Chapter 15 Pre- and Postoperative Laryngeal Exam in Thyroid and Parathyroid Surgery
Introduction
 Please go to expertconsult.com to view related video Fiberoptic Laryngeal Exam: Laryngeal Anatomy and Function.
Please go to expertconsult.com to view related video Fiberoptic Laryngeal Exam: Laryngeal Anatomy and Function.
Thyroid surgery is a common procedure undertaken worldwide by a variety of surgeons ranging from a small number of highly specialized endocrine surgeons working in large-volume centers to general surgeons with a particular interest in endocrine surgery, a growing number of ear, nose, and throat (ENT) surgeons, and a vast number of general surgeons. Although there are differing patterns of performance of laryngeal exam, in part depending on the training of the surgeon, we feel that all patients undergoing thyroid and parathyroid surgery in this modern era should have pre- and postoperative exams.1
The majority of thyroid surgeries are performed outside large academic expert centers. A study in early 2000 found that in the United States, 50% of thyroid surgery is performed by surgeons who perform fewer than five cases a year.2 This reality is at odds with the known correlation between workload and outcome in thyroid surgery as in other subspecialties.3 Furthermore, obtaining informed consent before proceeding with an operation involves providing information about the risks of possible specific morbidity. Such information should be based on knowing one’s personal results/outcomes and can only be accurately obtained through reasonable volume.
For thyroidectomy, postoperative voice changes are the most common complication. Traditionally this risk has been quoted to be in small percentages, based on low figures derived from series of patients treated in centers with large endocrine practices and with variable postoperative laryngeal exam practices. In recent years, increased awareness and interest in this area have generated a plethora of publications on the topic. Furthermore, several professional bodies have started to make reference to voice and laryngeal function in their guidelines for best practice. This area will be increasingly debated as injury to the recurrent laryngeal nerve (RLN) represents the most common cause of litigation in endocrine surgery.4 A recent study by Abadin et al. showed that RLN injuries constituted 46% of all sources of thyroid surgery malpractice litigation between 1989 to 2009.5 Lydiatt stated that in unilateral vocal cord paralysis (VCP) lawsuits, four out of six (67%) were in favor of plaintiffs, and lack of informed consent was alleged in seven of nine (78%) cases.4
Surgeons operating on the thyroid may find the Journal of the American Medical Association (JAMA) editorial “Moral Wounds: Complicated Complications,” which details the patient’s perspective of posts thyroidectomy VCP, informative.6
Anatomy and Voice
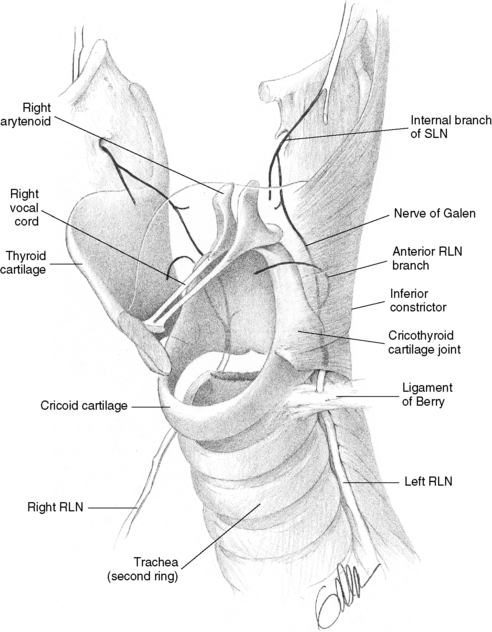
Voice is a very personal attribute dependent on signals from specialized areas of the central nervous system and involves coordinated movement of laryngeal muscles and resonance through the upper airways.7 The passage of air through the partially closed and tensed vocal cords triggers oscillations of the epithelial cover of the vocal cord (VC) (termed the mucosal wave). This process is maintained by the interplay of several factors (Table 15-1, Figure 15-1). The larynx is composed primarily of the upper shield–shaped thyroid cartilage, which has a left and right lamina and rests on the lower ring like cricoid cartilage through the cartilaginous cricothyroid joint posteriorly. The midline notch in the thyroid cartilage represents the “Adam’s apple.” The vocal cords are two folds of epithelium covered muscle projecting into the laryngeal lumen and are located approximately halfway down the thyroid cartilage. The two arytenoid cartilages, right and left, sit on the cricoid’s posterior lamina and are the posterior attachments of the vocal cords. These insert anteriorly into the inner surface of the midline thyroid cartilage. The basic motion of the arytenoids is rotational. When rotating laterally, they cause abduction of the vocal cords; when rotating medially, they cause adduction of the vocal cords. Laryngeal musculature can be divided into those muscles that result in vocal cord abduction and those that cause vocal cord adduction. The cricothyroid muscle on the outer surface of the larynx is the only laryngeal muscle present within the thyroid surgical field. In this position the cricothyroid muscle, when active, acts to tilt the thyroid cartilage followed on the underlying cricoid cartilage and in this way tenses the vocal cords, allowing for higher vocal registers and voice projection.
