Primary Open-Angle Glaucoma
Anjana Jindal
Scott Fudemberg
Definition
Primary open-angle glaucoma (POAG) is an optic neuropathy with characteristic neuroretinal rim loss; it is associated with certain risk factors, most notably increased intraocular pressure. The defining criteria for glaucoma have changed with our evolving understanding of its critical elements. In 1938, Barkan proposed that glaucoma be classified into open- and narrow-angle forms.1 This classification scheme is especially valuable because it highlights a difference in etiology that significantly affects management. Narrow-angle glaucoma typically responds to iridectomy or iridotomy whereas open-angle glaucoma does not. Among open-angle glaucomas, primary open-angle glaucoma is a diagnosis of exclusion and may be diagnosed only when no identifiable secondary cause is determined. For example, evidence of pseudoexfoliation syndrome in a patient with open-angle glaucoma makes the diagnosis of pseudoexfoliation glaucoma instead of primary open-angle glaucoma. However, some patients may exhibit features of more than one type of glaucoma and should therefore be considered as having mixed-mechanism glaucoma. A patient may have narrow but open anterior chamber angles and elevated intraocular pressure. In these cases, peripheral iridotomy is likely to widen a narrow angle but unlikely to significantly lower intraocular pressure. Additionally, some patients may manifest features of multiple types of secondary glaucoma. Ultimately, correct classification of glaucoma is important because management strategy may be significantly altered depending on the diagnosis of specific types of glaucoma.
Primary open-angle glaucoma is an acquired condition characterized by (i) open anterior chamber angle, with normal gonioscopic appearance; (ii) chronic progressive loss of retinal ganglion cells, manifested by a characteristic optic neuropathy; and (iii) typical patterns of visual field loss in the more advanced stages. The classic requirement for elevated intraocular pressure (IOP) is dropped from the modern definition. Essential to the modern understanding of glaucoma is the concept that no “normal” intraocular pressure exists. There is no intraocular pressure that is known to be protective for all patients. The Ocular Hypertension Treatment Study (OHTS) highlighted the fact that many patients with seemingly elevated IOP do not develop other features of glaucoma.2,3 Likewise, the Collaborative Normal-Tension Glaucoma Study found that even some patients with seemingly normal IOP will experience glaucoma progression.4,5 Nonetheless, it is highly unlikely that patients with very low IOP would get worsening glaucoma, but very low IOP is often poorly tolerated causing pathologic hypotony. With the caveat of very low IOP aside, there is no level of IOP that guarantees no glaucoma progression. Although there is no normal IOP, average IOP is well documented. Average (mean ± standard deviation) IOP is 15.5 (±2.57) mm Hg.6 Assuming a Gaussian distribution in which two standard deviations include the values of about 95% of the population, an IOP of 20.5 mm Hg (mean plus two standard deviations) could be used as the upper limit of normal IOP. Although the distribution of average IOP is skewed toward the higher range, this statistical definition was widely accepted and previously used in the definition of POAG.
Important risk factors include IOP, race, age, family history, and central corneal thickness. POAG affects both eyes but often asymmetrically. In early and even in moderate stages, the patient is usually asymptomatic. Abnormalities of the visual field occur insidiously and typically initially involve the midperiphery. In advanced stages, the patient may become aware of an enlarging scotoma, particularly when it encroaches on fixation. If left untreated, vision may be lost. The natural history of the disease is one of a slowly progressive optic neuropathy. It has been estimated that untreated glaucoma can take an average of 14.4 years to progress from early to end stage at an IOP of 21 to 25 mm Hg, 6.5 years at 25 to 30 mm Hg, and 2.9 years at more than 30 mm Hg.7
Differential Diagnosis of Primary Open-Angle Glaucoma
Glaucoma is not the only condition with optic nerve cupping and visual field loss. Other conditions, both congenital and acquired, can mimic glaucoma.
Physiologic optic nerve cupping: typically normal IOP, large optic nerve, and static appearance
Congenital disc anomalies: optic nerve coloboma8 (Fig. 1), congenital pit9,10 (Fig. 2), and tilted disc syndrome11(Fig. 3)
Average- (normal-) tension glaucoma
Ocular hypertension
Secondary open-angle glaucoma: e.g., pseudoexfoliation, pigment dispersion, steroid-induced, lens particle, and so on
Previous glaucomatous damage: due to prior episodes of elevated intraocular pressure, e.g., from trauma, uveitis, steroids, that have resolved. IOP is normal and optic nerve appearance remains static.
