Prevention and Management of Complications of Glaucoma Surgery
Augusto Azuara-Blanco
L. Jay Katz
INTRODUCTION
This chapter will review the prevention and management of complications of glaucoma surgery. Some adverse events are specifically associated with an intervention, while other complications may appear after any time of glaucoma surgery. The general and specific complications will be addressed separately.
GENERAL COMPLICATIONS OF GLAUCOMA SURGERY
Intraoperative and Postoperative Suprachoroidal Hemorrhage
Suprachoroidal hemorrhage is a serious complication that can be seen during or after any intraocular surgery. If it occurs intraoperatively and cannot be controlled (i.e., expulsive hemorrhage), it can lead to loss of vision. The prevalence of this complication in the general population after cataract extraction is approximately 0.2%.1,2,3 The prevalence of suprachoroidal hemorrhage in glaucoma patients undergoing various types of intraocular surgery has been reported to be 0.73%.4,5,6,7 In the Tube versus Trab study (TVT)8 two patients (2%) and three (3%) patients developed suprachoroidal hemorrhage after tube and trabeculectomy surgery, respectively. Ocular risk factors for suprachoroidal hemorrhage include IOP, glaucoma, aphakia, pseudophakia, previous vitrectomy, vitrectomy at the time of glaucoma surgery, myopia, and postoperative hypotony. Systemic risk factors are arteriosclerosis, high blood pressure, tachycardia, and bleeding disorders or use of anticoagulants. The source of the hemorrhage is usually one of the posterior ciliary arteries, particularly the point of entrance of the short posterior ciliary vessels into the suprachoroidal space. There seems to be a vascular necrosis and subsequent rupture of the vascular wall.9
Intraoperative suprachoroidal hemorrhage can be associated with sudden collapse of the anterior chamber. The patient may complain of sudden pain breaking through the local anesthesia. If the process is gradual, a dark mass can be observed through the pupil to evolve slowly obscuring the red reflex; however, if the process is abrupt, the hemorrhage is more expulsive.
Postoperative suprachoroidal hemorrhage usually occurs within the first week after glaucoma surgery and is usually associated with postoperative hypotony (Fig. 24.1).4,5,6 The development of a suprachoroidal hemorrhage is typically acute and associated with the sudden onset of severe pain and decreased vision. Often this follows exertion with a Valsalva maneuver, such as straining in the bathroom. Examination of the anterior segment frequently reveals a shallow anterior chamber and a normal or high intraocular pressure (IOP). On fundus exam, a detached and dark choroid is noted, with loss of red reflex. The choroidal dome-shaped elevations have a dark reddish-brown color. Some cases present with bleeding into the vitreous cavity and, uncommonly, retinal detachment. Ultrasonography can be used to diagnose suprachoroidal hemorrhage when a fundus exam is not possible, and to monitor the liquefaction of the clot.
Intraoperatively, once a suprachoroidal hemorrhage has been identified, prompt and secure closure of the incision is the first goal of the treatment, with gentle reposition of prolapsed uvea. The surgeon’s finger can be used to tamponade the incision site temporarily while sutures are placed. Meanwhile, intravenous acetazolamide (500 mg) and mannitol 20% (1-1.5 g/kg) are administered. Once the eye has been closed, the anterior chamber can be reformed through the incision or a paracentesis tract. After this point, a conservative approach is probably appropriate. Some authors have advised immediate drainage of the hemorrhage through posterior sclerostomies (usually not possible because of rapid clotting), and at times, also combined with a vitrectomy in aphakic patients, especially if the hemorrhage is large. Prognosis for recovery of vision is good as long as the eye can be closed without loss of uvea.
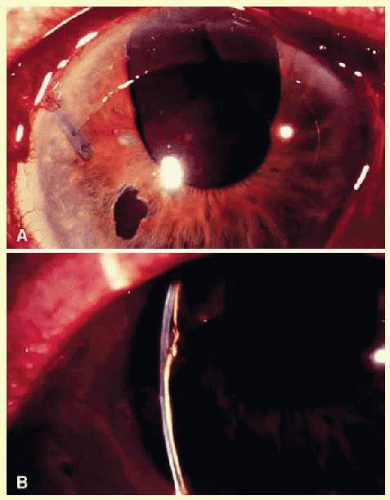 FIG. 24.1 Slit lamp photograph. A: Massive suprachoroidal hemorrhage after Molteno tube shunt implantation. The tube with an intraluminal suture in place can be seen. B: Slit beam illumination reveals a flat anterior chamber. |
Treatment of postoperative suprachoroidal hemorrhage is directed toward control of the IOP and relief of pain. The majority of these eyes will do well with this conservative management, and surgical drainage is not usually necessary.10 The indications for drainage include intolerable pain, a persistent flat anterior chamber, and massive “kissing” choroidal detachments. A waiting period of at least 8 to 14 days following a suprachoroidal hemorrhage is advised for the fibrinolytic response to liquefy the clot and allow for more effective evacuation of the suprachoroidal space. Drainage through a sclerotomy into the suprachoroidal space, with constant infusion of fluid into the anterior chamber, reveals liquefied blood, which is usually red or black. Occasionally, the fluid drained is a mixture of clear, straw-colored fluid and reddish to black liquefied blood. Bleeding into the vitreous cavity at the time of the hemorrhage and retinal detachment worsen the visual prognosis.