Table 15-1 Factors Contributing to Generation of Normal Voice
| Cartilages | Thyroid cartilage | Represents the anterior insertion of the VC Forward tilting of the thyroid cartilage onto the cricoid cartilage under the action of the cricothyroid muscle leads to increased tension of the VCs, allowing for higher vocal registries and voice projection |
| Cricoid cartilage | The posterior lamina offers support to the arytenoid cartilages (right and left) | |
| Arytenoid cartilages | Represent the posterior insertion of the VC When they rotate laterally they cause abduction of VC Medial rotation leads to adduction of VC | |
| Muscles | Thyroarytenoid muscle (vocalis muscle) | Represents the main muscular component of the VC and acts as an adductor |
| Adductors of VC | All intrinsic muscles of the larynx | |
| Abductors of VC | Posterior cricoarytenoid muscle | |
| Strap muscles | Sternohyoid, sternothyroid | |
| Nerves | RLN | Carries motor fibers to all intrinsic laryngeal muscles with the exception of cricothyroid muscle |
| EB-SLN | Innervates the cricothyroid muscle (see above) |
Any disruption in the luminal surface of the VC disrupts this process and leads to a coarse change to the character of the voice generically called hoarseness. The change to voice resulting from vocal cord paralysis is more accurately termed breathiness and represents a weakened voice caused by a relative glottis incompetence during phonation because of the lateral resting position typical for most paralyzed vocal cords (see Chapters 45, Pathophysiology of Recurrent Laryngeal Nerve Injury, and 46, Management of Recurrent Laryngeal Nerve Paralysis).
Mechanisms of iatrogenic RLN injury include mechanical, thermic, or vascular factors. Focal demyelination after minimal injury of RLN (e.g., compression) leads to a temporary blockage of nerve conduction (neuropraxia) that generally recovers completely and spontaneous after 6 to 8 weeks (see Chapter 33, Surgical Anatomy and Monitoring of the Recurrent Laryngeal Nerve). More severe trauma to the RLN (e.g., crush, stretch, or ischemic injuries) can damage the myelin sheath (axonotmesis), which can still recover spontaneously with greater delay and potentially less than normal function and possible synkinetic dysfunction. More violent trauma to the RLN (e.g., laceration or severe crush or stretch injuries) leads to interruption of the endoneurial, perineurial, or epineurial sheaths (neurotmesis), which is followed by incomplete or absent nerve regrowth.8
Because the external branch of the superior laryngeal nerves innervates the cricothyroid muscle, injury to this nerve can result in problems with the vocal projection and attainment of higher vocal registers. This nerve has also been termed the nerve of Amelita Galli-Curci after the famous operatic soprano whose career was brought to a ruinous end in 1935 as a result of thyroid surgery done under local anesthesia. The media wrote that postoperatively “the surprising voice is gone forever. The sad specter of a ghost replaces the velvety softness,” although the details are controversial.9 Endoscopic laryngeal findings may be quite subtle in external branch injuries and must be confirmed through cricothyroid muscle electromyographic studies (see Chapter 32, Surgical Anatomy of the Superior Laryngeal Nerve).