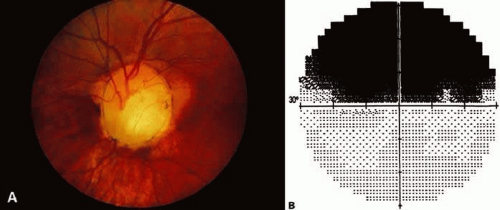 Figure 1. Optic disc coloboma and associated visual field deficit can resemble glaucoma. A. Optic disc coloboma. B. Corresponding Humphrey visual field defect. (Courtesy of Wallace L.M. Alward, M.D., Iowa City, IA.) |
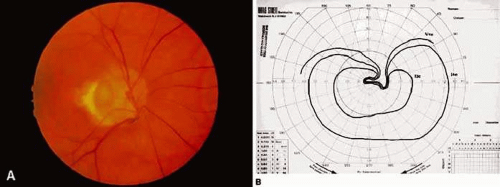 Figure 2. Congenital optic nerve pit and associated visual field deficit can resemble glaucoma. A. Congenital optic nerve pit. B. Corresponding Goldmann visual field defect. (Courtesy of Wallace L.M. Alward, M.D., Iowa City, IA.) |
 Figure 3. Tilted disc can resemble myopic, glaucomatous disc. (Courtesy of Wallace L.M. Alward, M.D., Iowa City, IA.) |
These conditions can have optic nerve and visual field changes that look similar to glaucoma. In addition, congenital anomalies can interfere with recognition of glaucomatous damage when they coexist with glaucoma. Young age, highly asymmetric or unilateral disc changes, atypical visual fields, or visual fields that do not correspond to the disc changes should increase the examiner’s suspicion of a nonglaucomatous cause.
Ocular Hypertension
Ocular hypertension refers to IOP elevated more than the statistically normal range with normal anatomy and without evidence of characteristic glaucomatous optic nerve damage or visual field abnormalities. It has been estimated that 4% to 7% of people older than age 40 years have elevated IOP without detectable glaucomatous damage on standard clinical tests.15 Those with ocular hypertension are often referred to as glaucoma suspects because the risk of glaucoma increases with elevated IOP; they need to be followed on a routine basis16,17,18 These patients often provide a challenge as to whether and when to treat since there is great variability in who goes on to develop glaucoma. Data from the OHTS study suggest that approximately 10% of untreated ocular hypertensive patients with IOP consistently greater than 24 mm Hg will develop glaucoma in 5 years. The study also showed that the cumulative risk for progression to glaucoma was 4.4% in the treated group compared to 9.5% in the observation group.19 The decision on whom to treat and when to treat should be based on individual risk factors such as age, central corneal thickness, IOP, optic nerve appearance, and family history.
Average- (Normal- or Low-) Tension Glaucoma
Average-tension glaucoma occurs in a subset of patients who have POAG and may be described as a primary, acquired, progressive optic neuropathy characterized by typical patterns of cupping and visual field changes. It is distinguished from POAG by the absence of IOP elevated above the statistically average range. There are those who believe that average-tension glaucoma and POAG do not represent two separate entities but different places in the spectrum of the same disease process. Alternately, proponents of separating average-pressure glaucoma and primary open-angle glaucoma note some significant clinical differences such as greater likelihood of disc hemorrhages and denser, steeper, more localized visual field defects closer to fixation.20,21,22
Glaucoma Suspect
A person is considered a glaucoma suspect if, in the presence of a normal open angle on gonioscopy, he or she has one or more of the following: (i) suspicious optic nerve (glaucomatous appearing neuroretinal rim thinning, asymmetric glaucomatous neuroretinal rim thinning, notching or loss of the neural rim, or glaucomatous appearing nerve fiber layer thinning), (ii) consistently elevated IOP, or (iii) visual field abnormality consistent with glaucoma. The presence of family history of glaucoma, particularly a strong family history, may also merit consideration of a patient as a glaucoma suspect.
