agents used to treat neovascularization and fibrovascular proliferation may have a role in pterygium treatment.
Topical Patient Administered Mitomycin C
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