Reported Prevalence of Recurrent Laryngeal Nerve Paralysis
At the present time it is impossible to estimate how many patients have temporary or permanent VC paralysis after thyroid surgery. As long as clinicians continue to use voice symptoms as a screening for RLN injury and perform laryngoscopy only on a small subgroup of patients, the incidence of VC palsy will remain underreported. In addition to variability in laryngeal exam bias undoubtedly exists in the published literature in that existing published series generally represent favorable and therefore publishable results from expert units. The figures circulated in medical literature may therefore create false reassurance for patients and unwary surgeons. As noted earlier, in the United States 50% of thyroid surgeries are performed by surgeons who perform fewer than five such procedures per year.2
In a recent review of 27 articles and 25,000 patients, the rate of VC paralysis (VCP) varied widely according to the method of examining the larynx, and researchers found that the average temporary VCP rate was 9.8% and ranged from 2.3% to 26%.10 For this reason it is expected that anonymous reporting in nationwide audit databases should provide more accurate information. In Sweden, the Scandinavian quality register (SQR) reported, in 2008, 3660 thyroid operations performed within 1 year in 26 endocrine surgical units from Sweden and Denmark (units specializing in endocrine surgery) led to an immediate VCP rate of 4.3% nerves at risk.11,12 For the SQR, the rate of VCP doubled when patients were submitted to routine laryngeal exam as opposed to postoperative laryngoscopy, which was performed only in patients with persistent and severe voice changes. The third British Association of Endocrine and Thyroid Surgeons (BAETS) audit reported on a total of 10,814 cases of thyroid surgery and found an overall 2.5% rate of RLN palsy and a 4.9% incidence of voice changes. For first-time surgery, the reported incidence of RLN palsy was 1.4% after lobectomy and 3.7% after total thyroidectomy. These figures increased to 5.4% and 6.9%, respectively, in redo surgery.13 Such data are derived from the self-reported cases operated on by a group of endocrine surgical experts and as such might be too optimistic to be extrapolated to the overall practice of thyroid surgery. Further caution must be taken given that only 21.5% of patients reported in the BAETS audit had postoperative laryngoscopy, hence the RLN palsies reported likely represent only a portion of the total with post-thyroidectomy VC paralysis. Administrators of these two national databases deem the rates of temporary and permanent RLN paralysis to be severely underestimated.11,13
The recognition of vocal cord paralysis is important in that there have been substantial advances in the management of paralytic dysphonia and dysphagia, including the development of transcutaneous in-office injection procedures that are effective and safe.14–17 In the past, injection of polytetrafluoroethylene (Teflon) fell from favor because of problems of migration and granulomatous reaction. Such vocal cord injection is one of a number of techniques available for the management of postoperative vocal cord paralysis (see Chapters 45, Pathophysiology of the Recurrent Laryngeal Nerve Injury, and 46, Management of Recurrent Laryngeal Nerve Paralysis). Formal open thyroplasty involves a cervical skin incision and partial thyroid cartilage removal with placement of a Silastic implant or other spacer material lateral to the muscular substance of the vocal cord. This procedure may be combined with the arytenoid adduction, whereby the arytenoid cartilage is repositioned through suture placement to modify the desired vector of force on the repositioned paralytic cord so as to optimize voice. Simpler and less invasive injection thyroplasty may be less suitable for patients with large posterior glottic gaps and may be less durable. The simplicity, safety, and effectiveness of injection thyroplasty have resulted in a recent gain in its popularity.
Voice Symptoms with Normal Vocal Fold Mobility
Postoperative subjective and objective voice changes commonly occur in patients with intact vocal fold motility. Typical symptoms are transient and often consist of voice fatigue during phonation and difficulty with high pitch and singing voice associated with decrease in the speaking fundamental frequency and vocal range.18 The speech becomes more monotone and vocal pitch can be more than two semitones lower. Typically there is progressive normalization within 3 to 6 months postoperatively.18–20
In several large studies of patients without VC palsy, subjective voice complaints occurred in 30% to 87% of patients.12,21–25 In a prospective nonrandomized study of 100 patients, subjective voice changes occurred in one third of patients with preserved VC movement.12 In one prospective single-arm study of 54 patients, 30% of patients reported early subjective voice changes and 14% reported late (3-month) changes.22 A higher incidence of 50% was found in a larger study of 400 patients, but voice symptoms improved within 6 months in 85% of patients and within 1 year in 98%.23 In addition to the subjective findings a variety of objective voice analyses, abnormalities occur typically in fundamental frequency/frequency range, decreased maximum sound pressure, vocal jitter (increased vocal cord vibration cycle variability), and phonation time. These occur transiently and are seen postthyroidectomy without vocal cord paralysis in up to 84% of patients22,26 Though most agree there is progressive normalization of voice changes within 3 to 6 monthspostoperatively,19 there are reports suggesting that voice changes persisted up to 6 months in 87% of patients, mostly through voice fatigue, changes in pitch, and voice alterations when speaking loud or singing.25 One retrospective analysis with a mean of 4 years after uncomplicated thyroidectomy in 60 patients identified nonspecific voice changes in 28% and impaired swallowing in 15% of patients without vocal cord paralysis.27
