Physical and Psychological Preparation of Children for Anesthesia and Surgery
Jane M. Breck
Fred M. Rogers
Hedda B. Sharapan
Albert W. Biglan
When a child requires a general anesthetic for a surgical procedure, it can be a traumatic experience. This is especially true when an operation is going to be performed on such a sensitive organ as the eye. The child and his or her parents need to be prepared for ophthalmic surgery in a compassionate and supportive atmosphere. The ophthalmologist may be distracted by concerns about performing the correct procedure and/or by the technical details of the operation; however, he or she must consider the health status of the child and the child’s and parents’ emotions in order to make this experience a caring as well as a safe one.
Two decades ago ophthalmic surgery for a child was commonly performed in a hospital setting with the advantage of having the preoperative and postoperative care provided in the hospital. Ophthalmic surgery for a child is now performed in an outpatient setting either in a surgi-center or in a hospital. Because of this, procedures may be performed in surroundings that are not dedicated and equipped to take care of a child. This transition and reduction of time in a hospital places more of the burden of specialized preoperative and postoperative care for a child on the ophthalmologist and the child’s family. The needs of the child have not changed over this period, and he or she still requires the same level of support at home, both before and after the procedure. The child’s safety and emotional needs must be considered and satisfied when surgery is performed on an outpatient basis.
Preparation of the child and family for an operation begins in your office. When the ophthalmologist and the staff are sensitive and accommodating to the child, that initial contact is the first step in establishing a caring attitude and in building trust with the child.
Once it has been decided to perform an operation on a child, clear communication with the child’s pediatrician or family physician is needed to outline what procedure is going to be performed and where the procedure is to be performed. The surgeon should provide the pediatrician and the family with clear printed information regarding the policies and procedures concerning hospital admission. These instructions should also contain information that helps coordinate the efforts of both the surgeon and the pediatrician in providing help to the child and parents through this stressful time. The preparation in the surgeon’s office as well as in the pediatrician’s office should also complement care provided by the staff in the preoperative section of the hospital, the operating room, during administration of the anesthesia, and in the postoperative recovery area. Following the operation, much of the postoperative care is provided by the parent. It is, therefore, very important to give clear instructions regarding postoperative care and to provide parents with support to help the child not only physically but also emotionally through this recovery period.
Some operations are performed on relatively healthy children, whereas others are performed on children who have severe physical disabilities or extensive health problems. In some cases, emergency surgery must be performed on a patient who has never met the surgeon before. The staff must be prepared to respond to each of these situations, and procedures must be adapted to these situations.
In the first part of this chapter Breck discusses the physical preparation of children for ophthalmic surgery. Breck focuses on the detection and resolution of problems prior to hospitalization. Details of administration of an anesthetic to a child, as well as the management of medical problems before, during, and after the anesthetic are discussed elsewhere.
In the second part of this chapter, Fred Rogers and Hedda Sharapan provide insight into the psychological preparation for anesthesia as they share their many years of experience working with children and provide insight into a child’s response to a stressful situation such as an operation. Fred Rogers and his staff are people who have spent their professional lives trying to help others understand children and how certain life experiences might affect their lifelong development. As a result, they have provided some helpful guidelines and recommendations for ophthalmologists and their staff to assist children through their eye operation. Attention to the psychological as well as the physical aspects of the operation can help make the operation as caring an experience as possible.
PART 1: PHYSICAL PREPARATION FOR SURGERY
The preoperative assessment and examination by the pediatrician or family practitioner is an important prelude to a satisfactory corrective ophthalmic surgical procedure for the young patient. The younger or more medically complex the child, the more clinical information is needed to assure that the child can tolerate the procedure and the anesthesia.
The preoperative assessment should ideally cover three broad areas: (1) detection of any acute or chronic medical problems; (2) acquisition of enough medical information about the infant or child to assure that the child is in optimal health; and (3) identification of any risk factors in the medical or family history that might unexpectedly interfere with a good outcome. In this process, a pertinent medical and family history is taken, hospital and office clinical records are reviewed, a careful physical examination is performed, and the decision to obtain any laboratory studies is made.
The examination should precede and not replace consultation with the anesthesiologist. It should provide the anesthesiologist with enough information to determine the child’s baseline health status and to target any ways in which the patient deviates from the norm and may require special attention or monitoring. The pediatrician should highlight for the anesthesiologist any concerns that may compromise the safe delivery of anesthesia or influence the patient’s recovery.