Prevention
Several steps can be taken in “high-risk” eyes: before surgery, correction of bleeding problems and discontinuation of inhibitors of platelet aggregation (i.e., acetylsalicylic acid) are recommended. Preoperative intravenous mannitol at the time of surgery should be considered. Prophylactic sclerostomies are indicated in those eyes with raised episcleral venous pressure. Use of viscoelastic and prompt (with preplaced scleral flap sutures) tight suturing of the scleral flap to prevent hypotony are recommended. The patient is urged to restrict activities (bending, weight lifting) and to avoid Valsalva-positive conditions (constipation, vigorous coughing, sneezing, or nose blowing) during the early postoperative period.
Hyphema
Hyphema is a common postoperative occurrence in glaucomatous eyes following filtration surgery, surgical peripheral iridectomy, trabeculotomy, and some new angle surgeries such as Trabectome.11 In the Collaborative Initial Glaucoma Treatment Study (CIGTS) study bleeding into the anterior chamber was the most common intraoperative complication (8%) and one of the most common incidents after trabeculectomy (10%).7 In the TVT8 and Advanced Glaucoma Intervention Study (AGIS)12 trials the frequency of hyphema was 8% and 11.4% respectively. Bleeding commonly arises from the ciliary body or cut ends of the Schlemm’s canal, although it might also arise from the corneoscleral incision or iris.
Intraoperatively, if a bleeding spot does not stop spontaneously, it must be identified and coagulated. If the bleeding persists it may be useful to close the scleral flap and temporarily increase the IOP. During filtration surgery, bleeding is minimized by performing the internal sclerostomy as far anterior as possible.
In general, postoperative hyphema presents within the first 2 or 3 days following surgery. In the vast majority of cases, no treatment is necessary, and the blood will be absorbed within a brief period of time. Cycloplegics, corticosteroids, restriction of activity, and elevation of head of the bed 30 to 45 degrees (to prevent blood from obstructing a superior sclerostomy) are recommended. Increased IOP can occur, particularly if the filtering site is obstructed by a blood clot, and it should be treated if necessary with aqueous suppressants. Injection of tissue-plasminogen activator may be considered. Surgical evacuation is also considered, depending on the level IOP, size of hyphema, severity of optic nerve damage, likelihood of corneal blood staining, and presence of sickle trait or sickle cell anemia (infarction of the optic nerve can occur at relatively low IOP, and carbonic anhydrase inhibitors are contraindicated). Liquid blood can easily be removed with irrigation. If a clot has formed, it can be removed by expression with viscoelastic or with a vitrectomy instrument set at low vacuum.
Hypotony
Due to the nature of glaucoma surgery, the operations that offer the lowest postoperative IOP are associated with the greatest risk of hypotony-related complications. Hypotony is more likely to occur when antifibrotic agents are used in filtration surgery. It seems to be more common in patients with inflammatory glaucoma and after cyclodestructive procedures. Hypotony can be defined as an IOP below a certain value (e.g., IOP < 6 mm Hg) or the presence of ocular abnormalities associated with low IOP. The possible mechanisms include excessive aqueous outflow (related to excessive filtration, wound leak, or cyclodialysis cleft) or to reduced aqueous production (related to ciliochoroidal detachment, inflammation, inadvertent use of aqueous suppressants, or extensive cyclodestruction).13,14 These conditions can coexist. For example, low IOP due to overfiltration can induce ciliochoroidal detachment and secondary decreased aqueous production. Possible complications include shallow or flat anterior chamber, gradual failure of the bleb, visual loss, cataract, corneal edema, Descemet’s membrane folds, choroidal effusions, suprachoroidal hemorrhage, macular and optic disc edema, and chorioretinal folds (predominantly in young myopic patients). According to Spaeth (Table 24.1), the severity of flat anterior chamber can be classified as grade I, when there is peripheral-iris apposition; grade II, with pupillary border-corneal apposition; or grade III, with lens-corneal touch (see Chapter 15). The central anterior chamber depth can also be described relative to the corneal thickness. Choroidal effusion occurs when fluid collects in the suprachoroidal space (Fig. 24.2), resulting in forward movement of the lens-iris diaphragm with anterior chamber shallowing. On fundus examination, moundlike elevations of the choroid, more commonly in the periphery, are visible.
