Chapter 140 Prognosis of Posterior Uveal Melanoma
Ocular prognosis of globe-conserving therapies
Treatment of primary choroidal melanoma without evidence of metastasis involves either globe-conserving therapy or enucleation. In a randomized clinical trial of patients with primary choroidal melanoma treated with globe-conserving iodine-125 brachytherapy versus enucleation, the Collaborative Ocular Melanoma Study (COMS) demonstrated no significant difference in mortality, 5, 10, and 12 years following treatment between brachytherapy and enucleation.1–3 Thus, increasing emphasis has been placed on globe-conserving therapy for choroidal melanoma. Reported rates of local treatment failure vary between treatment modalities and between centers using similar modalities. Radiation therapy overall results in lower rates of local treatment failure compared to nonradiation-based treatment approaches.
Radiation
Maintaining the integrity of the eye after globe-conserving treatment for choroidal melanoma is an important outcome in evaluating the success of a specific treatment. Local treatment failure or local tumor recurrence is associated with morbidity consisting of either need for re-irradiation or organ loss by enucleation. Iodine-125 plaque radiotherapy is the most common primary treatment modality for choroidal melanoma. Among the largest published series reporting local treatment failure with iodine-125, the COMS medium tumor trial reported the risk of treatment failure at 5 years, as measured by local recurrence rate in 650 patients to be 10.3%.4 A report by Sagoo et al. of 650 juxtapapillary tumors indicated a local treatment failure rate of 21% at 10 years.5 For iodine-125 brachytherapy the local treatment failure rate in the literature ranges from 0 to 27% among centers with varying follow-up intervals and sample sizes.6–22 Series by McCannel et al.6 and Tabandeh et al.8 reported very low local failure rates with iodine-125, 0% and 1.7%, respectively; both centers use intraoperative ultrasonography which minimizes the risk of edge-miss. Among the treatment modalities that involve radiation, Rouberol et al. reported a 21.7% and 24.3% rate of local recurrence after 5 and 10 years, respectively, after ruthenium brachytherapy in 213 patients treated from 1983 to 1995.23 Wilson also reported in a retrospective review a higher local treatment failure rate using ruthenium plaques compared to both proton beam irradiation and iodine-125 brachytherapy.24 In a series of 368 patients treated with proton beam, Mosci reported a local treatment failure rate of 8.4%.25 In another group of 1922 patients treated with proton beam irradiation, a local recurrence rate of 3.2% and 4.3% at 5 and 10 years, respectively, was reported.26 Published data indicate that the use of ruthenium results in higher rates of local treatment failure than iodine-125. Proton beam radiotherapy has a variable rate of local failure depending on the experience of the treatment center. Iodine-125 is the most commonly used form of local treatment for uveal melanoma in North America and rates of local treatment failure vary between centers.
Nonradiation therapy
Nonradiation local treatment of uveal melanoma includes laser photocoagulation, Visudyne photodynamic therapy, and transpupillary thermotherapy. With a reduction in primary enucleation for choroidal melanoma, and a general trend toward eye-salvaging therapy, developments in nonradiation therapies continue to emerge. The main theoretical advantages of laser over radiation include minimizing collateral damage to healthy ocular tissues compared to radiation, minimizing radiation exposure to the patient and operator, and a more simplified treatment approach not requiring radiation oncology or use of an operating theater. However, laser overall has been found to be less successful in achieving local tumor control compared with most forms of radiation-based treatment. The literature is sparse on reports utilizing argon laser photocoagulation to treat choroidal melanomas, but there are many reports of failures, and the prevailing opinion is that argon laser is not an adequate primary treatment for choroidal melanoma of any size.27–29 There are few reports of photodynamic therapy for uveal melanoma in the literature; only two case reports exist using this technique for small atypical amelanotic choroidal melanoma.30,31 Barbazetto et al. reported a case series of four patients treated by photodynamic therapy with recurrent tumors treated with other modalities, resulting in eventual enucleation of two eyes.32
Following the discontinuation of transpupillary thermotherapy (TTT) as a therapy for age-related macular degeneration, a noticeable interest in this form of thermal laser for use in posterior segment tumors occurred. However, the largest series using TTT reported high rates of local treatment failure. Shields et al. reported a 22% local treatment failure rate at 3 years in a series of 256 posterior uveal melanoma treated by transpupillary thermotherapy.33 Aaberg et al. reported a rate of 23% at 5 years in a series of 135 patients.34 Zaldivar described eight cases with histologic findings in eyes enucleated after failed TTT. Although the height of the tumor decreased, extrascleral extension and lateral spread of the tumor ensued.35 Harbour found that not only was there no significant difference in visual outcome between TTT and plaque radiotherapy, but also that the recurrences were substantially higher when TTT was used compared with iodine-125 plaque.36 Currently, the use of TTT has been limited to an adjunct to primary brachytherapy to compensate for edge-miss in plaque placement by some operators.37,38