In addition to providing the medical preparation, the pediatrician who has known the child and parents for a while and is a trusted friend can be very helpful in .allaying anxiety. By recognizing the normal concerns and feelings about any hospitalization or surgery, he or she can allow time for discussion of these issues during the examination before surgery. Parents should be reassured that the morbidity rate for elective ophthalmic surgery in a major medical center is very low.1 The pediatrician may also provide answers to questions in frank and simple terms, thus decreasing the fears that even a minor procedure may generate.
Same-day surgery minimizes the psychological impact of the hospitalization on the child, is convenient, and is cost effective.2 However, a discussion of the possibility of a lengthier hospital stay for the more medically-at-risk child must be introduced at this time if indicated. The hospital experience is routine for the physician but hardly a benign event for the child and the family.3 The pediatrician, the surgeon, and the anesthesiologist need to work together and communicate their findings and intentions clearly. This will result in the best outcome for their mutual patient.
THE MEDICAL HISTORY
While taking the medical history, the pediatrician uncovers information about the child’s general health and any symptoms that may require a more detailed preoperative medical evaluation. History-taking is one of the best screens for disease.4
Specific questions should be asked about any recent symptoms of illness, fever, rashes, or recent exposures to infectious diseases. Exposure to chicken pox within the last three weeks, exposure to a streptococcal throat infection within the last 3 to 5 days, and a history of family members ill at home are significant.
Cardiac and pulmonary signs and symptoms in the child are specifically sought, including cold or cough, chest pain, wheezing, asthma or allergies, history of recent or recurrent pneumonia or bronchitis, shortness of breath, pallor, duskiness, or fatigue with exertion.5 The medical history should also determine exposure to cigarette smoke in the home as well as the possibility of lead or other toxin exposure.
Information should be obtained on neurologic status, level of cognitive function, behavior, presence of seizures (type and treatment), complaints of pain, or headaches. The extent of chronic conditions of the nervous system such as mental retardation or cerebral palsy and the presence of sensory impairment such as deafness or visual deficits should be documented.
Inquire about easy bruising, bleeding from gums, bleeding in the past during minor surgery, bleeding into deep tissue or joints, or a history of aspirin ingestion.
Nutritional history includes dietary intake, special diet or restrictions, recent weight loss or excessive weight gain, and the presence of gastrointestinal symptoms.
Recent events in the child’s life that may produce stress are explored: school demands, the birth of a sibling, illness of a parent (especially the primary caregiver), divorce, separation, or a move. Attention to psychological issues helps to determine if the child is more emotionally vulnerable than usual or if the timing of the elective procedure should be changed.2
In addition to the routine questions of drug history, ask if the child is subject to motion sickness. Some references report that nearly all children subjected to motion sickness will have postoperative vomiting and recommend prophylactic treatment.1 A drug history of eye drop use is important, because phospholine iodide inhibits pseudocholinesterase and may prolong the action of succinyl choline.1
Healthy multihandicapped children frequently require ophthalmic surgery and a detailed past medical history is needed. Strabismus often occurs in patients with congenital infections, central nervous system (CNS) trauma or disease, previous craniotomy for removal of a brain tumor, history of meningitis, severe prematurity, and respiratory distress syndrome. These children require a full review of their medical history, including hospitalizations and previous surgeries, for a complete understanding of the factors contributing to the child’s well-being during anesthesia and surgery.
FAMILY HISTORY
The family history should include questions about parents’ and siblings’ health as well as the incidence of hereditary disease, congenital anomalies, allergies and asthma, blood dyscrasias or bleeding disorders, and the response of family members to general anesthesia. The pediatrician must inquire if any family member had a problem during or after anesthesia and surgery. There is an association between strabismus and blepharoptosis and malignant hyperthermia (hyperpyrexia). Although rare, it should be asked about.
THE PHYSICAL EXAMINATION
This examination should be done one week or less prior to inpatient surgery and one month or less prior to outpatient surgery.6 This evaluation should answer the question, “Is this child healthy and able to tolerate anesthesia and surgery?”
A complete physical examination begins with a general observation of the child in which body proportions, nutritional status, behavior, and interaction with parents are noted.
Vital signs in the normal range indicate a stable physical condition. A fever, temperature 101°F (38.4°C) or higher, is an indication to cancel elective surgery. Irregular pulse, abnormal blood pressure, tachypnea, or noisy respirations should alert the physician to investigate a potential problem.
