Figure 5-1 Schematic representations of corneal recontouring by the excimer laser. A, Correction of myopia by flattening the central cornea. B, Correction of hyperopia by steepening the central corneal optical zone and blending the periphery. C, Correction of astigmatism by differential tissue removals 90° apart. Note that in correction of myopic astigmatism, the steeper meridian with more tissue removal corresponds to the smaller dimension of the ellipse. D, In LASIK, a flap is reflected back, the excimer laser ablation is performed on the exposed stromal bed, and the flap is then replaced. The altered corneal contour of the bed causes the same alteration in the anterior surface of the flap. (Illustrations by Jeanne Koelling.)
Surface ablation procedures were initially performed as PRK, the sculpting of the de-epithelialized corneal stroma to alter refractive power, and they underwent extensive preclinical investigation before being applied to sighted human eyes. Results of early animal studies provided evidence of relatively normal wound healing in laser-ablated corneas.
The popularity of PRK decreased in the late 1990s when LASIK began to be performed because of LASIK’s faster recovery of vision and decreased postoperative discomfort. Although more LASIK than surface ablation procedures are still performed, the number of surface ablations has increased in recent years. PRK remains an especially attractive alternative for specific indications, including irregular or thin corneas; epithelial basement membrane disease (often called map-dot-fingerprint dystrophy); previous corneal surgery, such as penetrating keratoplasty and radial keratotomy; and treatment of some LASIK flap complications, such as incomplete or buttonholed flaps. Surface ablation eliminates the potential for stromal flap–related complications and may have a decreased incidence of postoperative dry eye. Corneal haze, the major risk of PRK, decreased markedly with the use of adjunctive mitomycin C; subsequently, the use of PRK for higher levels of myopia has increased.
Majmudar PA, Forstot SL, Dennis RF, et al. Topical mitomycin-C for subepithelial fibrosis after refractive corneal surgery. Ophthalmology. 2000;107(1):89–94.
Srinivasan R. Ablation of polymers and biological tissue by ultraviolet lasers. Science. 1986; 234(4776):559–565.
Trokel SL, Srinivasan R, Braren B. Excimer laser surgery of the cornea. Am J Ophthalmol. 1983;96(6):710–715.
LASIK
The term keratomileusis comes from the Greek words for “cornea” (kerato) and “to carve” (mileusis). Laser in situ keratomileusis, which combines keratomileusis with excimer laser stromal ablation, is currently the most frequently performed keratorefractive procedure because of its safety, efficacy, quick recovery of vision, and minimal patient discomfort. LASIK combines 2 refractive technologies: excimer laser stromal ablation and creation of a stromal flap.
Wavefront-Optimized and Wavefront-Guided Ablations
Conventional excimer laser ablation treats lower-order, or spherocylindrical, aberrations such as myopia, hyperopia, and astigmatism. These lower-order aberrations constitute approximately 90% of all aberrations. Higher-order aberrations make up the remainder; such aberrations cannot be treated with spectacles. Ophthalmologists are still learning about the visual impact of higher-order aberrations in the normal population. In fact, the small amounts of higher-order aberrations found in this population may not adversely affect vision. Higher-order aberrations are also a by-product of excimer laser ablation. Some higher-order aberrations can cause symptoms—such as loss of contrast sensitivity and nighttime halos and glare—that decrease the quality of vision. The aberrations most commonly associated with these visual complaints are spherical aberration and coma. See Chapter 1 for more detailed discussion of higher-order aberrations.
In an effort to reduce preexisting aberrations and minimize the induction of new aberrations, wavefront-guided ablation creates ablation profiles that are customized for individual patients. In addition to addressing higher-order aberrations, wavefront-guided treatments can correct the lower-order aberrations of spherical error and astigmatism. Wavefront-optimized lasers have changed the ablation profile of conventional treatments by adding more prolate peripheral ablation, thereby reducing spherical aberration; however, they have no effect on other higher-order aberrations.
Compared with conventional excimer laser ablation, wavefront-guided ablations and wavefront-optimized ablations appear to offer better contrast sensitivity and induce fewer postoperative higher-order aberrations. Although advances in aberrometry and registration systems have led to improved outcomes, patients who undergo photoablation may still have more higher-order aberrations postoperatively than they did preoperatively.