Pathogenesis
The pathogenesis of elevated intraocular pressure and optic nerve atrophy with characteristic glaucomatous cupping are incompletely understood. Elevated IOP is believed to result from abnormal resistance in the aqueous outflow system.23 Aqueous production is not believed to play a pathologic role in glaucoma. Histopathologic studies of the outflow structures uncovered potential mechanisms of outflow reduction in glaucoma.24
Other studies have addressed mechanisms of optic nerve atrophy and cupping in glaucoma.25 Theoretical mechanisms for glaucomatous optic neuropathy include mechanical, vascular, and cellular factors. The mechanical theory proposes a direct pressure-induced damage to the retinal ganglion cell axons at the level of the lamina cribrosa. The vascular theory proposes microvascular changes and resultant ischemia in the optic nerve head. The cellular theory postulates that damage from mechanical stress on the retinal ganglion cells and/or insufficient blood flow ultimately must be mediated through astrocytes of the optic nerve head.1 (1)
Mechanisms of Elevated Intraocular Pressure
Morphologic alterations in the extracellular matrix of the aqueous outflow system in patients with glaucoma have been described in detail.26,27,28 Briefly, these changes include nodular proliferation of extracellular collagen, fragmentation, and “curling” of the collagen fiber bundles.26 There is an increase in glycosaminoglycan content but an overall decrease in hyaluronic acid.29 The endothelial cells lining the trabecular meshwork show foamy degeneration with basement membrane thickening.28 Ultrastructural changes in the juxtacanalicular tissue—the outermost aspect of the trabecular meshwork, which is believed to be the most likely site of obstruction in glaucoma—have also been described.26,30,31,32 There is accumulation of nonfibrillar material with characteristics of basement membrane, curly collagen, and chondroitin sulfate protein complex. Changes in matrix vesicles (extracellular lysosomes), sheath material from subendothelial elastic-like fibers, extracellular glycoprotein, fibronectin, and elastin have been reported.32,33,34,35,36 Specificity of some of the morphologic changes has been questioned because similar findings have been noted in normal, aged eyes without glaucoma.31 This has led some to speculate that glaucomatous changes in the outflow pathway may represent an accelerated aging process.37
In addition to the changes in the trabecular meshwork, collapse of the Schlemm canal has been invoked as another mechanism of outflow obstruction.38,39 To support this hypothesis, adhesions between the inner and outer walls of the Schlemm canal have been shown.26,38 There is a certain amount of segmental variability in histopathologic specimens, however.40
Finally, differences in composition of the aqueous have been suggested as another mechanism for increased outflow resistance. Transforming growth factors (TGFs) are polypeptides with multiple cellular regulatory functions. TGFs can inhibit epithelial cell proliferation, induce extracellular matrix protein synthesis, and stimulate mesenchymal cell growth. Elevated levels of TGF-β2 have been found in the aqueous of glaucoma eyes.41 The study speculated that increased TGF-β2 levels may be responsible for the decreased cellularity of the trabecular meshwork and may lead to increased debris and resistance to outflow. Others report decreased collagenase activity, increased collagen synthesis, and elevated levels of metalloproteinase-1 inhibitor in the aqueous of glaucoma eyes.42 The study suggests that the decrease in collagen degradation may lead to excess deposition of collagen and loss of the trabecular meshwork cells in glaucoma. Despite these studies, the detailed cellular events and molecular substrates that lead to abnormalities of outflow resistance in glaucoma remain poorly understood.
Molecular genetic studies of large families with juvenile open-angle glaucoma have led to identification of the first glaucoma gene (GLC1A) in chromosome 1.43 Interestingly, about 3% of patients with typical adult-onset POAG also have a mutation in the GLC1A gene.44 This suggests gene mutation is responsible for a small but significant portion of POAG. Cellular and molecular events that lead to a defective GLC1A gene and cause elevated IOP and glaucoma remain an active area of research.
Mechanism of Optic Nerve Damage
Historically, glaucomatous optic nerve damage has been attributed to either a mechanical, vascular, or cellular etiology. It is unlikely, however, that any one theory alone will fully explain the optic nerve damage in glaucoma.
Mechanical Considerations
Both in vitro and in vivo studies have shown that elevated IOP can cause posterior bowing of the lamina cribrosa, the collagenous structure that supports the retinal ganglion cell axons as they exit the eye.45,46,47 The lamina cribrosa is made up of about 10 parallel plates, each with various-sized pores that allow bundles of axons to pass through and yet maintain the competence of the eye to hold pressure. Evidence suggests that the plates of the lamina cribrosa are compressed in POAG and may even be entirely collapsed in some cases.48 Such physical distortion of the lamina cribrosa is thought to damage the passing axons by distortion or kinking. Other studies have shown elongation of the pores within the lamina cribrosa, suggesting mechanical forces that may stretch and fragment smaller beams.49 Changes in the extracellular matrix have been described that may lead to the loss of structural support in the lamina cribrosa.50,51,52,53 These changes include basement membrane thickening, disorganized and fragmented laminar beams, increased level of certain types of collagen, and structural changes in elastin. Interpretation of these morphologic changes within the lamina cribrosa should be done cautiously because they may represent secondary rather than primary changes in glaucoma.