Surgery
Peyman et al.39 studied a group of 34 patients treated by eye wall resection with an average follow-up of 5.3 years and reported that 11 (32.3%) required enucleation (mainly because of evidence of tumor cells in resected margins) and 13 (38.2%) retained 20/200 or better vision after treatment. No patient had local treatment failure, and two patients had died of metastatic melanoma at the time of that report. In a matched case–control study, 81 of 49 pairs of patients undergoing either transscleral resection at one center or iodine brachytherapy at another, Kivela and colleagues found fewer recurrences with plaques than resection, but no difference in 8-year mortality.40 Furthermore, only eyes undergoing radiation experienced neovascular glaucoma, radiation retinopathy, cataract or ischemic changes. Shields et al.41 described a series of 95 patients with choroidal or ciliary body tumors, or both, who were managed by partial lamellar sclerouvectomy. A total of 81 cases (85%) were uveal melanoma; vitreous hemorrhage occurred in 79 (83%); intraretinal or subretinal hemorrhage in 33 (35%); retinal detachment in 26 (28%), and cataract in 32 (34%) patients. Retinal detachment surgery was necessary in 16 patients (17%), and enucleation was necessary in 15 (16%) patients. Distant metastases developed in five patients (5%) with a median follow-up of 2.5 years. In the largest series of transscleral endoresection by Damato et al., the local treatment failure rate at 3 years was 20%.42 Puusaari et al. in a series of 33 patients reported a local treatment failure rate of 40% by 5 years.43 Garcia-Arumi44 reported in a series of 34 cases of vitrectomy with tumor endoresection with average follow-up of 70 months a local treatment failure rate of 5.8%, which is comparable with reports of others who have used vitrectomy with endoresection.45,46
Systemic prognosis for metastasis and death
The most common site for metastasis in uveal melanoma is the liver. At least 50% of all patients diagnosed with uveal melanoma develop metastatic disease.47 The COMS study reported liver metastasis with median survival once metastasis was diagnosed between 6 and 12 months.48 In an analysis of metastatic uveal melanoma patients by Rietschel et al., the authors found that the most common nonhepatic first-metastatic site to be diagnosed was the lung.49 Patients who were younger than age 60, had metastasis to the lung, had a longer interval between treatment of the melanoma and discovery of metastasis, had better survival after a diagnosis of metastatic disease.
There is a lack of substantial difference in survival for local globe-preserving therapies compared with enucleation in the early post-treatment years, which may be related to the possibility that metastases occur before the tumor is treated, perhaps before it is diagnosed.50 Another consideration in evaluating the apparent similarity in survival outcome of conservative therapies in comparison with enucleation is that selection of patients with small- to medium-sized tumors and other more favorable prognostic indicators for eye-sparing treatment methods may bias survival results in favor of these therapies. It is therefore important to control for these prognostic factors to the extent possible in nonrandomized studies. A data collection and management system for studies of prognosis and treatment was developed in the 1980s in order to standardize these measures in observational cross-sectional and longitudinal studies, and was used to identify several factors relevant to metastasis.51–54 In the initial studies evaluating prognosis after treatment with proton beam or enucleation,53,54 the Cox proportional hazards model was first used in ophthalmology to study prognosis and survival after treatment of uveal melanoma. Epidemiologic methods were applied to standardize variables and control for differences in demographic factors as well as tumor-specific variables: tumor height, tumor diameter, location of the tumor posterior to the equator, anterior to the equator, and involvement of the ciliary body. Larger tumor size and anterior location decreased rate of survival, and treatment type did not have a significant effect. Length of observation period or evidence of growth prior to treatment has not been shown to affect prognosis. Visual outcomes after proton beam irradiation were also evaluated using these methods.55,56
Radiation therapy
Metastasis and survival
Actuarial survival rates following radiation therapy of uveal melanoma have been reported to be 75%57 to 80%,58 and 89%59 5 years after treatment. For 96 patients treated by cobalt plaque, the 5-year survival rate (without death from metastatic melanoma) was approximately 75%.57 In a study of 128 patients treated by proton beam irradiation,58 with a median of 5.4 years of follow-up, the probability of metastasis-free survival at 5 years was 80%. Lommatzsch60 reported a 5-year survival of 89% in a group of 309 patients treated by ruthenium. In that study, tumors measured up to 5 mm in height and 15 mm in diameter, and the mean follow-up was 6.7 years. Similar survival estimates were observed in a series of ruthenium-treated patients in Germany,61 Sweden,62 and Finland.63 In an update of an earlier report, Char reported on long-term outcomes in 218 patients treated with helium ion irradiation and followed for an average of 12 years.64,65 The mean tumor thickness in this cohort was 6.7 mm, and the mean largest tumor dimension was 11.9 mm; 5-, 10-, and 15-year survival were estimated to be 73%, 61%, and 54%, respectively. Series of patients treated by iodine-125 irradiation66,67 have also been described.