Wavefront-guided ablation appears to have clear-cut benefit compared with wavefront-optimized ablation only for patients with significant preoperative higher-order aberrations; thus, wavefront-guided ablation is not suitable for all patients and may not be appropriate for use after cataract surgery, particularly with multifocal intraocular lenses. In addition, wavefront data may be impossible to obtain in highly irregular corneas or in eyes with small pupils. Patients with highly irregular corneas that cannot be treated with wavefront technology may be treated with topography-based ablations. Topography-based ablations were recently approved by the US Food and Drug Administration (FDA) and have been widely used in Canada, Europe, and other countries. In general, wavefront-guided ablations remove more tissue than conventional ablations do.
Nuijts RM, Nabar VA, Hament WJ, Eggink FA. Wavefront-guided versus standard laser in situ keratomileusis to correct low to moderate myopia. J Cataract Refract Surg. 2002;28(11): 1907–1913.
Stonecipher KG, Kezirian GM. Wavefront-optimized versus wavefront-guided LASIK for myopic astigmatism with the ALLEGRETTO WAVE: three-month results of a prospective FDA trial. J Refract Surg. 2008;24(4):S424–S430.
Patient Selection for Photoablation
The preoperative evaluation of patients considering refractive surgery is presented in detail in Chapter 2. Table 5-1 lists relative contraindications to photoablation.
Table 5-1
Special Considerations for Surface Ablation
In general, any condition that significantly delays epithelial healing is a relative contraindication to surface ablation. Although keloid scar formation was listed as a contraindication to PRK in FDA trials, 1 study found that African Americans with a history of keloid formation did well after PRK, and keloid formation is no longer considered a contraindication to surface ablation or LASIK. Historically, patients taking isotretinoin or amiodarone hydrochloride were excluded from undergoing excimer laser procedures, although there is little evidence that these drugs adversely affect laser keratorefractive outcomes.
Patients with epithelial basement membrane dystrophy (EBMD) are better candidates for surface ablation than for LASIK because surface ablation may be therapeutic, reducing epithelial irregularity and improving postoperative quality of vision while enhancing epithelial adhesion. In contrast, LASIK may cause a frank epithelial defect in eyes with EBMD, especially when performed with a mechanical microkeratome.
Any patient undergoing excimer laser photoablation should have a pachymetric and topographic evaluation (see Chapter 2). Younger patients and patients with thin corneas, low predicted residual stromal bed thickness, or irregular topography may be at increased risk for the development of ectasia with LASIK. As such, these patients may be better candidates for surface ablation. Patients with subtle topographic pattern abnormalities need to be evaluated on a case-by-case basis. In some circumstances, patients who are stable may be offered surface ablation but with a clear acknowledgment, as well as a signed informed consent form, that they understand there may still be a risk of progression to corneal ectasia.
Special Considerations for LASIK
The preoperative evaluation of patients for LASIK is similar to that for surface ablation. A narrow palpebral fissure and a prominent brow with deep-set globes both increase the difficulty of creating a successful corneal flap, and the presence of either may lead a surgeon to consider surface ablation over LASIK.
Many reports indicate that postoperative dry eye due to corneal denervation is more common with LASIK than with surface ablation. This difference is important to remember when considering refractive surgery in a patient with known dry eye syndrome. Nevertheless, many patients undergoing PRK will also experience postoperative dry eye, but it is believed that this occurs to a lesser extent than for LASIK patients.
Corneal topography must be performed to assess corneal cylinder and rule out the presence of forme fruste keratoconus, pellucid marginal degeneration, or contact lens-induced corneal warpage. Corneas steeper than 48.00 D are more likely to have thin flaps or frank buttonholes (central perforation of the flap) with procedures using mechanical microkeratomes. Corneas flatter than 40.00 D are more likely to have smaller-diameter flaps and are at increased risk for creation of a free cap due to transection of the hinge with mechanical microkeratomes. These problems may be reduced by using a smaller or larger suction ring, which changes the flap diameter; modifying the hinge length; slowing passage of the microkeratome to create a thicker flap or using a microkeratome head designed to create thicker flaps; applying higher suction levels and creating a higher intraocular pressure (IOP); or selecting a femtosecond laser to create the lamellar flap. If a patient is having both eyes treated in a single session, the surgeon must be aware that using the same blade to create the flap in the second eye typically results in a flap that is 10–20 µm thinner than the flap in the first eye. In addition, there is some concern about transferring epithelium and/or infectious agents between eyes. These specific concerns are greatly minimized with the use of a femtosecond laser for flap creation.