TABLE 24-1 Classification of Flat Anterior Chamber | |
|---|---|
|
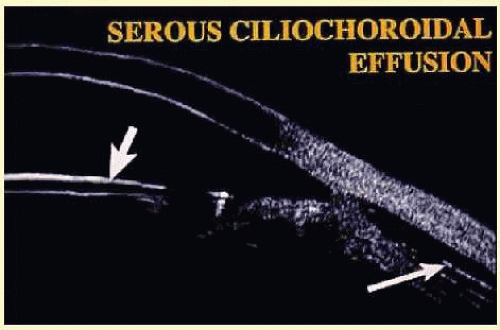 FIG. 24.2 Composite of ultrasound biomicroscopic examination. A peripheral choroidal effusion (large arrow) is seen as an acoustically hollow area in the suprachoroidal space. The anterior chamber is moderately shallow (small arrow: intraocular lens). |
Hypotony Maculopathy
Some patients with persistent intraocular hypotony develop loss of central vision secondary to marked irregular folding of the choroid and retina. Initially, these folds are broad and not sharply delineated. They tend to radiate outward in a branching fashion temporally from the optic disc, and concentrically or irregularly nasally to the disc. There may be swelling of the peripapillary choroid simulating papilledema (Fig. 24.3). The retina often shows a series of stellate folds around the center of the fovea. The retinal vessels are tortuous and sometimes engorged. The primary cause of visual loss is the marked folding of the central retina. Early detection of this condition is important because correction of the cause will usually result in visual improvement. In cases of prolonged hypotony, permanent pigmented lines caused by changes in the retinal pigment epithelium occur in the macular area and nasally. A postoperative bleb leak and a cyclodialysis cleft were formerly the most common causes of hypotony maculopathy. The incidence of hypotony maculopathy after glaucoma surgery has increased with the use of antifibrotic agents, specifically mitomycin-C. A direct toxicity effect of mitomycin on the ciliary body cannot be ruled out. The maculopathy is most likely to occur in young myopic patients, who may have a sclera more susceptible to swelling and contraction.15,16,17,18 In the TVT study hypotony maculopathy appeared in five (5%) cases after trabeculectomy and in one (1%) after tube surgery.8
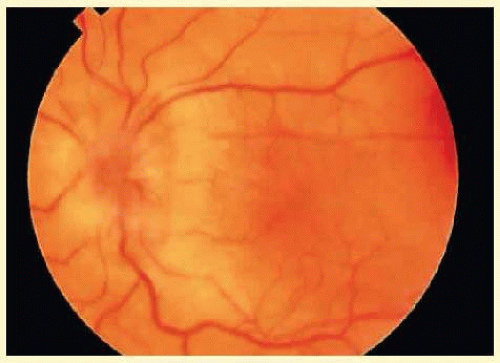 FIG. 24.3 Fundus photograph. Hypotony maculopathy with choroidal folds, retinal striae, and marked swelling of the peripapillary choroid simulating papilledema. |
Phthisis can occur in some complicated cases with severe chronic hypotony. The sclera shrinks and thickens, and the pull of the extraocular muscles deforms and squares the eyeball. There may be retinal gliosis and formation of a cyclitic membrane in the end stage. Ultimately, impairment of intraocular fluid dynamics results in corneal edema, cataract, calcification of the corneal epithelium, pigment epithelium, and inner choroid.