Prognostic factors for patients treated by irradiation have been evaluated in several studies. Using the tumor registry and analytic methods developed by Seddon and colleagues,51–56 the first 780 patients treated by proton beam irradiation were evaluated,58 of whom 64 had developed metastasis at the time of the study. Similar to the earlier studies, leading predictors of metastasis were tumor diameter larger than 15 mm, ciliary body involvement, extrascleral extension, and age at treatment of 60 years or older. Surgical localization of the tumor and elevated pretreatment liver enzymes were not statistically significant prognostic factors. They found no survival advantage of proton beam irradiation compared with enucleation.53,68 In an investigation of the role of hormonal factors in the development of metastasis,69 among women of childbearing age who had been treated by proton beam irradiation for uveal melanoma neither postirradiation pregnancy history nor oral contraceptive use were associated with the rate of metastasis.
Augsburger and Goel studied tumor regression as a prognostic factor for metastasis following cobalt plaque irradiation. Findings of this preliminary study suggest that rapid tumor regression is a poor prognostic sign.70 Tumors regressing more rapidly were significantly more likely to metastasize concurrently with their regression in a series of patients treated by proton beam irradiation.71
Local tumor recurrence or local treatment failure may increase the risk of metastases from uveal melanoma.72,73 This appeared to be the case in a cohort of patients with juxtapapillary melanoma treated by brachytherapy.74 In that study, rates of melanoma metastasis were 13%, 16%, and 37% at 5, 10, and 15 years, respectively; tumor recurrence (defined as any amount of regrowth), larger tumor diameter, and superior location of the tumor were found to predict occurrence of distant metastasis. This may be due in part to technical difficulties in placement of the plaque, resulting in undertreatment of the tumor (or overtreatment of the normal retina). Harbour et al.75 evaluated the prognostic significance of patterns of tumor regrowth after irradiation. The relative risk for death resulting from metastasis was significantly higher among patients with increased tumor thickness than among those whose tumor spread at the margin (5.1 versus 2.2, respectively, relative to those without tumor recurrence). The mean rate of metastasis was also significantly higher in patients with increased tumor thickness compared with those with marginal spread. Reducing local treatment failure is critical in the management of primary uveal melanoma not only for the sake of preserving the eye, but more importantly for lowering the risk of systemic metastasis.
