Chapter 14 This chapter discusses the evaluation and differential diagnosis of proptosis. The underlying etiologies for proptosis range from slow, chronic conditions to acute, life-threatening disease. Accurate use of both the clinical history and features of the specific orbital examination guides the examiner toward the proper choice and timing of ancillary laboratory or imaging studies required to make the appropriate diagnosis and design the proper therapy. In this chapter, major categories of orbital disease are outlined with classic clinical presentations as well as “red flags” that should alert the examiner to the urgency of the workup and onset of therapy. For each specific diagnosis, the reader is referred to the corresponding chapter for detailed management guidelines. Refer to Table 14–1 for differential diagnoses based on the history of the present illness. The history with specific inquiry relevant to orbital processes is invaluable in helping define the differential diagnosis. 1. When was the appearance of the eyes first noted to be abnormal? If the patient is in the pediatric age group, was the proptosis present in early childhood? 2. If the proptosis is acquired, is it stable or is it progressing? If it is progressing, is the change occurring slowly, or rapidly? 3. Is the degree of proptosis affected by change in body position or Valsalva? In a child, is change in the degree of proptosis evident while crying? 4. Request that the patient bring old photographs to the initial examination. Family photographs are an invaluable source of information about progression and rate of change in the patient with proptosis. The past medical history and the associated symptoms are also important in the evaluation of the proptotic patient. 1. Is there a history of systemic disease that may be associated with an orbital process, such as immunologic disorders, diabetes, thyroid disease, sarcoidosis, Wegener’s granulomatosis, other rheumatologic illness, neurofibromatosis, or cancer? 2. Is there a past history of eye disease? 3. Is there a family history of immune-mediated or neoplastic diseases? 4. Is there a past history of ocular or orbital surgery? 5. Is there a history of orbital or ocular trauma? If yes, what is the mechanism of that injury and is there a possibility of an occult foreign body? 6. Is there a history of fevers, night sweats, or recent weight loss? 7. Are there associated symptoms such as pain, diplopia, visual blurring, or loss of color perception or visual acuity? The ophthalmologic examination is key to the diagnosis and management of orbital disease and proptosis. 1. Is there evidence of sensory alteration? Do not apply topical anesthetics (e.g., for measuring intraocular pressure) prior to your evaluation of the patient because they may interfere with assessment of corneal sensation. Impaired sensation or unusual pain suggests trigeminal involvement, seen in orbital apex/cavernous sinus lesions or those that typical invade or track along nerves, such as lacrimal malignancy or invasive basal cell carcinoma. 2. Is there a gaze-evoked change in intraocular pressure? Measure intraocular pressure in both primary position and upgaze. Elevations of intraocular pressure in upgaze are commonly observed in the setting of thyroid-associated orbitopathy (Graves’ disease) or other cicatrizing diseases of the extraocular muscles. Table 14–2 summarizes the complete orbital examination.
PROPTOSIS
QUESTIONS TO ASK REGARDING THE PRESENT ILLNESS
PERTINENT PAST MEDICAL HISTORY AND ASSOCIATED SYMPTOMS
THE OPHTHALMOLOGIC EXAMINATION
QUESTIONS TO ASK AND POINTS TO KEEP IN MIND
History | Differential Diagnosis |
|---|---|
Onset of proptosis: congenital | Vascular malformations, hamartomas, cystic orbital lesions |
Onset of proptosis: days | Orbital cellulitis, nonspecific orbital inflammations, trauma, hemorrhage into prior lesions, high flow arteriovenous fistulas |
Onset of proptosis: days to weeks | Nonspecific orbital inflammations, primary and metastatic neoplasias |
Onset of proptosis: months to years | Structural lesions including dermoids, cysts, mucoceles, slow growing neoplasms such as meningiomas |
Rate of progression: slow | Structural lesions and slow growing neoplasms |
Rate of progression: fast | Metastatic tumors, hemorrhage into preexisting lesions, trauma, nonspecific inflammatory syndromes |
Associated systemic disease | Known malignancy, sarcoidosis, systemic lupus erythematosus, Wegener’s granulomatosis, collagen-vascular conditions, hematologic diseases |
Physical Examination | Look for: |
|---|---|
Ophthalmologic exam | Visual acuity, color perception, relative afferent pupillary defect (APD), choroidal folds, disc edema, disc atrophy, shunt vessels |
Visual Field | Defects in the visual field, changes over time |
Inspection | Ecchymoses or discoloration, conjunctival vascular attenuation or tortuosity, lid lag, lid retraction, dynamic change with Valsalva |
Measurements | Globe position—exophthalmometry readings; globe dystopia —vertical or horizontal displacement |
Palpation | Resistance to retropulsion, discrete mass lesion, pain |
Cranial nerve function | Motility: if limited, restriction versus paralysis; impaired sensation: dermatomal distribution |
Auscultation | Bruits |
Optic Nerve Function
1. Is there a relative afferent pupillary defect (APD)?
Yes: there is asymmetric damage to the optic nerve or retina, possibly secondary to a compressive optic neuropathy (see Chapter 2) (Fig. 14–1).
No: either there is no damage to the afferent system or the damage is too subtle to evoke an afferent pupillary defect (APD) or there is bilateral and symmetric bilateral optic nerve compression.