The initial management of early postoperative hypotony with a formed anterior chamber is conservative. Topical steroids and cycloplegics are used. Restrictions in activity (bending, weight lifting) and avoidance of Valsalva-positive conditions are recommended, especially in patients at risk for suprachoroidal hemorrhage. If there is hyposecretion related to intraocular inflammation and/or ciliochoroidal detachment, the initial treatment consists of intense corticosteroid therapy and long-acting cycloplegics that stabilize the blood-aqueous barrier. Intervention is indicated in cases with hypotony associated with other complications, and in persistent low IOP with loss of visual acuity and hypotony maculopathy. After filtration surgery, prompt management is also indicated when there is loss of bleb height. Treatment should be aimed at correcting the specific cause of hypotony. When there is lens-corneal touch (flat anterior chamber, grade III), immediate surgical intervention is necessary to prevent endothelial damage and cataract formation (see Chapter 15). Reformation of the anterior chamber with air, nonexpansile concentrations of gas, balanced salt solution, or preferably by viscoelastic can be done at the slit lamp or under the operating microscope through the paracentesis made intraoperatively. Viscoelastic material is best for maintaining, at least temporarily, the anterior chamber depth. When there are large and appositional choroidal effusions, drainage of the fluid may be necessary (Fig. 24.4). This technique is described in detail in Chapter 15.
 FIG. 24.4 B-scan ultrasound showing hyperreflective dome-shaped echoes, corresponding to the detached choroid-retina, with acoustically hollow content corresponding to the fluid accumulated in the suprachoroidal space. |
When hypotony is due to overfiltration of a filtering bleb, several options are available. A large bandage contact lens,19 symblepharon ring,20 and Simmons’ shell21 can be helpful. Several chemical and thermal treatments have been used to induce an inflammatory reaction in the filtering bleb, which modifies the morphology of the filtering blebs and increases the IOP. These procedures include topical application of 0.25% to 1% silver nitrate or 50% trichloroacetic acid to the bleb surface22 cryotherapy,23 diathermy and cauterization,24 argon laser,25 and Nd:YAG thermal laser.26 More than one treatment session might be needed to achieve the desired goal. Possible complications included postoperative discomfort, bleb leak, transient increase in IOP, and corneal edema. Nd:YAG thermal laser treatment of overfiltering and leaking blebs has been described as well. It is best done under regional anesthesia. For this procedure, the continuous-wave mode is required. Energy levels range between 3.0 and 4.0 J, with the laser offset between 0.9 and 1.2 mm, and the aiming beam focused in the conjunctival epithelium. The goal is to induce whitening and wrinkling of the conjunctival epithelium. A grid pattern of 30 to 40 spots of laser is placed over the entire bleb. Postoperatively, oral aqueous suppressants and a compressive or pressure patch (i.e., cotton plug placed directly over the bleb surface) may be used during the first 48 hours. Injection of autologous blood into the bleb can reduce overfiltration and resolve bleb leaks.27,28,29,30 Inflammatory cells and serum proteins from the injected blood may accelerate the inflammatory and healing process, which decreases filtration (Fig. 24.5). Possible complications include hyphema, endophthalmitis, increase in IOP requiring surgical intervention, bleb failure, corneal blood staining, and corneal graft rejection.31,32,33,34 Finally, surgical revision may be needed.35,36,37,38,39 Resuturing the scleral flap (and scleral patch grafting when resuturing is not possible) is most effective in cases with hypotony maculopathy associated with overfiltering filtering bleb. Transconjunctival suturing of the sclera flap is relatively simple and appears to be highly effective.40,41 Alternatively, two sets of stitches limiting the size of the bleb can also be helpful.
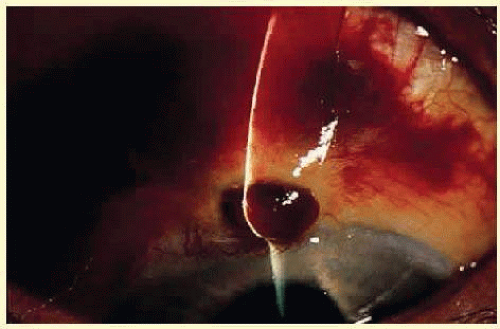 FIG. 24.5 Slit lamp photograph. Appearance of a filtration bleb after autologous blood injection, which was used to reverse chronic hypotony. |
Flat Anterior Chamber and Elevated or Normal Intraocular Pressure
Three conditions should be considered in cases with postoperative flat anterior chamber and elevated or normal IOP: suprachoroidal hemorrhage (see previous section), aqueous misdirection, and pupillary block.
Aqueous Misdirection
“Aqueous misdirection” also called “malignant glaucoma” or “choroidal expansion glaucoma” is characterized by a shallowing or flattening of the anterior chamber without pupillary block (i.e., in presence of a patent iridectomy) or choroidal pathology (e.g., suprachoroidal hemorrhage), commonly with an accompanying rise in IOP.42,43,44 It occurs in 2% to 4% of patients operated on for angle-closure glaucoma, but can occur after any type of incisional surgery. In the TVT study8 it occurred in three patients (3%) after tube surgery and one (1%) after trabeculectomy, while its incidence in CIGTS was 0.4% over 5 years.7 The chance of developing malignant glaucoma is greatest in phakic hyperopic (small) eyes with angle closure glaucoma.