Preoperative pachymetric measurement of corneal thickness is mandatory because an adequate stromal bed must remain to decrease the possibility of postoperative corneal ectasia, although the definition of what constitutes an adequate residual stromal bed (RSB) remains controversial. The following formula is used to calculate the RSB:
RSB = Central Corneal Thickness – Thickness of Flap – Depth of Ablation
Although most practitioners use a minimum RSB of 250 µm as a guideline, this figure is clinically derived rather than based on any definitive laboratory investigations or controlled prospective studies. A thicker stromal bed after ablation does not guarantee that postoperative corneal ectasia will not develop. Moreover, the actual LASIK flap may be thicker than that noted on the label of the microkeratome head, making the stromal bed thinner than the calculated minimum of 250 µm. Consequently, an increasing number of surgeons are using intraoperative pachymetry—especially for high myopic corrections, enhancements, or thin corneas—to determine actual flap thickness.
Although many practitioners do not routinely measure intraoperative pachymetry and instead use an estimated flap thickness based on plate markings, the most accurate method for determining flap thickness and RSB is to measure the central corneal thickness at the beginning of the procedure, create the LASIK flap with the surgeon’s instrument of choice, lift the flap, measure the untreated stromal bed, and subtract the intended thickness of corneal ablation from the stromal bed to ascertain whether the RSB will be 250 µm or whatever safe threshold is desired. Flap thickness is then calculated by subtracting the untreated stromal bed measurement from the initial central corneal thickness. It is important to measure the corneal bed thickness quickly after making the flap in order to avoid corneal thinning from exposure to the air.
The surgeon should preoperatively inform patients with thinner corneas or higher corrections that future LASIK enhancement may not be possible because of inadequate RSB. These patients may be better candidates for surface ablation enhancements if needed.
Many ophthalmologists believe that excessive corneal flattening or steepening after LASIK may reduce vision quality and increase aberrations. Thus, many of them avoid creating overly flat or overly steep corneas, although no established guidelines are available on the specific values to avoid. The surgeon can estimate the postoperative keratometry by calculating a flattening of 0.80 D for every diopter of myopia treated and a steepening of 1.00 D for every diopter of hyperopia treated (see Chapter 2).
If wavefront-guided laser ablation is planned, wavefront error is measured preoperatively, as discussed in Chapter 1. Although wavefront data are used to program the laser, the surgeon must still compare these data to the manifest refraction before surgery to prevent data-input errors. In general, substantial differences between the manifest refraction and the wavefront refraction should alert the surgeon to a potentially poor candidate for the procedure.
Flanagan G, Binder PS. Estimating residual stromal thickness before and after laser in situ keratomileusis. J Cataract Refract Surg. 2003;29(9):1674–1683.
Kim WS, Jo JM. Corneal hydration affects ablation during laser in situ keratomileusis surgery. Cornea. 2001;20(4):394–397.
Randleman JB, Hebson CB, Larson PM. Flap thickness in eyes with ectasia after laser in situ keratomileusis. J Cataract Refract Surg. 2012;38(5):752–757. Epub 2012 Mar 16.
Randleman JB, Woodward M, Lynn MJ, Stulting RD. Risk assessment for ectasia after corneal refractive surgery. Ophthalmology. 2008;115(1):37–50. Epub 2007 Jul 12.
Salib GM, McDonald MB, Smolek M. Safety and efficacy of cyclosporine 0.05% drops versus unpreserved artificial tears in dry-eye patients having laser in situ keratomileusis. J Cataract Refract Surg. 2006;32(5):772–778.
Smith RJ, Maloney RK. Laser in situ keratomileusis in patients with autoimmune diseases. J Cataract Refract Surg. 2006;32(8):1292–1295.
Williams LB, Dave SB, Moshirfar M. Correlation of visual outcome and patient satisfaction with preoperative keratometry after hyperopic laser in situ keratomileusis. J Cataract Refract Surg. 2008;34(7):1083–1088.
Surgical Technique for Photoablation
Many of the steps in keratorefractive surgery are identical for surface ablation and LASIK. These include calibration and programming of the laser and patient preparation. The major difference between surface ablation and LASIK is preparation for ablation, which is by exposure of the Bowman layer for surface ablation and the midstroma for LASIK. A list of FDA-approved lasers for refractive surgery can be found on the FDA website (www.fda.gov/MedicalDevices/ProductsandMedicalProcedures/SurgeryandLifeSupport/LASIK/ucm168641.htm).