There is evidence that elevated IOP can impede axoplasmic flow within the retinal ganglion cell axon.54,55,56,57 Axonal transport is vital to the normal functioning of neurons; retrograde axonal transport of target-derived neurotrophic factors may be essential for cell survival.58,59 It has been suggested that elevated IOP may lead to the degeneration of retinal ganglion cells by interfering with retrograde axoplasmic flow of essential neurotrophic factors. Lack of neurotrophic factors may trigger apoptosis (programmed cell death) in the retinal ganglion cell (see Cellular Mechanisms of Ganglion Cell Death).
Vascular Considerations
Proponents of the vascular theory argue that microvascular changes in the optic nerve head are responsible for glaucomatous optic nerve damage.60 Blood supply to the prelaminar and laminar areas of the optic nerve is derived from the peripapillary choroid and short posterior ciliary arteries.61 The vascular supply to the anterior optic nerve may be compromised in glaucoma by several different mechanisms:
The capillary network of the optic nerve head may be selectively lost in POAG.62 However, research also shows that the retinal ganglion cell axons and the capillary network may be lost at the same rate, suggesting there is no selective loss or pre-existing damage to the capillary network.63
Hayreh64 noted the importance of the “watershed” zones of the choroidal blood supply. The watershed zones refer to the border areas between various choroidal segments, each supplied by a short posterior ciliary artery. The watershed zones represent potential areas of compromised circulation and can include the optic nerve head. In addition, nocturnal systemic hypotension has been proposed as an additional risk factor for the development of glaucoma.65
An epidemiologic association between POAG and systemic microvascular disease (e.g., diabetes mellitus) has been reported.66 However, other studies have failed to show a significant correlation between POAG and diabetes.67,68
There is some evidence that autoregulation of blood flow in the optic nerve head is altered in POAG.69,70 Autoregulation is an important mechanism by which arterioles dilate or constrict with the rise or fall in perfusion pressure to maintain constant blood flow to the retina. In glaucoma, this autoregulatory mechanism may be defective and may predispose the optic nerve to ischemic damage.
Cellular Mechanisms of Ganglion Cell Death
There is increasing interest in elucidating the cellular and molecular events that lead to retinal ganglion cell death in glaucoma. Apoptosis is a process by which excess neurons undergo spontaneous degeneration during normal development. Apoptosis has been demonstrated in primate71 and rat models of glaucoma.72,73 These studies suggest that elevated IOP may trigger cellular events leading to apoptosis. One hypothesis is that elevated IOP impairs the retrograde axonal transport of essential neurotrophic factors74,75 and in turn triggers apoptosis of the retinal ganglion cell.
Glutamate is an excitotoxic amino acid that normally functions as a neurotransmitter in the retina. Ischemia can produce excess levels of extracellular glutamate, which may lead to cell death through a complex series of cellular events that involve glutamate receptors and Ca++ influx into the cell.76,77,78 Elevated levels of glutamate in the vitreous have been demonstrated in glaucomatous monkeys and humans, garnering support for this theory.79 It is unclear whether the accumulation of vitreal glutamate is a primary or secondary process in glaucoma.
Epidemiology
Glaucoma is a significant public health problem. It is the second leading cause of blindness in the United States.80,81 An estimated 2.22 million Americans have glaucoma, and about 150,000 are legally blind.15,82,83,84 This number is expected to increase as the proportion of older people in the population continues to grow. In the older black population, glaucoma is the leading cause of blindness, and the risk of blindness from glaucoma is 6.6 times greater than that population of white Americans.84 Worldwide, glaucoma is also the second leading cause of blindness. The World Health Organization (WHO) estimated the incidence of newly diagnosed POAG at 2.4 million per year, with 3 million individuals blind from glaucoma.85 In Nigeria, up to 34% of glaucoma patients may be blind in both eyes and 91% blind in at least one eye.86
Prevalence and Incidence of POAG
Population-based studies show that the prevalence of POAG ranges from 0.4% to 8.8% in those older than age 40 years (Table 1).87,88,89,90,91,92,93,94 On average, POAG is found in 1.9% of white and 0.58% of Asian populations. In black populations, however, the prevalence is significantly higher at 6.7%. Although some of the difference can be attributed to epidemiologic study design and the precise definition of POAG, the significantly higher rates observed in Western African populations probably reflect a fundamental risk factor associated with race (see Risk Factors).