Measurements of height, weight, and head size are recorded and compared to established norms to assess growth, development, and nutrition (Figs. 1 AND 2).
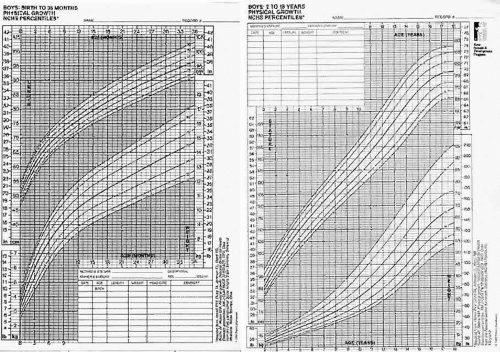 Fig. 1. A. National Center for Health Statistics physical growth chart for boys, birth to 36 months. B. Prepubescent physical growth 2 to 18 years. (Adapted from Hamill PVV, Drizd TA, Johnson CL, Reed RB et al: Physical growth: National Center for Health Statistics percentiles. Am J Clin Nutr 32:607–629, 1979. Data from the Fels Longitudinal Study, Wright State University School of Medicine, Yellow Springs. Ohio. Courtesy of Ross Laboratories) |
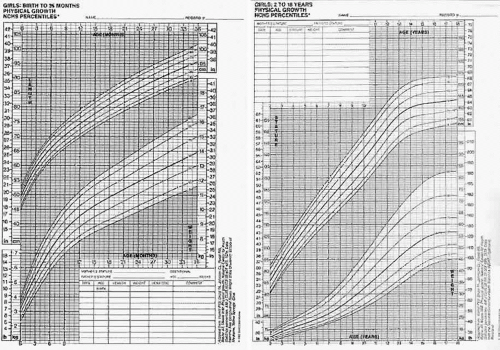 Fig. 2. A. National Center for Health Statistics physical growth chart for girls, birth to 36 months. B. Prepubescent physical growth 2 to 18 years. (Adapted from Hamill PVV, Drizd TA, Johnson CL, Reed RB et al: Physical growth: National Center for Health Statistics percentiles. Am J Clin Nutr 32:607–629, 1979. Data from the Fels Longitudinal Study, Wright State University School of Medicine, Yellow Springs, Ohio. Courtesy of Ross Laboratories) |
It is very important to inspect the head and neck structures very carefully for conditions that would make intubation difficult or contribute to upper airway obstruction after sedation or induction. Because of their small size, children’s airways can be easily compromised.7 Young infants are obligate nose breathers and a “stuffy nose” is a significant problem. Other sources for potential problems include small nares, narrow palate, posterior pharyngeal secretions, ear infections on otoscopic exam, large tongue, loose teeth, hypertrophied tonsils, small underdeveloped mandible, and any limitation of movement of the neck. Symptoms referable to ligamentous laxity with instability of the atlantoaxial joint of the cervical spine in Down syndrome patients is discussed in a section to follow. Patients who have a head tilt associated with a cyclovertical muscle palsy should not have an increased risk for an airway management problem.1
Emphasis is placed on the heart and lungs with a careful cardiopulmonary examination. If a heart murmur, tales in the chest, coughing, or wheezing are present, a more complete evaluation is warranted. Cardiovascular assessment includes examination of the skin and the nail beds and assessment of skin perfusion and temperature, especially in the limbs.7
Examination of the abdomen for presence of distention, increased organ size, or the presence of a mass should also be included. In children with cerebral palsy, a rectal examination should be performed. It is advisable to relieve constipation prior to surgery, as anesthesia could worsen this condition.
The child is observed for neurologic deficits or a developmental disorder, and the extent of the deficit is recorded. The child’s behavior is very important to observe during the physical examination. The pediatrician’s impression of the child can uncover issues that make this patient more psychologically vulnerable during surgery and hospitalization. Factors to consider include age and temperament of the child; nature and site of the procedure (eyes have a strong emotional association); predicted degree and duration of postoperative pain, discomfort, or disability; and length of time spent in the hospital for this procedure and past procedures.2
TIMING OF SURGERY
Elective surgery may be deferred or scheduled earlier depending on numerous factors: type and extent of the ophthalmic problem, age of the patient, developmental level, presence of risk factors, and need for postoperative cooperation by the patient. Early treatment may provide more appropriate developmental stimulation for the infant, remove parental anxiety, or avoid parental rejection or emotional reaction to the child’s condition.8
For premature children, it is recommended that elective operations be delayed until the postconceptual age has reached 55to 60 weeks, because anesthetics may depress the control center for breathing. For the fullterm infant, elective surgery should be delayed until forty-four weeks postconceptual age.9
The younger infant may not demonstrate the degree of traumatic psychological effects that is sometimes seen in the older child. Even with minor surgical procedures, a preschool child may show some behavioral disturbances for up to one to two months after the hospitalization. Insecurity, increased dependency, and disturbed sleep are not uncommon even with the best preparation, understanding staff, parental reassurance, or a calm, confident attitude. These behaviors may be avoided or shortened with good preoperative psychological preparation.
