Streptococcal Pharyngitis
The most important distinction to make in a child with acute pharyngitis is to determine whether the etiologic agent is Group A Beta-Hemolytic Streptococcus (GABHS) a.k.a
Streptococcus pyogenes. This is the only common pathogen that necessitates the use of antibiotics (
4). The overuse of antibiotics in pharyngitis from other pathogens, usually viral, should be avoided, with the exception of the rare bacterial infections. Treatment with antibiotics for GABHS will shorten the patient’s symptoms by 24 to 48 hours and reduce infectivity as well as suppurative complications, but the most important reason to give antibiotics is to prevent late sequelae (rheumatic fever and rheumatic heart disease) (
2,
3,
4,
5,
6,
7,
8). Because the symptoms of viral and bacterial pharyngitis are similar, and physicians using clinical judgment have been shown to overestimate the occurrence of GABHS, laboratory testing is required in pediatric patients (
1,
4,
5,
7).
GABHS infection is common in the 5- to 15-year-old age group, with a peak incidence during the early school years, and a decline in incidence in late adolescence and adulthood. In temperate climates, it is most common in the winter and early spring months (
4,
7). GABHS accounts for 20% to 30% of cases of pharyngitis in children, compared to 5% to 15% in adults, and is rare in patients less than 2 to 3 years (
2). According to a 2008 study, the economic burden from pediatric streptococcal pharyngitis in the United States is estimated between $224 and $539 million per year, with most of the cost attributed to parent’s time off from work (
9). In addition to GABHS, infection with other serogroups of streptococcus is possible but much less common. These include Streptococcus C and G, which have been responsible for foodborne and waterborne outbreaks of pharyngitis, but with generally less severe symptoms than GABHS (
8).
The incubation period for streptococcal pharyngitis is 1 to 4 days, after which patients will develop rapid onset of severe sore throat and odynophagia, with fevers, malaise, and possibly headache and gastrointestinal (GI) symptoms, such as abdominal pain and vomiting. In general, viral symptoms, such as cough, coryza, and nasal congestion are absent, and the presence of these symptoms makes the diagnosis of GABHS less likely. Tender, enlarged cervical lymph nodes are common. Pharyngeal examination shows erythematous oropharyngeal mucosa, including a beefy red uvula and possibly soft palate petechiae. Tonsils are also erythematous and inflamed, and may have a whitish, creamy exudate. Infants often have red, excoriated nares, with minimal rhinorrhea. Occasionally, patients will have a characteristic “scarlet fever” rash, consisting of fine, blanching, erythematous papules beginning on the trunk and spreading to the extremities, with sparing of the palms and soles (
3). This rash has a texture like sandpaper, and will last 6 to 9 days. In addition to the rash, enlarged tongue papillae with erythema (strawberry tongue) may be present, with circumoral pallor. Infants and children less than three with GABHS tend to present predominately with irritability, fevers, and abdominal symptoms, such as vomiting.
Diagnosis of GABHS depends on clinical judgment and laboratory testing, and there are several different clinical guidelines available. A scoring system has been developed and validated, which assigns points for symptoms consistent with GABHS, and may help determine the risk of GABHS in each patient (
10). All guidelines recommend against further testing if the patient does not have symptoms typical of GABHS. However, physicians have been shown to overestimate the incidence of GABHS, and overtreat with antibiotics (
10). Therefore, in patients less than 15 years of age, with typical symptoms of sore throat, fever, adenopathy, and inflamed pharynx, laboratory testing should always be performed. The gold standard laboratory test is a pharyngeal swab, with culture on a blood-agar plate, which has a sensitivity of 90% to 95% (
7,
10). Throat swabs should be taken from bilateral tonsils and the posterior oropharyngeal wall, and not the oral cavity. However, culture results typically take greater than 24 hours to obtain, and a “rapid-strep” (rapid antigen detection test, RADT) has been developed. RADT results are available in 5 to 10 minutes, which allows for immediate antibiotic treatment of a positive result. Unfortunately, traditional RADT tests only have a sensitivity of 80% to 90%, making a false-negative result more likely (
5,
6,
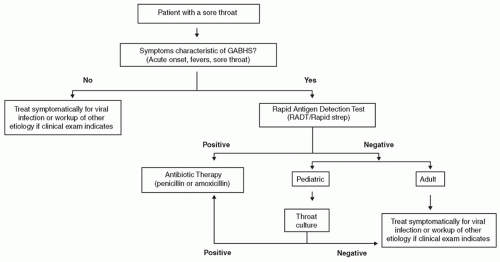
11). Newer RADT, which use optical immunoassays and chemiluminescent DNA probes, are 90% to 99% sensitive, but these are more expensive and may not be available. Therefore, a reasonable approach to the pediatric patient with sore throat is as follows: If the patient has symptoms typical of GABHS (fever, sore throat, lymphadenopathy), RADT should be performed in the office. If positive, the patient is started on antibiotic therapy immediately. If negative, a throat culture is obtained, and the patient is discharged home with a prescription for oral antibiotics. If the culture is positive, the patient is informed to fill the prescription and start therapy; if negative, they do not fill the prescription and are treated symptomatically. Practitioners should rely solely on the RADT if they have independently verified that their RADT has sensitivity greater than 90% (
Fig. 52.1).