In this condition, increased pressure at the vitreous cavity pushes the lens forward and flattens the anterior chamber.42 Decompression and shallowing of the anterior chamber appears to be a predisposing factor. In aqueous misdirection a relative resistance to the anterior movement of aqueous humor in the anterior vitreous face or the anterior hyaloid membrane probably occurs. The increased resistance can be related either to abnormal permeability or to available hyaloid surface area for fluid transfer. In normal circumstances, the anterior hyaloid and vitreous offer insignificant resistance to forward fluid flow. In some cases, pupillary block occurs first and is followed by aqueous misdirection.45 Choroidal expansion as a mechanism leading to aqueous misdirection has been proposed.46
Aqueous misdirection usually occurs in the early postoperative period after filtration or cataract surgery. The anterior chamber is shallow, and the IOP is high (Fig. 24.6). However, with a functioning filtration bleb, the IOP may not be elevated. The peripheral iridectomy is patent, and a dilated exam and B-scan ultrasound confirm the absence of choroidal effusion of hemorrhage. If the adequacy of the surgical iridectomy is in doubt and the pupillary block is possible, a laser iridotomy should be performed.
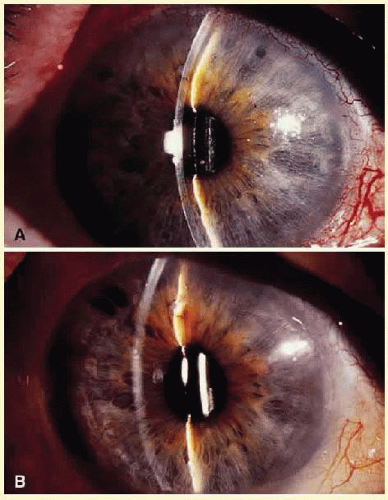 FIG. 24.6 Slit lamp photographs. A: Aqueous misdirection. The anterior chamber is very shallow. Two patent peripheral iridotomies are barely seen at the 10 and 1 o’clock positions. Intraocular pressure was 42 mm Hg. B: Same eye 4 weeks after pars plana tube insertion of aqueous shunt with vitrectomy. The anterior chamber is deep. The temporal iridectomy is enlarged. Intraocular pressure was 12 mm Hg. |
Medical treatment, laser surgery, and vitreous surgery have all been useful options to treat aqueous misdirection. This condition is initially managed with mydriatic-cycloplegic drops, aqueous suppressants, and hyperosmotics. Topical 1% atropine or 1% cyclopentolate four times daily and 2.5% phenylephrine four times daily are used. These agents will hopefully result in a posterior movement of the lens-iris diaphragm. In cases of aphakic aqueous misdirection, mydriatic-cycloplegic drops are of little benefit. However, it is reasonable to use them for their effect on relaxation of the ciliary body muscle. Systemic carbonic anhydrase inhibitors and topical beta-adrenergic blocking agents in full doses are important. Osmotics (isosorbide, glycerin, or intravenous mannitol) can also be helpful to decrease the fluid content of the vitreous cavity and can be given every 12 hours. If it is well tolerated and there are no contraindications, the medical treatment is tried for 2 to 4 days. If the condition is relieved (i.e., the anterior chamber has deepened), the hyperosmotic agents are discontinued first, and the aqueous suppressants are reduced or even stopped over several days. Phenylephrine drops can be stopped, but the cycloplegic drops should be continued for months to years or, in some cases, indefinitely to prevent the recurrence of this condition. Medical treatment relieves about 50% of cases of aqueous misdirection. If medical therapy is unsuccessful and the ocular media are clear, a Nd:YAG laser capsulotomy and hyaloidotomy can be used to disrupt the anterior vitreous face, especially in pseudophakic cases.47 The usual beginning laser energy is between 2 and 4 mJ. The focus is placed posterior to the anterior hyaloid. After a successful Nd:YAG hyaloidotomy a slight deepening that increases over the next few hours is usually seen. In pseudophakic eyes, a peripheral hyaloidotomy is more efficient than a central hyaloidotomy because the lens capsule and intraocular lens can prevent communication between the vitreous cavity and the anterior chamber. If not successful, peripheral iridectomy with zonulo-hyaloido-vitrectomy via the anterior segment is relatively simple and very successful.48 In phakic eyes, Nd:YAG hyaloidotomy can be tried through the peripheral iridectomy, focusing behind the zonules, but away from the ciliary body. However, a clear view and sharp focusing may not be possible, and there is a risk of lens or zonular injury. Pars plana vitrectomy should be considered when other therapies fail.49,50 A standard three-port pars plana vitrectomy, removing the anterior vitreous and part of the anterior hyaloid, is done. In phakic patients, the lens can sometimes be spared, but the probability of recurrence is higher. Pars plana tube shunt insertion with vitrectomy has been recommended to treat patients with aqueous misdirection, especially in cases with angle-closure glaucoma. The implantation of the tube shunt through pars plana can help prevent recurrence of this condition and can help in long-term control of IOP.50
