Principles of Trauma
Peter J. Koltai
James Chan
Trauma is the leading cause of death and disability of Americans younger than 40 years (1). In the United States, more than 150,000 violent deaths occur each year, and more than 500,000 trauma victims are left with permanent disabilities. Annually, approximately 30 to 40 million visits are made to emergency departments for injury treatment (2). The cost to our society is significant. In 2000, $117 billion was spent by Americans, which accounts for 10% of all medical expenditures (3). This is comparable to the percentages attributable to other public health issues such as obesity (9.1%) and smoking (14.4%) (4).
Deaths from trauma fall into three categories— immediate, early, and late. Immediate death occurs within minutes of injury and is caused by acute airway obstruction or major vessel disruptions of the brain, heart, or other internal organs. Early death occurs in the first few hours after injury and is associated with excessive hemorrhage, blood accumulation around the brain, or respiratory failure. Late death occurs days to weeks after trauma and is caused by sepsis and multiple organ failure.
More than half the deaths due to trauma occur within several minutes of the accident. Because immediate treatment is rarely available, accident prevention is the most logical way to decrease this number. Many public health injury prevention strategies have been successfully implemented including use of seat belts (5) and bicycle helmets (6), implementation of blood alcohol limits (7), and fire safety education including widespread smoke alarm use (8). Early deaths account for about one-third of all trauma deaths. Although not all of these patients can be saved, many can be treated effectively with rapid and definitive response. This requires a parallel system of coordinated prehospital care and hospital care at dedicated trauma centers.
Death at an accident scene is usually related to head injury with associated hypoventilation due to loss of consciousness. Intubation in the field can thus be lifesaving. Massive hemorrhage is another common cause of prehospital death. When intravenous catheters are inserted at the scene, circulatory volume can be maintained until the hemorrhage can be surgically controlled. Rapid transport to a hospital with an organized team of surgeons, anesthesiologists, and trauma professionals is vital for the effective treatment of trauma patients. In urban areas, ambulances usually provide efficient transportation to the hospital. In rural areas, distance becomes a critical factor and helicopters or airplanes can be lifesaving.
Trauma patients undergo rapid and severe changes in normal body function, including hemorrhage, tissue hypoxia, cellular damage, and disrupted function of vital organs. The physiologic response to massive injury is dramatic and occurs both systemically and locally. Systemic responses include activation of the clotting sequence, shifts of extravascular fluid into the circulatory system, redistribution of blood flow to the heart and brain, and alterations in renal and pulmonary function to maintain acid-base balance. Metabolic changes include skeletal muscle and fat breakdown to provide substrate for the body’s fuel-intensive response to trauma. Local responses include immunologic activation with leukocytes mobilization, acute-phase protein synthesis, inflammatory cell migration into the injured area, and onset of fibroblast proliferation and blood vessel ingrowth to begin the wound repair process. Understanding the restorative mechanisms that occur in an acutely injured patient is necessary for the complex task of treating these patients with regard to fluid maintenance, nutritional requirements, wound healing, and susceptibility to infection (9,10).
NEUROENDOCRINE RESPONSE
Hemostatic adjustments to trauma are mediated by the neuroendocrine system. Stimuli such as hemorrhage, hypoxia, and tissue damage stimulate a graded response that increases to a peak level, after which additional response is no longer possible. Pain is the first signal from
the central nervous system (CNS) to reestablish homeostasis. The hypothalamic response to pain stimulates the pituitary gland to release corticotropin, which stimulates adrenal secretion of cortisol. Pain causes elaboration of antidiuretic hormone for fluid conservation. Pain activates the sympathetic nervous system and stimulates direct adrenal secretion of epinephrine.
the central nervous system (CNS) to reestablish homeostasis. The hypothalamic response to pain stimulates the pituitary gland to release corticotropin, which stimulates adrenal secretion of cortisol. Pain causes elaboration of antidiuretic hormone for fluid conservation. Pain activates the sympathetic nervous system and stimulates direct adrenal secretion of epinephrine.
Blood loss stimulates vascular pressure and volume receptors and precipitates a CNS-mediated decrease in cardiac output, an increase in peripheral vascular resistance, and redistribution of blood flow to vital organs. Hypoxia and hypercapnia cause chemoreceptor stimulation, vasomotor activation, and increased respiratory drive. At later stages, stimulation of the hypothalamus by interleukin 1 initiates the hypermetabolic response to injury manifested by the elevated temperatures experienced by injured patients (11,12).
The hormonal response to trauma is marked by a rise in the catabolic hormones, corticotropin, cortisol, growth hormone, glucagon, epinephrine, and norepinephrine. In contrast, plasma concentrations of the primary anabolic hormone, insulin, are decreased due to CNS-mediated sympathetic inhibition of the pancreas. Posttraumatic hyperglycemia provides non-insulin-mediated tissues such as the brain with a preferential supply of glucose.