The proposed mechanisms for voice alteration despite normal RLN function are insufficiently understood (Table 15-2). Direct cricothyroid muscle dysfunction by direct injury or transient wound fluid–related myositis may play a role. Also regional soft tissue changes may postoperatively affect the larynx, including edema, strap muscle retraction and denervation, and ultimately perilaryngeal scarring. Although strap muscle management during surgery could impact laryngeal function and therefore conceivably affect postoperative voice, one study found no relationship between strap muscle division and postoperative voice outcome.28 Strap muscles are known to activate during lower pitch vocalization.29 Certainly intubation-related30 vocal cord changes including short-term edema, vocal cord laceration, arytenoid dislocation, or more long-term vocal cord granuloma formation31 are all possible sources of vocal changes despite grossly normal neurologic function (see Table 15-2). Echternach et al. reported that a surprisingly high 42% of their patients undergoing thyroid surgery had laryngeal complications from intubation when an experienced otolaryngologist performed laryngeal exam 3 to 4 days after surgery.32 Most studies suggest lower rates of laryngeal trauma from intubation, ranging from 6% to 13%.30,33 The extent of surgical “trauma” seems important because the incidence and severity of voice and swallowing problems are significantly less severe in patients undergoing video-assisted thyroidectomy.34 There have been rare reports of endotracheal intubation in the setting of surgeries that did not involve the vagus or recurrent laryngeal nerve, independently causing vocal cord paralysis. It has been suggested that to cuff pressure on the more distal course of the anterior branch may result in such recurrent laryngeal nerve paralysis.35,36 It appears, however, that vocal cord paralysis specifically from endotracheal intubation is extremely rare, affecting less than 0.04%.27,37 A patient may also occasionally suffer from hoarseness postoperatively after thyroidectomy from intercurrent upper respiratory tract infection. This typically results in transient upper respiratory tract–related laryngitis. Such viral upper respiratory tract infections may rarely be associated with vocal cord paralysis (see Table 15-2).
Table 15-2 Factors That Can Lead to Postoperative Voice Changes
| Injury | Functional Consequence | Impact on Voice Character |
|---|---|---|
| Neural | ||
| RLN injury (complete or partial, transient or permanent) | Immobile and laterally displaced cord Inadequate closure of vocal cords with phonation and swallowing Loss of VC bulk and tone Bowing atrophy of vocal cord | Breathy voice Vocal fatigue Hoarseness |
| External branch of the superior laryngeal nerve (EB-SLN) injury (complete or partial, transient or permanent) | Posterior glottic rotation toward the paretic side Bowing of the vocal fold on the weak side and Inferior displacement of the affected cord | Easy voice fatigue Decreased pitch Inability to project voice |
| Non-Neural | ||
| Direct cricothyroid muscle injury—transient myositis or direct injury | As for EB-SLN | As for ESBLN |
| Regional soft tissue injury (in the presence of intact neurologic function) | Laryngotracheal regional scar with fixation Strap muscles denervation or trauma Local hematoma or edema | Voice fatigue Decrease in vocal range Vocal pitch can be lower |
| Intubation-related injuries | VC trauma (i.e., edema, hematoma, laceration) VC granuloma Arytenoid dislocation | Hoarseness Odynophagia |
| Voice change from unrelated intercurrent URTI | Typically viral-related laryngitis unrelated to surgery, rarely associated with VCP | Hoarseness, breathy voice if VCP |
Subtle voice changes are not easily volunteered by patients and may be difficult for unaware clinicians to pick up. The GRBAS scale (Grade, Roughness, Breathiness, Asthenia, Strain) provides a rating of voice over five key voice parameters including roughness, breathiness, asthenia, and strain. Each aspect is rated on a four-point scale ranging from 0 (normal) to 3 (severely abnormal). The scale is recommended for both clinical and research purposes by the European Laryngeal Research Group and has proved inter- and intraobserver reliability.38 The main limitation of this technique is the restricted access to services of specialized voice therapists able to offer accurate and reproducible assessments. Discrepancies between different assessors also highlight the need for better standardization of this technique.39 As a patient-centered tool, many have used the Voice Handicap Index (VHI) questionnaire. Patient self-assessment of VHI reliably identifies voice dysfunction after thyroidectomy: those with a change in VHI > 25 from the preoperative baseline warrant early referral to speech pathology and laryngology.40
In addition to voice changes, nonspecific swallowing symptoms may occur but are infrequently recorded or reported. A swallowing impairment score developed as a subjective self-analysis questionnaire demonstrated that swallowing problems occur in the first week in over half of patients undergoing thyroid surgery and may last for more than 3 months. Injury to afferent fibers innervating the pharyngeal and larynx may underlie such symptoms.27