Prevention
In high-risk eyes undergoing filtration surgery, the decompression and shallowing of the anterior chamber should be minimized. The use of viscoelastic and a large peripheral iridectomy can be helpful. Postoperative overfiltration should be avoided with a thick scleral flap sutured tighter and with more sutures than usual. Cycloplegics should be used routinely in high-risk eyes. Postoperatively, judicious suture lysis or cutting/pulling releasable sutures and slow tapering of cycloplegics are recommended. A postoperative shallow anterior chamber due to overfiltration should be vigorously treated.
Pupillary Block
Pupillary block can be caused by adhesions between the iris and the lens, pseudophakos, or vitreous. The inability of aqueous humor to pass from the posterior to the anterior chamber results in the forward movement of the peripheral iris and closure of the drainage angle. Pupillary block typically occurs as a flat or shallow anterior chamber with normal or elevated pressure. It may be difficult to distinguish from malignant glaucoma.
In a few cases, although a peripheral iridectomy is intended at the time of filtration surgery, only the stroma of the iris is removed and the posterior pigment epithelium is left intact. In these cases, blockage may develop. In other cases, the iris may become incarcerated in the wound, or the iridectomy may be obstructed by intraocular tissue, such as Descemet’s membrane, anterior hyaloid surface, vitreous (in aphakic eyes), or ciliary processes.
Therapy with cycloplegic-mydriatics may resolve pupillary block, but a Nd:YAG peripheral iridotomy should be done. The anterior chamber will readily deepen after iridotomy is performed, although in the presence of localized compartments of blockage, multiple iridotomies are necessary. This deepening is usually associated with the sudden escape of aqueous humor through the iridectomy and confirms the diagnosis of pupillary block. If laser iridotomy cannot be completed, a surgical iridectomy should be done.
Visual Loss
Unexplained loss of central visual field (i.e., “wipe out”) after glaucoma surgery is rare. Older patients with advanced visual field defects affecting the central field, with split fixation, are at increased risk. Early undiagnosed postoperative IOP spikes and severe postoperative hypotony have been suspected causes for “wipe out”.51,52,53
SPECIFIC COMPLICATIONS RELATED TO THE TYPE OF PROCEDURE
Complications of Guarded Filtration Procedures
Intraoperative Complications of Filtration Procedures
Conjunctival Buttonholes and Tears
Conjunctival buttonholes and tears can lead to bleb leak, failure of bleb formation, and flat anterior chamber. The usual cause for conjunctival buttonholes is penetration of the tissue by the tip of a sharp instrument (needle, scissors, blade) or the teeth of a forceps. Buttonholes and tears are more likely to occur in cases with extensive conjunctival scarring. To diagnose a buttonhole intraoperatively, the conjunctiva should be carefully examined at the end of the procedure by filling the anterior chamber and raising the filtering bleb. If recognized and if it is sizable, the buttonhole should be closed at the time of surgery. If it is located in the center of the conjunctival flap, a “pursestring” closure is attempted either internally on the undersurface of the conjunctiva or externally if the flap has already been reapproximated. A 10-0 or 11-0 nylon on a tapered (“vascular”) needle should be used. When the conjunctival buttonhole or tear occurs at the limbus, it can be sutured directly to the peripheral cornea. A mattress suture or, if large, a running suture with 10-0 nylon can be used. When the buttonhole or tear occurs near the incised edge of a limbal-based conjunctival flap, the sutures used to close the conjunctival incision can be placed posterior to the tear to close it.