Glucagon, cortisol, and catecholamines maintain blood glucose levels and prevent hypoglycemia. The primary function of glucagon, which is produced in the pancreas, is to promote gluconeogenesis in the liver. After trauma, direct sympathetic stimulation of the pancreas enhances glucagon secretion. Corticotropin release by the anterior pituitary gland causes adrenal production of cortisol, which promotes the breakdown of skeletal muscle into amino acids and facilitates gluconeogenesis in the liver. The hypoglycemic effect of cortisol counteracts insulin.
Release of catecholamines is the most fundamental hormonal reaction to trauma. Epinephrine, released by the adrenal medulla in response to direct neurostimulation, is a potent regulator of the circulatory system and systemic metabolism. Epinephrine’s hemodynamic effects include vasoconstriction, increased cardiac rate, and increased myocardial contractility and conductivity. Epinephrine also promotes glucose production by enhancing hepatic gluconeogenesis and inhibiting insulin release. Norepinephrine, the primary sympathetic nervous system neurotransmitter, exerts a direct effect on the circulatory system and vital organs. With massive and prolonged sympathetic discharge, norepinephrine can enter the bloodstream and exerts a direct vasoconstrictive effect on the vascular system similar to that of epinephrine (9,10).
METABOLIC RESPONSE
The postinjury period is characterized by catabolism. Negative nitrogen balance, hyperglycemia, and heat production reflect the increased energy requirements for ongoing reparative and inflammatory processes. Increased energy expenditure is due to sustained release of circulating catecholamines and increased activity of the sympathetic nervous system. The primary energy source during this period comes from oxidation of lipids promoted by the elaboration of the catabolic hormones (9,10).
Although fat is the primary energy source after injury, protein is also broken down to produce energy. In a fasting catabolic patient, glucose can be generated only from the breakdown of protein. Lipid breakdown to triglycerides and glycerol contributes minimally to form precursors for the synthesis for new glucose. As a result, protein is rapidly broken down to form precursors for new glucose synthesis in a trauma patient in the catabolic state. The result is rapid loss of muscle mass. The depth and the length of the catabolic state are related to trauma severity. Although it represents an adaptive mechanism, a persistently prolonged and severe catabolic state leads to severe malnutrition, multiple organ failure, and death (9,10,13,14,15).
TREATMENT OF A PATIENT WHO HAS SUSTAINED TRAUMA
The key to improving survival and managing disability in the trauma patient are the initial evaluation and resuscitation performed at a dedicated trauma center. The American College of Surgeons has developed a protocol taught in advanced trauma life support courses to improve the care of injured patients during the early hospital phase. It is based on a primary and secondary survey approach that allows physicians to handle the complex, multisystem problems of trauma patients. This treatment algorithm can be divided into four categories—primary survey, resuscitation, secondary survey, and definitive care.
The primary survey involves hierarchical assessment of airway, breathing, and circulation. The purpose is to identify extreme, life-threatening injuries and institute immediate life-sustaining maneuvers. Resuscitation is performed simultaneously with the primary survey. The secondary survey consists of a rapid but systematic head-to-toe physical examination with the patient completely disrobed. This global assessment is done to identify all potentially lifethreatening and occult injures. An important part of the primary and secondary survey are radiographic studies including the use of ultrasonography. Samples are drawn for baseline blood studies, typing, and cross-matching. Once these priorities have been addressed, vital signs are rechecked. When the patient’s condition is stable, a detailed management plan is established.
Primary Survey
Airway
The foremost emergency measure is establishing the airway, which may be lost to a variety of causes. The oropharynx, larynx, and trachea can be obstructed by secretions,
blood, and foreign bodies. Oropharyngeal airway collapse can occur with loss of consciousness and from facial fractures (Chapter 78). Direct trauma to the larynx and trachea may cause airway obstruction below the oropharynx (see Chapter 77). Manuevers to secure an adequate airway range from the simple to the complex and begins with manual cleaning of the oropharynx followed by suctioning of secretions (Chapter 63).
blood, and foreign bodies. Oropharyngeal airway collapse can occur with loss of consciousness and from facial fractures (Chapter 78). Direct trauma to the larynx and trachea may cause airway obstruction below the oropharynx (see Chapter 77). Manuevers to secure an adequate airway range from the simple to the complex and begins with manual cleaning of the oropharynx followed by suctioning of secretions (Chapter 63).