Prognosis after enucleation
Metastasis from uveal melanoma may occur at any time after the onset of tumor diagnosis. Jensen,76 in his 25-year follow-up of Danish patients, found that the peak incidence of metastasis occurred during the first year after enucleation, and over half of those who developed metastasis did so within 3 years of treatment. However, it is a well-known but poorly understood fact that patients may develop metastasis decades after enucleation. Due to hypotheses that enucleation itself might cause increased mortality,77 the COMS study compared enucleation to pre-enucleation radiation for large tumors, and did not find a difference in mortality.47
Comprehensive and long-term studies of survival after enucleation derive from Denmark and Finland. These reports have the advantage of being population based with few losses to follow-up. Raivio compiled a roster of all patients diagnosed with uveal melanoma between 1923 and 1966 in Finland.78 Of 359 identified cases, survival status at 10 years was known for all but five patients; 314 cases (89%) had 15 or more years of follow-up available, and 214 cases (60%) had at least 20 years. The 5-, 10-, and 15-year survival rates based on melanoma-related deaths were 65%, 52%, and 46%, respectively. Of the 42 patients who survived at least 20 years, nine later developed metastasis. Jensen76 evaluated survival at least 25 years after enucleation in Danish patients with uveal melanoma. The majority of patients included in the original series had died (82%); 51% of those deaths were due to metastasis. Actuarial survival rates at 5, 10, and 15 years were similar to those reported by Raivio.78 A novel deficit survival analysis of 230 patients in 1984 by Lavin and colleagues indicated no overall survival advantage after enucleation.79
Metastasis from uveal melanoma usually occurs within the first few years after enucleation. The liver is usually the first site of metastasis after treatment.80–83 There is some evidence to suggest that metastasis may occur several years before the diagnosis of hepatic metastasis is made.50,84,85 Other organs that may be affected include the lung, bone, skin, and central nervous system.82 The majority of patients with hepatic involvement succumb within a few months of detection of the metastatic lesion.83
Visual prognosis and ocular morbidity
Rates of complications and visual loss after radiation depend on the type of treatment and the size and location of the tumor within the eye. Severe complications requiring enucleation have been reported to occur in 10%86 to 22%65 of patients. Rubeosis iridis and neovascular glaucoma87 and radiation retinopathy or optic neuropathy60,81,88,89 have been reported as the major complications that may occur in irradiated eyes. Lens opacification is a common complication of helium ion90 and proton beam91 radiotherapy, occurring in over 40% of cases in published series. Development of cataracts is also relatively common after episcleral plaque therapy67,92,93 with reported 5-year incidence ranging from about 20%67 to 37%.93
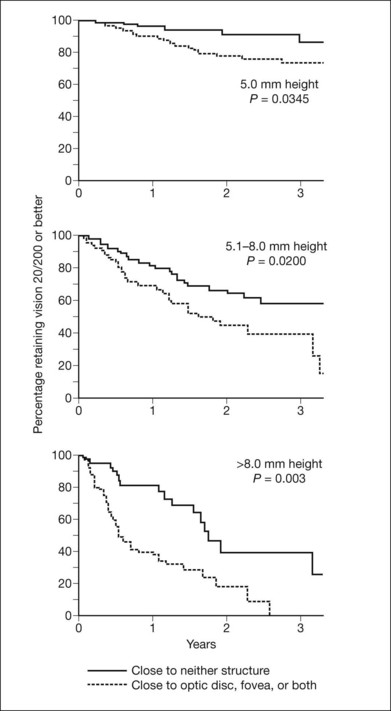
Vision after proton beam irradiation has been studied,55,56 and greater tumor thickness and proximity to the disc or macula (or high dose to these structures) were found to increase the risk of vision loss to worse than 20/200. Curves demonstrating cumulative probability of visual acuity loss according to height and distance of the tumor from the optic disc and fovea are presented in Figure 140.1. When patients were evaluated according to combined tumor characteristics, the probability of retaining vision of 20/200 or better at 3 years was 91% in the low-risk group (tumors 5 mm in height and more than two disc diameters from the macula and disc), 61% in the intermediate-risk group (tumors that were tall or close to the disc or macula), and 24% in the high-risk group (tumors that were tall and close to the disc or macula).
Visual field deficits have also been demonstrated after proton beam irradiation.94 Visual acuity outcomes similar to those in proton beam-irradiated patients were seen after iodine-125 plaque.95 In a review of 93 patients undergoing plaque therapy for juxtapapillary lesions,74 72% of patients lost at least three lines of visual acuity as measured on a Snellen chart by 4–5 years after treatment. The risk of losing this amount of vision was related to initial visual acuity; patients with better initial visual acuity (i.e. 20/20–20/40) were more likely to experience a loss of three or more lines than those with initial visual acuity of 20/50–20/100 or worse than 20/100 (67%, 64%, and 8%, respectively, at 5 years after treatment). In another study of 186 patients treated by helium ion irradiation, 49% retained 20/200 or better vision in the treated eye, with a median follow-up time of 26 months.96
In addition to measured visual acuity, visual functioning is a major concern after treatment for uveal melanoma. Augsburger et al.97 evaluated vision-related changes in employment and ability to drive, read, and watch television by standardized interview in patients treated by plaque radiotherapy or enucleation. Among 51 patients in the plaque radiotherapy group followed for a mean interval of 87 months after treatment, over 90% had no loss of vision-related performance. Similar results were reported in 51 enucleated patients followed for an average of 89 months. Thus, despite potential acuity loss in the affected eye, the vast majority of patients treated with plaque radiotherapy or enucleation retained full functioning in vision-related activities.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


