Photodynamic Therapy
Brandon G. Busbee
Caroline R. Baumal
While the technique of photodynamic therapy (PDT) was recently approved for treatment of specific types of exudative maculopathy, it is not a new concept. In the 1970s, the investigational use of PDT to treat systemic malignancies in animal models was reported.1 The mechanism of PDT tumor destruction occurs as a result of vascular occlusion, stasis, and hemorrhage, as well as direct tumor cell death.2 The vaso-occlusive effect of PDT led to its investigation in animal models as a potential therapy for various types of ocular neovascularization and tumors.3,4 The ability to visualize ocular structures and to apply directed light to a targeted area using a contact lens makes the eye an ideal site for the modality of PDT.
The U.S. Food and Drug Administration (FDA) approved PDT in the year 2000 for treatment of subfoveal choroidal neovascularization (CNV) with specific features in age-related macular degeneration (AMD), and it was subsequently approved for myopia and ocular histoplasmosis syndrome. Its efficacy to treat other vascular disorders and tumors of the eye is currently being investigated.
MECHANISM OF PHOTODYNAMIC THERAPY
PDT involves two steps: the administration of a photosensitizing agent that localizes in the target tissue, followed by the application of low-intensity light to the target tissue to produce localized tissue damage. The photosensitizer may be administered by various methods, including topical, local, or systemically. For example, photosensitizers are often given topically for dermatologic disorders.5,6 In ophthalmology, these agents are typically administered intravenously to reach the retinal or choroidal circulation, although liposomal release and other experimental methods of administration have been considered. The photosensitizing agent must be delivered and preferentially concentrated in the target tissue compared to normal adjacent tissue in order to have a specific treatment effect. It has been demonstrated that certain photosensitizers have an affinity for neovascular tissue and tumor cells.7 After the drug has reached the desired tissue, low-energy light, which is supplied by a laser source and is within the absorption band of the photosensitizer, is applied directly to the area of interest. The interaction of the photosensitizer with light of a specific wavelength induces a photochemical reaction that liberates by-products that are toxic to the target tissue. Neither the drug nor the light alone (at the irradiance in the range used to PDT) appears to have any significant biological effect.8 It is the combination of these factors, utilizing light of a specific wavelength to activate the photosensitizer drug, which creates the photochemical reaction. Sequestering of the photosensitizing agent in the target tissue and direct application of low-energy, focused light by a contact lens to activate the photosensitizer within the lesion are the main features that limit induced damage to the surrounding tissue.
The mechanism of PDT action resides in the photosensitized oxidation of biological matter. When the photosensitizing agent is activated by the delivered light energy, the agent is transformed from its ground state to a higher energy singlet activated molecule. For the more efficient photosensitizers, the higher energy state decays into a lower energy, more stable molecule referred to as a triplet sensitizer. This triplet sensitizer can undergo either a Type I or Type II reaction. The Type I reaction generates superoxide anions, whereas Type II reactions result in production of singlet oxygen.9 These by-products are believed to be responsible for the localized tissue damage produced by PDT. In vivo studies after PDT show the immediate onset of vascular stasis and hemorrhage.2 These observations, along with work done on PDT for systemic tumors, provided a framework for initial studies of PDT for ocular tumors and neovascularization.8,10,11,12,13,14
CLINICAL EFFECT OF PHOTODYNAMIC THERAPY
PDT with commercially available verteporfin (Visudyne) of CNV in AMD produces choroidal hypofluorescence on fluorescein angiography within a few days following treatment.15,16,17 This corresponds to the vascular occlusion noted in animal studies.3,4 The fluorescein hypofluorescence is a result of transient, choroidal hypoperfusion, which has been demonstrated by indocyanine green (ICG) angiography.16,18 This hypoperfusion of the underlying choroidal vasculature is most pronounced within the first week after PDT. The vascular occlusive effect of PDT is not permanent, and reperfusion of the choroidal vessels typically recurs between 4 and 12 weeks after PDT.16 By 12 weeks after PDT, approximately two thirds of CNV lesions had recurred in one series.15 In another series at 12 weeks following verteporfin-PDT, the recurrence of hyperfluorescence in CNV approached the fluorescein hyperfluorescence seen before any PDT therapy in 90% of eyes.19 This recurrent leakage of CNV after PDT occurred at both the very low and high-energy light treatment doses in the early phase I and II verteporfin studies. This led to the concept of repeating PDT treatments to reinduce or maintain occlusion within CNV.