Scleral Flap Disinsertion
A thin scleral flap can be torn or amputated from its base during the surgical procedure. If a sclerostomy has not yet been performed, a new scleral flap should be dissected in a different area. If a sclerostomy has already been done, reapproximation of the scleral flap can be attempted with 10-0 or 11-0 nylon sutures. If unsuccessful, additional tissue is usually necessary to cover the sclerostomy. This can be obtained by transferring a piece of Tenon’s capsule or a flap of partial-thickness sclera from the area adjacent to the defect. Alternatively, donor sclera, fascia lata, or pericardium can be used.
Vitreous Loss
Vitreous loss during glaucoma surgery is an uncommon complication, especially in phakic eyes. Conditions that may predispose to vitreous loss include high myopia, previous intraocular surgery, trauma, aphakia, and a subluxated lens. Loss of vitreous can be associated with several complications such as corneal edema, epithelial downgrowth, uveitis, retinal detachment, cystoid macular edema, and endophthalmitis. The vitreous can mechanically plug the sclerostomy and lead to filtration failure. Vitreous should be removed from the surgical site and anterior chamber with a vitrectomy instrument, avoiding damage to the lens in phakic eyes. In the aphakic eye with vitreous filling the anterior chamber, an anterior vitrectomy can be planned as part of the primary procedure. In phakic or pseudophakic eyes with vitreous in the anterior chamber, pars plana vitrectomy may be considered to adequately remove the vitreous from the posterior segment and to avoid lens/intraocular lens subluxation and lens injury.
Postoperative Complications of Filtration Procedures
Overall, severe visual loss is after guarded filtration procedure (trabeculectomy) uncommon, but the incidence of transient complications is high. In the CIGTS, early complications occurred in 50% of 465 trabeculectomies. The most frequent complications were shallow or flat anterior chamber (13%), encapsulated bleb (12%), ptosis (12%), serous choroidal detachment (11%), and hyphema (10%). Suprachoroidal hemorrhage occurred in 0.7% of cases, and there were no cases of endophthalmitis.7 In the United Kingdom, a national survey of trabeculectomy was conducted, and of 1,240 reported cases, early complications were reported in 46% and late complications in 42% of cases.54 The most common early complications were hyphema (24%), shallow anterior chamber (23%), hypotony (24%), wound leak (17%), and choroidal detachment (14%). The most frequent late complications were cataract (20%), visual loss (18%), and encapsulated bleb (3%).
Bleb Leak
Bleb leaks can occur early in the postoperative period or months to years after filtration surgery. The incidence of bleb leaks in the AGIS,12 CIGTS,7 and TVT8 studies ranged from 6% to 11%, but was much higher in both arms of the Fluorouracil Filtering Surgery Study (FFSS) study (20% to 32%).55 An inadvertent buttonhole in the conjunctiva during a filtering procedure or a wound leak, through the conjunctival incision, can be responsible for an early leaking bleb. Spontaneous late bleb leaks are more frequent in avascular, thin blebs, which occur more frequently when antimetabolites are used in the filtering procedure and after full-thickness procedures, especially mitomycin-C. The incidence of both early and late bleb leaks is higher in trabeculectomies supplemented with antimetabolites.55 Leakage of the filtering bleb can be associated with hypotony, shallow-flat anterior chamber, and choroidal detachment, and may increase the chances for bleb infection and subsequent endophthalmitis. Soltau56 reported infections occurring 25 times more frequently in leaking blebs than in intact blebs. Early leaking can flatten the bleb and lead to subconjunctival-to-episcleral fibrosis, which would jeopardize a satisfactory long-term filtration. In the Fluorouracil Filtering Surgery Study bleb leak was a risk factor for surgical failure.55
Bleb leaks are detected with the Seidel test (Table 24.2). The tear film is stained with fluorescein. For this purpose, a fluorescein strip is applied to the inferior tarsal conjunctiva or, very gently, directly to the bleb. Without applying pressure, the eye is examined under cobalt blue illumination. If there is a leak, unstained aqueous humor will be seen flowing into the tear film (Fig. 24.7). If there is no spontaneous leakage, pressure may be gently applied to the globe or to the bleb while the suspicious area is examined.
The need and urgency of the management of bleb leaks depend on several factors. Some cases, particularly in monocular individuals, with leaking blebs that have had previous episodes of bleb-related infections, ocular hypotony, shallow-flat anterior chamber, loss of bleb elevation, or reduced vision should be always treated. Alternatively, if there are no complications, such as in late leaks with formed blebs, normal IOP, good central vision, and without previous episodes of bleb-related infection, observation with prophylactic topical antibiotics is possible to allow spontaneous closure of the leak. However, in thin avascular blebs, recurrence of bleb leak is common. Pharmacological medical treatment with agents that decrease aqueous secretion and discontinuation of topical steroids, with or without patching, may accelerate the spontaneous closure of these defects by reducing flow of aqueous through the fistula. Patient education regarding symptoms of bleb-related ocular infection is crucial for prompt diagnosis and management.