Calibration of the Excimer Laser
The laser should be checked at the start of each surgery day and between patients by a technician for proper homogeneous beam profile, alignment, and power output, according to the instructions of the manufacturer. Ultimately, it is the responsibility of the surgeon to ensure that the laser is functioning correctly before treating each patient.
Preoperative Planning and Laser Programming
An important part of preoperative planning is programming the laser with the appropriate refraction. Often, the patient’s manifest and cycloplegic refractions differ, or the amount and axis of astigmatism differ between the topographic evaluation and refractive examination. Thus, it may be unclear which refractive data to enter into the laser. The surgeon’s decision about whether to use the manifest or the cycloplegic refraction is based on his or her individual nomogram and technique. The manifest refraction is more accurate than the cycloplegic refraction in determining cylinder axis and amount. If the refractive cylinder is confirmed to differ from the topographic cylinder, lenticular astigmatism or posterior corneal curvature is assumed to be the cause. In this case, the laser is still programmed with the axis and amount of cylinder noted on refraction. The surgeon should take particular care to check the axis obtained on the refraction with the value programmed into the laser because entering an incorrect value is a potential source of error, particularly when converting between plus and minus cylinder formats. Before each surgery, the surgeon and the technician should review a checklist of information, confirming the patient’s name, the refraction, and the eye on which surgery is to be performed. In wavefront procedures, the treatment should correspond to the patient’s refraction, and adjustments may be required to compensate for accommodation.
For many laser models, the surgeon also must enter the size of the optical zone and indicate whether a blend of the ablation zone should be performed. The blend zone is an area of peripheral asphericity designed to reduce the possible undesirable effects of an abrupt transition from the optical zone to the untreated cornea (Fig 5-1B). A prolate blend zone reduces the risk of glare and halo after excimer laser photoablation.
Special considerations for wavefront-guided techniques
Several wavefront mapping systems and wavefront-guided lasers are available commercially in the United States and worldwide. Wavefront mapping systems are unique to the specific wavefront-guided laser used. Calibration should be performed according to the manufacturer’s specifications.
For wavefront-guided ablations, the wavefront maps are taken with the patient sitting up at an aberrometer under scotopic conditions; the mapping results are then applied to the cornea in the laser suite with the patient lying down under an operating microscope. Some systems require pupillary dilation to capture wavefront data, whereas others do not. The wavefront refraction indicated on wavefront analysis is then compared with the manifest refraction. If the difference between them exceeds 0.75 D, both the manifest refraction and the wavefront analysis may need to be repeated. The data are either electronically transferred to the laser or downloaded to a disk and then transferred to the laser. Unlike conventional or wavefront-optimized excimer laser treatment, in which the manifest or cycloplegic refraction is used to program the laser, wavefront-guided laser treatment uses programmed wavefront data to create a custom ablation pattern.
Preoperative Preparation of the Patient
Many surgeons administer topical antibiotic prophylaxis preoperatively. The patient’s skin is prepared with povidone-iodine, 5%–10%, or alcohol wipes before or after the patient enters the laser suite, and povidone-iodine solution, 5%, is sometimes applied as drops to the ocular surface and then irrigated out for further antisepsis. There is no consensus about the utility of these measures. When preparing the patient, the surgeon should take care to avoid irritation of the conjunctiva, which could lead to swelling of the conjunctiva and difficulties with suction. In addition, before laser treatment, patients should be informed about the sounds and smells they will experience during the laser treatment. They may receive an oral antianxiety medication such as diazepam.
If substantial astigmatism is being treated, some surgeons elect to mark the cornea at the horizontal or vertical axis while the patient is sitting up to ensure accurate alignment under the laser. This step is done to compensate for the cyclotorsion that commonly occurs when the patient changes from a sitting to a lying position. A 15° offset in the axis of treatment can decrease the effective cylinder change by 35% and can result in a significant axis shift.