The ideal light energy dose, or fluence, to safely treat CNV was modeled on primate and early-phase studies that varied the parameters of laser irradiance, fluence, and treatment duration.8 Preliminary clinical studies demonstrated untoward effects of retinal vascular closure when a light energy dose of 150 J/cm2 was administered.20 This led to the recommendation in the phase III prospective clinical trials for PDT treatment at 50 J/cm2. Repetition of PDT treatment every 12 weeks was allowed if recurrent CNV leakage was present on fluorescein angiography and examination.21,22,23 The irradiance of 600 mW/cm2 used for PDT is markedly less than that used for thermal laser photocoagulation (which is typically in the range of 100 to 1000 W/cm2).8 Figures 1D and E demonstrate the typical CNV hypoperfusion on fluorescein angiogram noted at 4 weeks status-post PDT with verteporfin for predominantly classic CNV in AMD (Fig. 1A to C).
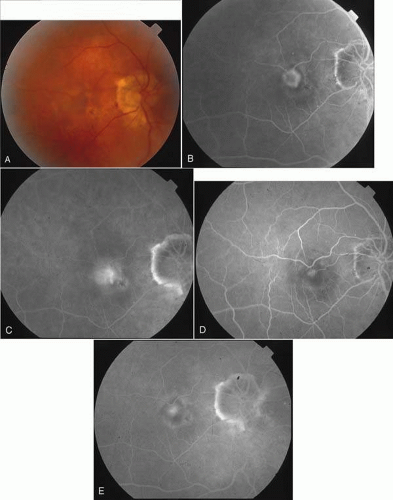 Fig. 1. A. Color fundus photograph of subfoveal CNV in a patient with AMD as well as myopia. B. Early-phase FA (35 seconds) demonstrates predominantly classic subfoveal CNV (as defined by the TAP study).23 C. Late-phase FA (3:20) demonstrates hyperfluorescent leakage from subfoveal CNV. D. Early-phase FA (42 seconds) at day 7 status post verteporfin-PDT demonstrates the typical ring of hypofluorescence corresponding to the treated area. E. Late phase FA (3:01) at day 7 status post verteporfin-PDT demonstrates a small, central area of fluorescein staining. |
PHOTOSENSITIZING AGENTS
Each photosensitizer has a specific absorption and side effect profile that affects its clinical utility for systemic and ocular PDT. The initially studied agents, known as the first-generation photosensitizers, were typically activated by shorter wavelength light and have more prolonged cutaneous photosensitivity than the newer, second-generation photosensitizers. The most common photosensitizers and their peak treatment wavelengths are outlined in Table 1 Most of the early experience using animal models in ophthalmology has been with the first-generation porphyrins, hematoporphyrin derivative (HPD) and dihematoporphyrin ether (DHE). These photosensitizers have also been studied for a variety of systemic diseases.24,25 DHE is commercially available as Photofrin (QLT Phototherapeutics, Vancouver, Canada). Another first-generation photosensitizer, 5-aminolevulinic acid (5-ALA), has been used topically to treat certain cervical and cutaneous neoplasias.5,6,25
Table 1. Photosensitizing Agents Used for Photodynamic Therapy | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Newer second-generation photosensitizing agents have been developed due to the side effect of prolonged cutaneous sun sensitivity with first-generation agents that required avoidance of sunlight for 4 to 6 weeks after PDT. These agents have been investigated in recent human studies for ophthalmic disease. The second-generation photosensitizers have a longer wavelength of absorption, which permits for deeper tissue penetration of the treatment effect. Additional advantages of the second-generation agents include more rapid clearance from the body, shorter duration of cutaneous light sensitivity, and greater affinity of these agents to concentrate in the proliferating cells of neovascular tissue.26,27
The agent benzoporphyrin derivative monoacid (BPD-MA or verteporfin) was approved by the FDA in April 2000 for the treatment of specific types of subfoveal CNV. This photosensitizing agent is commercially available under the trade name Visudyne (Novartis Ophthalmics, Duluth, GA). Verteporfin is administered intravenously and has a peak absorption of 692 nm.28 This agent appears to have preferential uptake in low-density lipoproteins (LDL) in human plasma. The photosensitizer-LDL complex is then delivered to neovascular tissue, which has an increased proportion of LDL-receptors compared with normal vascular endothelium. This effect may localize verteporfin in proliferating endothelial cells of ocular neovascular tissue. Experimental studies using fluorescein and ICG angiography have shown verteporfin reaches the choroidal and then retinal vasculature within 5 and 15 seconds, respectively. Clearance from the retina is completed by 30 minutes following injection of verteporfin. Experimental CNV collects verteporfin approximately 10 seconds after injection and the photosensitizer may remain in the complex for up to 1 hour.2
Verteporfin is primarily eliminated from the blood through hepatic metabolism within the first 24 hours.14 This rapid clearance of more than 50% of the injected photosensitizing agent significantly decreases the amount of time that patients are at risk of cutaneous light toxicity. This has been confirmed with favorable systemic side effect profiles using verteporfin in the following prospective studies: The Treatment of Age-related Macular Degeneration with Photodynamic Therapy (TAP) Study and The Verteporfin in Photodynamic Therapy (VIP) Study.23,30,31,32