TABLE 24-2 Seidel’s Test | ||||||||
|---|---|---|---|---|---|---|---|---|
|
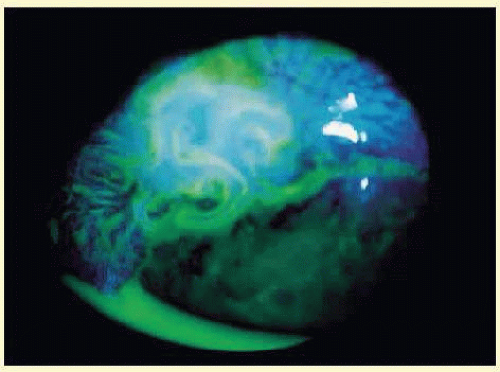 FIG. 24.7 Slit lamp photograph of a positive Seidel’s test. |
Therapeutic modalities to treat leaking blebs include pressure patching, bandage contact lens,19 Simmons’ shell,21 injection of autologous blood,27,28,29,30,31,32,33,34 cryopexy,23 thermal Nd:YAG laser,26 cyanoacrylate glue,57,58,59 fibrin tissue glue,60,61 and surgical revision.62 A large-diameter (17-20 mm), soft therapeutic contact lens can be helpful. The contact lens should be kept in place, if possible, for at least 1 week to allow reepithelization. Broad-spectrum topical antibiotics should be administered to protect against infection, and close observation is mandatory. Fibrin tissue glue is a mixture of fibrinogen and thrombin, which induces the formation of a clot that can seal bleb leaks.60,61,62,63,64 It is a nonirritating procedure that requires no patching. Tisseel (Immuno AG Industriestr, Vienna, Austria) is a commercialized fibrin glue, not U.S. Food and Drug Association approved, that has the disadvantage of being prepared from pooled plasma and thus may have the potential risk of transmitting blood-borne pathogens. Autologous fibrin tissue glue is prepared from the patient’s blood; therefore, eliminating the risk for disease transmission.61 The use of autologous serum drops for point-leaks or oozing through a thin bleb wall has recently been reported.65 Cyanoacrylate glue (Histoacryl, B. Brown Melsungen AG, Melsungen, Germany) adheres to tissues and can effectively close an early bleb leak seen shortly after surgery.57,58,59 However, the use of cyanoacrylate glue is not recommended in thin, avascular blebs with leaks developed months to years after surgery. The glue must be applied to a dry conjunctival surface, and only a small amount of glue should be used. The use of a bandage contact lens can prevent the adhesive from being dislodged.
When other simpler methods have failed, and the bleb leak is persistent, surgical intervention is necessary.66,67,68,69,70,71 It is important to attempt to save the established initial filtration site. Due to the friable nature of the conjunctiva in long-established filtering blebs, it is often impossible to close the defect directly with sutures, and, therefore, healthy conjunctival tissue is needed. First, the ischemic and thin-walled bleb tissue is denuded of conjunctival epithelium by blade debridement or gentle, mild cautery to allow long-term adherence of the grafted conjunctiva. Fresh conjunctiva adjacent to the bleb is then mobilized to cover the deepithelialized bleb by rotational, sliding, or free conjunctival grafts, depending on the dimension of the avascular area of the bleb and the quality of the surrounding conjunctiva. For conjunctival advancement,66,67 separate dissection of conjunctiva and Tenon’s capsule sometimes aids in closure because although conjunctiva can often be stretched further than Tenon’s, the closure of the latter provides more support. The conjunctiva is sutured over the previously abraded peripheral cornea, providing a watertight seal.68,69 With these methods, bleb function can be frequently preserved. Some surgeons prefer to remove the avascular area completely, but this approach may compromise the function of the filtering bleb. Free conjunctival graft from the inferior bulbar conjunctiva70 or amniotic membrane can be used as an alternative substrate.71 Hypotony associated with bleb leak presents difficult challenges. To plan surgical intervention, it must be determined whether hypotony is caused only by the leak. In cases with associated overfiltration additional sutures of the scleral flap or reinforcement with a patch graft would be necessary. The use of a donor patch graft (e.g., sclera, pericardium, cornea) is likely to compromise the function of the filtering bleb.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