After the patient is positioned under the laser, a sterile drape may be placed over the skin and eyelashes according to the surgeon’s preference. Before doing so, a “time-out” should be performed during which the correct patient is identified, and the treatment and eye(s) to which treatment will be performed are confirmed. Topical anesthetic drops are placed in the eye; for LASIK patients, care should be taken to ensure that the drops are not instilled too early, as doing so may loosen the epithelium substantially. An eyelid speculum is placed in the eye to be treated, and an opaque patch is placed over the fellow eye to avoid cross-fixation. A gauze pad may be taped over the temple between the eye to be treated and the ear to absorb any excess fluid. The patient is asked to fixate on the laser centration light while the surgeon reduces ambient illumination from the microscope, focuses on the cornea, and centers the laser. It is important for the plane of the eye to remain parallel to the plane of the laser, for the patient to maintain fixation, and for the surgeon to control centration even when using lasers with tracking systems. For most patients, voluntary fixation during photoablation produces more accurate centration than globe immobilization by the surgeon.
Preparation of the Bowman Layer or Stromal Bed for Excimer Ablation
The next surgical step for all excimer photoablation procedures is preparation of the cornea for ablation. With surface ablation procedures, such preparation consists of epithelial removal to expose the Bowman layer, whereas with LASIK, it involves the creation of a lamellar flap with either a mechanical microkeratome or a femtosecond laser to expose the central stroma.
Epithelial debridement techniques for surface ablation
The epithelium can be removed with (Fig 5-2)
- a sharp blade
- a blunt spatula
- a rotary corneal brush
- application of 20% absolute alcohol to the corneal surface for 20–45 seconds to loosen the epithelium
- a mechanical microkeratome with an epi-LASIK blade
- transepithelial ablation from the excimer laser itself
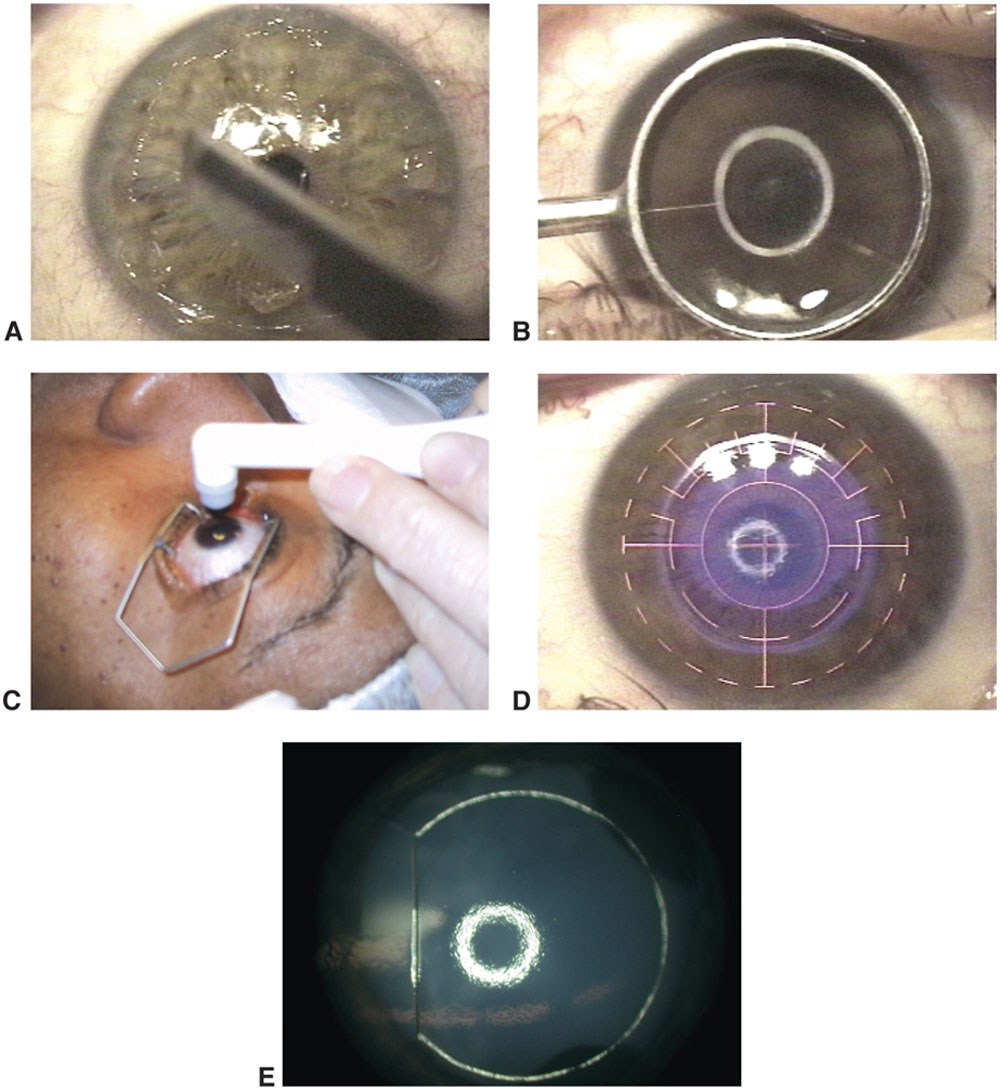
Figure 5-2 Techniques for de-epithelialization for surface ablation. A, Scraping with a blade. B, 20% dilution of absolute ethanol in an optical zone marker well. C, Rotary brush debridement. D, “Laser scrape,” in which a broad-beam laser exposes the entire treatment zone to ablation pulses; these pulses remove most of the epithelium that is fluorescing brightly, after which the basal epithelial layer is removed by scraping with a blade. E, Epi-LASIK with a mechanical microkeratome (the epithelial flap may be removed or retained). (Parts A, B, and D courtesy of Roger F. Steinert, MD; part C courtesy of Steven C. Schallhorn, MD; part E courtesy of Eric D. Donnenfeld, MD.)