Penicillin or amoxicillin, which is more palatable for children, is an effective treatment for GABHS. First-generation cephalosporins, azithromycin, or clindamycin may be used in patients with penicillin allergy (
1,
6). Corticosteroids have not been proven to have benefit in acute streptococcal pharyngitis (
12). Patients are not considered contagious after 24 hours of antibiotics, and should be allowed to return to school and regular activities at that time. If untreated, the GABHS pharyngitis is typically self-limited, with symptom resolution at 8 to 10 days, although throat cultures may be positive for up to 6 weeks in 50% of patients (
8). Patients are considered contagious during the acute illness and 1 week thereafter if not treated (
3). Testing or treatment of close contacts is generally not warranted, except in cases with recurrent pharyngitis between family members, or severely invasive strains of GABHS (e.g., necrotizing fasciitis). In children with recurrent strep throat and tonsillitis, tonsillectomy with or without adenoidectomy may be of benefit.
Approximately 10% of patients are considered carriers of GABHS, and will have positive strep testing without
acute illness or immune response. Treatment of carrier patients, or their family members (and pets) has not been shown to be useful and should be avoided (
13). However, antibiotic therapy may be appropriate with a personal history or close contact with someone who has had acute rheumatic fever or poststreptococcal glomerulonephritis, invasive strains of GABHS, or workers in health care facilities or nursing homes. Carrier patients can still develop pharyngitis from another serotype of GABHS or viral infection, and treatment should be started as appropriate.
Complications from streptococcal pharyngitis are rare but well described. These include rheumatic fever; rheumatic heart disease; poststreptococcal glomerulonephritis; suppurative complications such as peritonsillar, retropharyngeal, and parapharyngeal abscess; suppurative lymphadenopathy; mastoiditis; bacteremia; and sepsis. Rheumatic fever is diagnosed based on the Jones Criteria, which includes major and minor criteria such as carditis, polyarthritis, and chorea, and carries a mortality risk. Traditionally, the major role of antibiotic therapy is prevention of rheumatic fever, and rheumatic heart disease. It is estimated that 3% of patients with untreated GABHS infection will develop rheumatic fever, compared to 0.3% of patients treated with antibiotics. In the United States, rheumatic heart disease has largely been eliminated as a complication, but rates remain relatively high in undeveloped and underdeveloped countries, such as India. Antibiotics also decrease the rate of suppurative complications and associated abscess development.
Of special note is a relatively recently described but controversial entity, known as Pediatric Autoimmune Neuropsychiatric Disorders Associated with Streptococcal (PANDAS) infections. After streptococcal infection, including pharyngitis, these patients rapidly develop neuropsychiatric symptoms of obsessive-compulsive disorder (OCD) and tic disorders (
14,
15,
16,
17). The OCD and tics will last for several weeks before remitting, then abruptly return after the next streptococcal infection. In general, neuropsychiatric symptoms are from minimal to absent between episodes. It has been hypothesized that GABHS antineuronal antibodies cross-react with cells in the basal ganglia, giving rise to behavioral and motor disturbances (
16). In several case series, tonsillectomy has been of benefit, with resolution of neuropsychiatric symptoms (
17). The etiology of PANDAS is yet unknown, and its association with streptococcal infection has not been absolutely proven.
Corynebacterium Diphtheriae
Although now extremely rare,
Corynebacterium diphtheriae historically claimed the lives of millions of children and adults. Death usually occurred from cardio- or neurotoxicity from the exotoxin, or from asphyxiation from membranous pharyngitis. Vaccine introduction began in the 1920s, and there has not been a confirmed case in the United States since 2003, although diphtheria remains endemic in developing countries with low vaccination coverage (
18).
C. diphtheriae is a gram-positive filamentous rod, which is transmitted via nasal, eye, or oral secretions, or from skin lesions.
In addition to the typical symptoms of sore throat and malaise, diphtheria is characteristically associated with a gray pharyngeal/tonsillar membrane, which is produced by the local tissue response and necrosis from the bacterial exotoxin
(present in approximately one-third of patients). This can extend to cover the oropharynx and larynx, and cause rapid death by asphyxiation, particularly in the young child. The pseudomembrane is firmly attached to the mucosa, and removal characteristically leads to bleeding of the underlying site with an edematous submucosa. Patients may also have a prominent reactive cervical adenopathy leading to a “bull-neck” appearance (
1). Exotoxin-induced systemic cardiotoxicity and neurotoxicity are also possible and account for many of the adverse consequences of infection (
19).
When strongly suspected based on clinical grounds, the diagnosis is confirmed with culture of the pseudomembrane on Loeffler or tellurite medium. Treatment consists of antibiotics and antitoxin, typically with penicillin or erythromycin, and the equine hyperimmune diphtheria antitoxin. Current recommendations for immunization include combined vaccination during childhood and booster injection every 10 years in adults (
19).