The primary risk during early airway management is neck movement when there is an occult cervical spinal fracture. The airway must be controlled with the assumption that such a fracture exists. The neck must be completely immobilized in a neutral position. One member of the trauma team must be assigned to kneel at the head of the stretcher to maintain inline manual head stabilization and avoid hyperextension by holding the cervical spine with the hands while immobilizing the head with the forearms (Fig. 74.1). Traction on the head is avoided, because distraction with further injury to the spinal cord can occur if the patient has an unstable cervical spinal injury. Once the neck of an unconscious patient has been secured, forward traction of the mandible is performed to overcome pharyngeal collapse (Fig. 74.2). The next step is oropharyngeal airway placement in the unconscious patient. If the patient is conscious, a nasopharyngeal airway is used. Once the airway has been established and the patient is spontaneously breathing, supplemental oxygen can be provided through nasal prongs or a face mask.
When these simple measures are unsuccessful, more aggressive airway management is needed. Nasotracheal intubation is the preferred technique for establishing an airway in a conscious patient who may have a cervical spinal injury because it can be done without excessive neck mobility. Nasotracheal intubation is better tolerated by an awake patient than is orotracheal intubation and does not necessitate sedation or muscle relaxation. Nasotracheal intubation is precluded if the patient has extensive maxillofacial injuries.
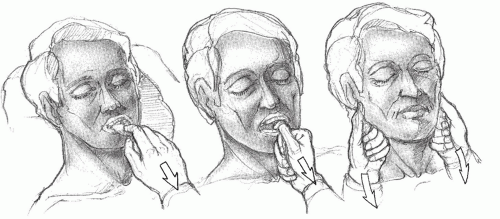 Figure 74.1 Stabilization of the cervical spine during primary survey of an injured patient. |
 Figure 74.2 Once the neck of an unconscious patient has been secured, forward traction of the tongue and mandible is performed. |
If the nasotracheal route cannot be used, orotracheal intubation is the next step. In ideal circumstances, a crosstable lateral cervical spine radiograph is obtained before orotracheal intubation to evaluate for a possible cervical spinal fracture. It is nevertheless important to remember that even a normal cross-table lateral radiograph of the cervical spine does not definitively exclude the presence of cervical spinal fracture or instability (16). When emergency airway control with orotracheal intubation is indicated, intubation proceeds with inline stabilization whether or not radiographs have been obtained. Bag-mask intubation can be an effective method of maintaining the airway until radiographs are obtained. If the patient is unconscious and cervical spinal injury has been ruled
out, orotracheal intubation can be readily accomplished. A patient who is awake must be paralyzed with succinylcholine for successful orotracheal intubation.
out, orotracheal intubation can be readily accomplished. A patient who is awake must be paralyzed with succinylcholine for successful orotracheal intubation.
After intubation, the chest is auscultated to ensure that the tube is in the trachea and not in the esophagus or in one of the mainstem bronchi. Correct endotracheal tube positioning can be confirmed reliably by the presence of end-tidal carbon dioxide. Carbon dioxide from the lungs can be detected rapidly by observing a color change on a disk that can be connected rapidly to the endotracheal tube. If no carbon dioxide is detected, the endotracheal tube is in the esophagus, and a new airway is attempted. If the patient is in cardiac arrest, endtidal carbon dioxide is unreliable in confirming the positioning of an endotracheal tube. A follow-up chest radiograph to confirm the position of the tube must be obtained expeditiously.
If an endotracheal tube cannot be inserted, as when a patient has major facial fractures or has sustained laryngotracheal trauma, surgical airway intervention may be needed. There are four surgical methods of obtaining an airway—needle cricothyrotomy, conventional cricothyrotomy, tracheotomy, and percutaneous transtracheal ventilation.
For children, needle cricothyrotomy is the best procedure. The procedure is performed by placing a number 12 or number 14 intravenous cannula with a plastic sheath through the cricothyroid membrane into the tracheal lumen. Once in the airway, the needle is withdrawn and the plastic sheath is advanced. When properly positioned, the sheath is connected with intravenous tubing to wall or bottled oxygen at 50 pounds per inch of pressure (about 15 L oxygen per minute). Ventilation is accomplished by means of 1-second intermittent injections of oxygen followed by 4-second exhalations. Patients can be maintained for up to 30 minutes with this technique, after which hypercapnia becomes a problem.
Surgical cricothyrotomy is the preferred approach for adult patients who need surgical airway intervention (Fig. 74.3). It consists of a small vertical skin incision over the area of the cricothyroid membrane followed by a horizontal incision through the cricothyroid membrane itself. The blunt end of the scalpel is inserted between the cricoid and the thyroid cartilages and rotated 90 degrees to make an opening through which an endotracheal tube or tracheostomy tube can be inserted.
For patients with laryngeal trauma, tracheal trauma, or tracheal disruption, cricothyrotomy is inadvisable, and emergency tracheotomy is performed. Percutaneous transtracheal ventilation, a technique similar to needle cricothyrotomy, is an acceptable alternative in the treatment of these patients. In the trauma patient, continuous pulse oximetry monitoring is extremely helpful in determining the adequacy of oxygenation and is used in the care of all critically injured patients to allow early detection of arterial oxygen desaturation.