In both transepithelial ablation and epi-LASIK, the peripheral margin of the de-epithelialization is defined by the laser or epi-keratome itself. For other epithelial debridement techniques, the surgeon often defines the outer limit of de-epithelialization with an optical zone marker and then debrides from the periphery toward the center. An ophthalmic surgical cellulose sponge can be brushed uniformly over the surface of the cornea to remove any residual epithelium and provide a smooth surface. The epithelium should be removed efficiently and consistently to prevent hydration changes in the stroma, because excessive corneal stromal dehydration may increase the rate of excimer laser ablation and lead to overcorrection. The laser treatment zone must be free of epithelial cells, debris, and excess fluid before ablation.
Epithelial preservation techniques
LASEK In the LASEK variant of surface ablation, the goal is to preserve the patient’s epithelium. Instead of debriding and discarding the epithelium or ablating the epithelium with the excimer laser, the surgeon loosens the epithelium with 20% alcohol for 20 seconds and folds back an intact sheet of epithelium.
Epi-LASIK In epi-LASIK, an epithelial flap is fashioned with a microkeratome fitted with a blunt epikeratome and a thin applanation plate that mechanically separates the epithelium.
Although the goal of LASEK and epi-LASIK is to reduce postoperative pain, speed the recovery of visual acuity, and decrease postoperative haze formation compared with PRK, controlled studies have had mixed results. In addition, the epithelial flap may not remain viable and may slough off, actually delaying healing and vision recovery. To date, epi-LASIK and LASEK have not proved to be superior to PRK in reducing corneal haze.
Ambrósio R Jr, Wilson S. LASIK vs LASEK vs PRK: advantages and indications. Semin Ophthalmol. 2003;18(1):2–10.
Matsumoto JC, Chu YS. Epi-LASIK update: overview of techniques and patient management. Int Ophthalmol Clin. 2006;46(3):105–115.
Flap creation for LASIK
Lamellar flap creation can be performed using either a mechanical microkeratome or a femtosecond laser. Many surgeons make asymmetric sterile ink marks in the corneal periphery, away from the intended flap hinge, just before placement of the suction ring. These marks can aid in alignment of the flap at the end of surgery and in proper orientation in the rare event of a free cap.
Microkeratome Before each surgery, the microkeratome and vacuum unit are assembled, carefully inspected, and tested to ensure proper functioning. The importance of meticulously maintaining the microkeratome and carefully following the manufacturer’s recommendations cannot be overemphasized.
The basic principles of the microkeratome and the role of the suction ring and cutting head are illustrated in Figure 5-3. The suction ring has 2 functions: to adhere to the globe, providing a stable platform for the microkeratome cutting head; and to raise the IOP to a high level, which stabilizes the cornea. The dimensions of the suction ring determine the diameter of the flap and the size of the stabilizing hinge. The thicker the vertical dimension of the suction ring and the smaller the diameter of the ring opening, the less the cornea will protrude, and hence a smaller-diameter flap will be produced. The suction ring is connected to a vacuum pump, which typically is controlled by an on–off foot pedal.