Other second-generation photosensitizing agents have been investigated for treatment of exudative AMD. Tin ethyl etiopurpurin (SnET2) has been studied in animal models and human CNV as well as for ciliary body ablation.33,34 Lutetium texaphyrin (Lu-Tex) is activated by 732 nm wavelength of light. This agent has a unique property of having an emission band at 750 nm, which permits it to secondarily function as an angiographic agent to image the posterior segment circulation.35
PHOTODYNAMIC THERAPY IN AGE-RELATED MACULAR DEGENERATION
AMD is the major cause of visual loss in individuals older than 65 years in developed countries. It is subdivided into exudative (wet) and nonexudative (dry) forms. Although the exudative form accounts for approximately 10% of AMD cases, it produces more severe visual loss when compared to the dry form. Most of the new investigational therapies are directed at limiting damage from exudative AMD. The hallmark of exudative AMD is CNV, although pigment epithelial detachment and fibrovascular tissue are also features. CNV is classified by the pattern of leakage on fluorescein angiography into classic, occult or a combination of classic and occult lesions. In brief, “classic CNV” is defined as bright, early hyperfluorescence with late leakage in the TAP study, whereas “occult CNV” includes irregular or stippled hyperfluorescence on fluorescein angiography.23 This classification of CNV is important when considering the potential treatment modalities as detailed below.
Before the approval of PDT for subfoveal CNV in AMD, thermal laser photocoagulation was the only treatment with efficacy demonstrated by the multicenter Macular Photocoagulation Studies (MPS). However, laser treatment of subfoveal CNV produces immediate and permanent central visual loss due to full-thickness retinal destruction induced by thermal photocoagulation. The MPS subfoveal studies demonstrated that at 2 years after randomization, the mean vision was 20/320 in subfoveal laser treated eyes compared with 20/500 in observed cases.36 Owing to the minimal potential for visual improvement for tasks involving discriminative acuity, thermal laser was recommended primarily for patients who were agreeable to the immediate visual decline demonstrated in the MPS trial, and had a purely classic subfoveal lesion no greater than 3.5 MPS disc areas.36,38,39 Only a limited number of eyes with subfoveal CNV lesions fulfilled these criteria. Thermal laser photocoagulation is also unsatisfactory as long-term therapy for CNV in any location owing to the high recurrence rate of CNV leakage and the full-thickness neurosensory retinal destruction that it produces. Moreover, it has only been recommended to treat classic CNV. The approval of PDT in the year 2000 offers a new therapy of CNV that is potentially less destructive. It has increased the proportion of AMD patients who are candidates for a form of treatment for subfoveal CNV, and it does not appear to produce thermal neurosensory retina damage.
THE TAP STUDY
The Treatment of Age-Related Macular Degeneration with Photodynamic Therapy (TAP) Study Group was a multicenter, double-masked, placebo-controlled, randomized clinical trial. The study enrolled over 600 AMD patients with subfoveal CNV from December 1996 to October 1997, who were prospectively followed for 2 years. Patients were randomized in a treatment ratio of 2:1 to either PDT with verteporfin (verteporfin-PDT group) or placebo. Inclusion criteria included CNV secondary to AMD that extended under the geometric center of the foveal avascular zone, lesion diameter not in excess of 5400 μm, modified Early Treatment Diabetic Retinopathy Study (ETDRS)–equivalent visual acuity between 20/40 to 20/200, and fluorescein angiographic evidence that the CNV contained some classic component (Table 2). From the safety and dosing data obtained from phase I and II studies, the cumulative treatment dose of 50 Joules/cm2 was determined optimal to reduce CNV leakage on fluorescein angiography without producing retinal or choroidal tissue damage.21,22 To achieve this dose of 50 Joules/cm2, a diode laser delivered light at a wavelength of 689 nm for 83 seconds through a slit-lamp and contact lens system. This was performed 15 minutes after commencing the 10-minute intravenous infusion of verteporfin. Patients were followed at 3-month intervals, and could be retreated with either verteporfin or placebo (maintaining their initial randomization) if there was recurrent leakage present on fluorescein angiography.23 Patients were retreated with verteporfin an average of 3.4 times in the first year, and 2.2 times during the second year. Thus, verteporfin-PDT eyes received an average of over five treatments over the 2-year study period.23,40 These retreatments did not appear clinically to increase the surrounding chorioretinal atrophy in relation to the CNV area when compared to placebo-treated eyes.40
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