Table 1. Population-based Prevalence Studies of Primary Open-angle Glaucoma | ||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
The incidence rate of POAG is not precisely known. An annual incidence rate of 0.24% was reported in a Swedish population.95 Conversely, several studies have reported incidence rates of glaucoma in patients with ocular hypertension (Table 2).96,97,98,99,100,101,102,103,104,105 Ocular hypertension is a well-known risk factor for the development of glaucoma (see Risk Factors). Reported annual incidence rates vary from 0% to 7%; on average, about 1.7% of ocular hypertensive patients become glaucomatous annually.
Table 2. Incidence of POAG in Ocular Hypertension | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Risk Factors
Several risk factors for the development of POAG have been identified based on statistical analysis of population-based prevalence studies. Of these, elevated IOP, older age, black race, and positive family history are most strongly correlated with POAG. Other factors such as myopia, diabetes mellitus, systemic hypertension, and migraine or vasospasm are less strongly associated or their association is not clearly established.
Intraocular Pressure
Both clinical and experimental studies suggest a strong correlation between elevated IOP and glaucoma. Clinically, elevated IOP, regardless of etiology, may produce optic nerve cupping and atrophy, with visual field loss often indistinguishable from that produced by POAG. Experimentally, elevated IOP in animal models of glaucoma can cause optic nerve cupping and atrophy similar to that seen in POAG.106 Furthermore, population-based studies have demonstrated a strong positive correlation between IOP and POAG (Fig. 4).16 However, it is critical to understand that, although average IOP has been determined for populations, no normal IOP exists. Average IOP in the United States is 16 mm Hg with a standard deviation of 3.107 Therefore, about 96% of the U.S. population has an IOP between 10 and 22 mm Hg. Studies have shown that as many as 30% to 50% of individuals with initial screening IOPs less than 22 mm Hg have glaucomatous neuropathy and/or visual field loss.
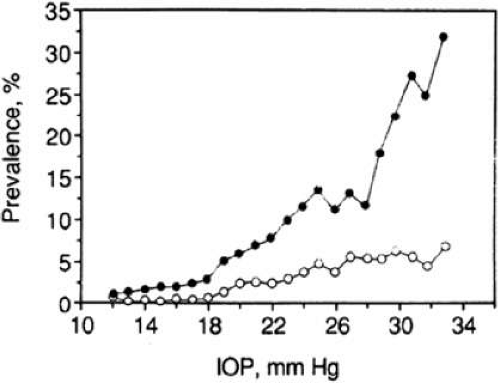 Figure 4. Prevalence of primary open-angle glaucoma as a function of screening IOP (white Americans [open circles], black Americans [closed circles]). (Reprinted with permission from Sommer A, Tielsch JM, Katz J et al: Relationship between intraocular pressure and primary open angle glaucoma among white and black Americans. The Baltimore Eye Survey. Arch Ophthalmol 109(8):1090, 1991.) |
Variability in IOP is also seen. The IOP in untreated glaucomatous eyes can vary by an average of 4.8 to 11.3 mm Hg or more in a 24-hour period, whereas most patients without glaucoma show a diurnal range of 5 mm Hg or less. Most individuals manifest a regular daily pattern, with peak pressure most commonly in the first few hours of wakening. However, 10% to 20% of patients are erratic, with variable patterns of diurnal IOP.108 Diurnal and long-term fluctuation of IOP were previously thought to be independent risk factors for the progression of glaucoma109,110 and visual field progression111; however, recent studies have shown this to be untrue.112,113
Central Corneal Thickness
Corneal thickness and resistance is known to affect IOP measurement. Average central corneal thickness (CCT) is approximately 545 microns (measured by ultrasound) in normal eyes. Increased CCT may give artificially high IOP, and decreased CCT may give artificially low IOP.114,115 Although numerous theoretical formulas exist, the exact effect of corneal thickness on IOP is not known. Thus, converting measured IOP using algorithms that account for CCT is not currently useful. At this point, CCT is best applied to clinical scenarios by differentiating measurements into groups (thick, average, or thin) with corresponding impact on risk of glaucoma progression (less, no change, or more, respectively). Analysis of the Ocular Hypertension Treatment Study showed that participants with a CCT less than 555 microns had a threefold greater risk of developing POAG compared with participants with CCT greater than 588 microns.116
The Ocular Hypertension Treatment Study (OHTS) also demonstrated thinner central corneal thickness to be a positive predictor of POAG in both univariate and multivariate analysis.2 It is likely that the predictive value of corneal thickness is due to its effect on measured IOP, but CCT has also proved to be a risk factor for glaucoma independent of IOP. Perhaps thin CCT is a clue to structural differences in some eyes that predispose to glaucoma. Although the implications of CCT on risk of glaucoma progression are established, more work is necessary to understand why.