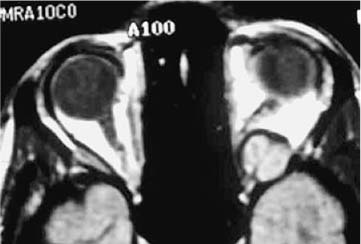
FIGURE 14–1 Schwannoma in orbital apex causing decreased vision from compressive optic neuropathy.
2. Is there an acquired dyschromatopsia?
Formal color testing is indicated to define acquired dyschromatopsia.
In the setting of bilateral, symmetric optic nerve compression, reduced color perception is often observed in each eye and is an early sign of compression.
3. Is there a visual field abnormality?
Formal visual field testing, either with manual or automated perimetry, is indicated as a baseline and for following most orbital diseases.
Abnormal visual fields may be observed in the setting of optic nerve compromise.
Orbital Inspection and Measurements
1. Initial orbital inspection includes observation of the eyelid position and movement (Figs. 14–2 and 14–3).
2. Is there lid lag and retraction?
These findings increase the likelihood of thyroid-associated orbitopathy, one of the most common etiologies of proptosis (Fig. 14–4).
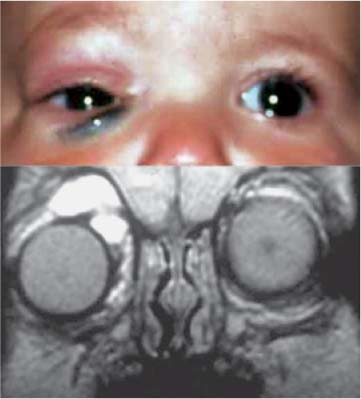
FIGURE 14–2 Inferotemporal displacement of the globe with periorbital echymosis is observed in this child. MRI revealed multiple cyst-like structures in this patient with a lymphangioma.
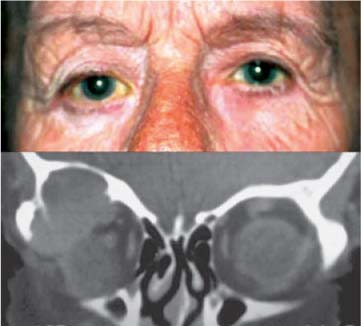
FIGURE 14–3 Note the inferonasal displacement of the globe in this patient. The corresponding lesion, a hematic cyst, was present in the superotemporal orbit and caused erosion of the orbital roof.
3. Is there ptosis?
In the setting of combined thyroid-associated orbitopathy and myasthenia gravis, ptosis may be observed; otherwise, ptosis is a red flag that the diagnosis is not thyroid-associated orbitopathy. The palpebral fissure should be measured with a millimeter rule.
4. Formally measure the globe position with respect to the orbital rim using an exophthalmometer.
Changes in this measurement over time will determine the pace of change of orbital disease, but be careful to maintain the same base measurement for successive examinations.
5. Formally measure globe dystopia, the vertical or horizontal displacement of the eye.

FIGURE 14–4 Bilateral proptosis with significant peri-orbital edema from thyroid-associated orbitopathy.
Vertical displacement is measured as the relative position of the globe with respect to the canthi and horizontal displacement is observed using the distance from the midpoint of the nose to the limbus at the level of the canthi.
Mass lesions in the orbit displace the globe to the opposite direction, e.g., medial lesions result in lateral globe displacement. Knowing the location of the orbital process is useful in forming the differential diagnosis.
6. Is the abnormal side proptotic? Or is it enophthalmic?
Enophthalmic changes in globe position are seen in the setting of chronic maxillary sinusitis with orbital floor erosion or in cicatrizing orbital disease such as metastatic scirrhous breast carcinoma.
Pathologic enophthalmos is often associated with abnormalities of eyelid function, such as lid lag or a superior sulcus deformity.
Motility
Many disorders of the orbit produce associated changes in motility, secondary to either myogenic or neurogenic involvement.
1. It is critical to measure both phorias and tropias using prisms with the cover and cross-cover testing in the cardinal fields of gaze.
2. Formal measurements of ocular ductions and versions should also be carefully performed.
It is important to use a standard notation that allows differentiation of subtle changes over time. For example, the lateral version reflex (LVR) allows the quick, reliable, reproducible measure of ocular motility and is ideal for following neuro-ophthalmic patients with either paralytic or myogenic strabismus. This test is easily performed with the careful use of a strong penlight that is coaxial with the observer and with stabilization of the patient’s head. The patient is asked to look in far upgaze, downgaze, abduction, and adduction, and the position of the light reflex is noted relative to the corneoscleral limbus (in millimeters). The measurements are noted in the patient’s chart and changes over time are easily appreciated.
3. If abnormal motility is observed, then perform the forced duction test to differentiate between paralytic and restrictive deficits.
Orbital Palpation
Orbital mass lesions that are anteriorly located in the orbit are amenable to direct examination by palpation. Palpation may be helpful in determining both the differential diagnosis and the selection of a potential site for biopsy. Compressibility of the mass may indicate a vascular lesion. Such lesions, if high flow, may also produce an orbital bruit that is evident on auscultation. Solid tumors are firm and less compressible. Pain on orbital palpation is often associated with inflammatory or infectious lesions.
LABORATORY EVALUATIONS IN PATIENTS WITH PROPTOSIS
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