POSTPONING SURGERY AND ANESTHESIA
Pediatricians are often faced with the questions of whether to postpone surgery in the child with an upper respiratory infection. Early studies by Tait and Knight in 1987 suggested that complications from surgery are not increased by the presence of an uncomplicated upper respiratory infection (URI).10,11 However, children with productive cough, sneezing, hoarseness, fever, or rhonchi were excluded from these studies. Cohen and Cameron12 reviewed a large pediatric anesthesia database and compared the rates of adverse events in 1,283 children with a preoperative URI with 20,876 children without URI. The risk of respiratory complications was increased twofold to sevenfold if a child had a URI compared with children without URI. Children with a URI require more observation and management during the perioperative period, because general anesthesia in children is associated with an increased risk of adverse respiratory events.13
If the surgeon elects not to operate on a child with a mild URI, and the average child has between three and six viral URIs per year that require several weeks until full recovery of respiratory function, he or she may find that there is little time for elective surgery in the fall and winter months. The current recommendation is this: those children under the age of 5 years with an acute URI, with signs of fever, hoarseness, productive cough, fussiness, purulent discharge, or rhonchi should have their surgery postponed until they are asymptomatic. There is a need for continuous monitoring of blood oxygen saturation and the administration of supplemental oxygen in the recovery period for any child with a history of a recent URI because of the potential for residual atelectasis or reactive bronchospasm, laryngospasm, epiglottic edema, atelectasis, and pneumonia. However, the older child with isolated naso-pharyngitis with no signs of systemic or lower tract disease can probably undergo minor elective surgery without increased risk.13
LABORATORY TESTS
Preoperative assessment should not have to include routine laboratory tests in healthy children having elective outpatient ophthalmic surgery if the child is followed routinely by their pediatrician and has a normal history and physical exam.14 The value of preoperative screening tests versus their cost-effectiveness has been examined. In healthy children, results of routine laboratory screening tests have not altered decisions on whether or not to perform surgery. A hemoglobin of 10 g/dL or higher may be the only test required by some anesthesiologists to assure a minimum level required for general anesthesia.5,15 Normal hemoglobin level varies widely with age throughout infancy and childhood. In infants 8 weeks old, the lower limit of normal is 9.8 g/dL in full terms, and 7.0 g/ dL in preterms.4 Unless significant blood loss is anticipated, a hemoglobin level lower than 10 g/dL is acceptable.5 When the hemoglobin is lower than normal, the most common cause of anemia in young children is iron deficiency anemia. Iron deficiency can be treated with an oral supplement prior to an elective procedure. In older children, an evaluation must differentiate among blood loss, hemolysis, or the anemia of chronic disease. A hemoglobin and sickle cell screen should always be done for ethnic groups at risk.14 In patients in whom a white blood count determination is indicated (recent infection, lymphadenopathy and so on), the acceptable reference range is 2,400 to 16,000.9
Urinalysis is not recommended as a routine screening test.16,17 Urinalyses are costly, and the yield of important findings is small. Mitchell looked at 732 screening urinalyses in 2695 hospital admissions and found only 6 patients with urinary tract infections in the 20% of the urinalyses that were abnormal. Most of the abnormal results were not evaluated further.16 OConnor17 found 15% abnormal urinalyses in 486 children admitted for elective surgery. In only 2 cases was the abnormality important enough to cancel the operation and neither child was later found to have significant urinary tract disease.17
A chest x-ray film should not be routinely obtained in apparently healthy children. As the value of screening tests is dubious at best, what are the disadvantages? Abnormal test results from an asymptomatic patient may not indicate disease.18 Additional tests are necessary in follow-up if false positive results are obtained. The need for additional referral is not cost-effective and can cause confusion and delay of the operating room schedule. This can produce great anxiety in the patient and family.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