Age
Population-based studies demonstrate a statistically significant association between prevalence of glaucoma and advancing age. In the Baltimore Eye Survey, individuals between 70 and 79 years of age were 3.5 times more likely to have glaucoma than participants aged 40 to 49 years (Table 3). This correlation between age and glaucoma prevalence was even stronger for black participants.88 IOP is a confounding factor, however, because it may also increase with age.117 It is possible that increased prevalence of glaucoma in older age groups may be due to increased IOP. It is unclear why aging increases the risk of developing glaucoma.
Table 3. Prevalence of POAG and Ocular Hypertension by Age | ||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||||
Ethnicity
Black race is an important risk factor (Tables 1 and 4, Fig. 4). In Baltimore, the prevalence of POAG is 6.6 times higher in black Americans compared with white Americans.84 Collectively, several population-based studies have also shown that the prevalence of POAG among blacks is consistently higher than among whites (Table 1). This is true even when glaucoma prevalence is adjusted for IOP (Fig. 4) and age (Table 4). The data strongly suggest an inherent predisposition of Western African descent to development of POAG. In the OHTS, blacks were associated with a 59% risk of developing POAG in univariate analysis; however, after inclusion of baseline vertical cup–disc ratio or corneal thickness in the multivariate analysis, this was no longer significant.2
Table 4. Prevalence of POAG by Age and Race | ||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||
Family History
Positive family history is another important risk factor. The Baltimore Eye Survey reported an age/race-adjusted odds ratio of 2.85 for an association between POAG and history of glaucoma in a first-degree relative. This association was strongest in siblings (age-adjusted odds ratio of 3.69) and weakest in the children of study subjects (age-adjusted odds ratio of 1.12).83 The population-based Rotterdam Study found that the risk ratio of glaucoma among first-degree relatives of glaucoma patients was 9.2.90,118 Other studies have found similar findings.119,120
Minor Risk Factors
Several clinic-based studies suggest that myopia is more frequent in ocular hypertension and glaucoma than would be expected in a normal population.121,122,123 However, the link between myopia and POAG is controversial. Elevated IOP is statistically associated with myopia, but this does not fully explain the higher prevalence of glaucoma in myopia, suggesting that myopia itself is a risk factor.124 In contrast to the other studies, the OHTS did not find an association with myopia and POAG.2 The mechanisms by which myopia predisposes to the development of POAG remain unclear. Myopic patients seek eye care earlier than emmetropic patients, so selection bias may contribute to the connection between glaucoma and myopia. Additionally, atypical optic nerve appearances and myopic fundus changes may make determination of glaucomatous optic nerve damage difficult.
Several studies reported higher prevalence of diabetes mellitus in POAG.125,126,127,128,129 Other studies such as the Framingham Eye Study, Baltimore Eye Survey, and the Ocular Hypertension Treatment Study failed to find such an association.67,68 The Framingham Eye Study determined diabetes by the presence of diabetic retinopathy, whereas the Baltimore Eye Survey and the OHTS relied on a history of diabetes provided by the patient. In addition, OHTS excluded individuals with diabetic retinopathy. All may have underestimated the true prevalence of diabetes. More recently, the Rotterdam Study reported a significant association between POAG and newly diagnosed diabetes mellitus.66 Although it seems plausible that microvascular changes in diabetes could predispose the optic nerve to glaucomatous damage, direct experimental evidence for this is still lacking. As with myopia, selection bias may contribute to an association between diabetes mellitus and glaucoma.
Systemic hypertension may be another risk factor for POAG.130,131 The Rotterdam study found a significant association between elevated systolic blood pressure and POAG but not with normal-tension glaucoma.66 The Baltimore Eye Survey suggested that this relation might be more complex.132 Although both diastolic and systolic blood pressures are modestly associated, the lower perfusion pressure (blood pressure minus IOP) was most strongly associated with POAG.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