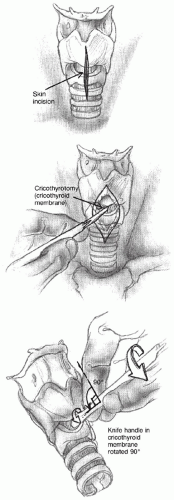 Figure 74.3 Cricothyrotomy. |
Breathing
Loss of respiratory drive among trauma patients is most commonly caused by severe head trauma. Ventilation is provided with a bag-mask until cervical spinal injury is ruled out. An endotracheal tube is then inserted, and mechanical ventilation begun. As part of the primary survey, injuries to the chest wall and structures within the thoracic cavity that can cause hypoventilation must be recognized and rapidly managed. These injuries include sucking pneumothorax, massive pneumothorax, and tension pneumothorax.
Sucking pneumothorax occurs when there is a defect in the chest wall larger than the tracheal diameter. Because of reduced resistance through this opening, inspiratory and expiratory efforts result in movement of air through the opening in the chest wall into the pleural space rather than through the trachea. Occluding the chest wall defect and chest tube placement followed by intubation with positive pressure ventilation is the best management of this injury.
Massive hemothorax is vented promptly. Although blood loss of 1,000 to 1,500 mL into the thoracic cavity almost always necessitates emergency thoracotomy, initial management is aimed at decompressing the chest cavity so that adequate ventilation can proceed. Tube thoracotomy is performed by means of making an incision at the fourth or fifth intercostal space in the midaxillary line (Fig. 74.4). A short subcutaneous tunnel is developed by means of finger dissection, and the tube is passed posterosuperiorly along an intrapleural tract toward the pleural apex. Continued hemorrhage at a rate of greater than 200 mL/h is an indication for thoracotomy.
Tension pneumothorax develops when a pleural, bronchial, or tracheal tear allows air to be forced into the pleural space without a means of egress. The result is collapse of the ipsilateral lung. As pleural pressure increases, the mediastinum and trachea shift to the opposite side, compress the contralateral lung, and compromise oxygenation. The mediastinal shift kinks the inferior and the superior vena cava; the kink impairs venous return, and hypotension develops. Signs and symptoms of tension pneumothorax are acute shortness of breath, tracheal deviation away from the injury, increased resonance to percussion, distention of the neck veins, and decreased breath sounds over the injured hemithorax. Tension pneumothorax is a clinical diagnosis made on these clinical grounds. Diagnostic chest radiographs should not delay chest decompression as this may lead to the patient’s death. Tension pneumothorax is managed by means of allowing air to escape through needle thoracocentesis with a largebore, 12-gauge intravenous cannula inserted into the second intercostal space in the midclavicular line (Fig. 74.5), followed by definitive treatment with chest tube insertion. Pneumothorax also can cause hypotension owing to its effect on myocardial performance. Any patient who remains in shock after chest trauma needs empirical chest ventilation.
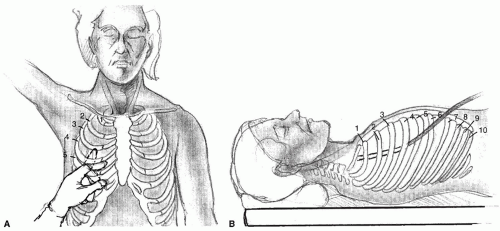 Figure 74.4 Tube thoracostomy. An incision is made in the fourth or fifth intercostal space in the midaxillary line. A: A short subcutaneous intrapleural track is developed by means of finger dissection. B: The tube is passed posteriorly and superiorly toward the pleural apex. |
Circulation and Shock
Once the airway and breathing have been reestablished, the next step is to assess the adequacy of the circulatory system. Shock is the clinical manifestation of the inability of the heart to maintain adequate circulation to vital organs. This low-flow state can be caused by cardiac dysfunction,
loss of blood volume, loss of vascular resistance, and an increase in venous capacity (13). The cellular response to shock is a shift from aerobic to anaerobic metabolism in nonvital organ systems. The result is lactic acidosis. If hypoperfusion persists, oxygen delivery to vital organs becomes inadequate, and acidosis deepens. Unless oxygenation and perfusion are restored, organ failure progresses, and the patient dies.
loss of blood volume, loss of vascular resistance, and an increase in venous capacity (13). The cellular response to shock is a shift from aerobic to anaerobic metabolism in nonvital organ systems. The result is lactic acidosis. If hypoperfusion persists, oxygen delivery to vital organs becomes inadequate, and acidosis deepens. Unless oxygenation and perfusion are restored, organ failure progresses, and the patient dies.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


