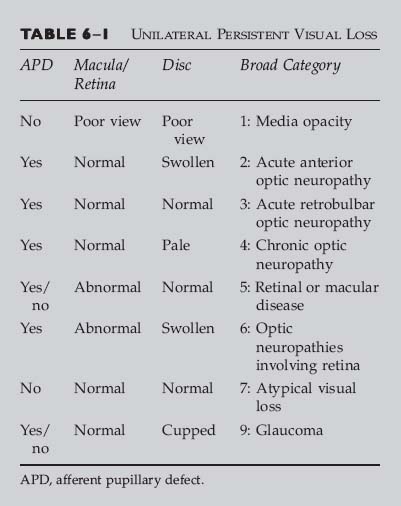
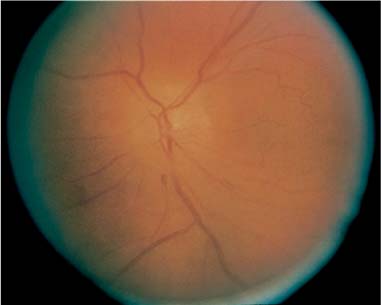
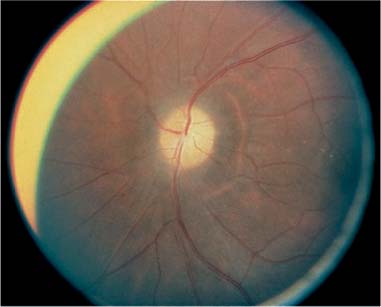
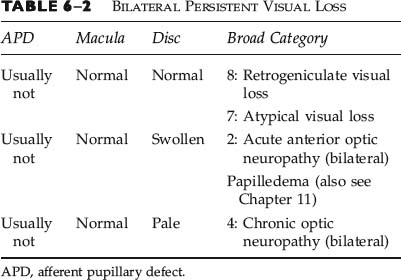
Chapter 6 This chapter can be used to diagnose the patient with persistent loss of vision. The tables in this chapter show the broad classification of persistent visual loss in one or both eyes, respectively. If vision was lost, but then regained, refer to Chapter 5. Some patients complain of “blurry vision” when they actually have diplopia. If so, refer to Chapter 9. We will assume that you have just examined the patient, but not performed a complete neuro-ophthalmic examination. First, you should use the status of the pupil and the findings on ophthalmoscopy to determine the broad category of disease (e.g., chronic optic neuropathy, glaucoma, retinal disease) that best describes the patient, using the tables below. Second, within the text corresponding to the broad category that best fits your findings, you should use other findings from the history and examination to precisely ascertain the diagnosis. The classical presentation of the disease will be described, as well as “red flags” that should alert you to the possibility that other diagnoses should be considered. Third, you will be referred to the chapter corresponding to that diagnosis, wherein guidance for further testing and management can be found. Table 6–1 is used for persistent loss of vision in one eye. If there is visual loss in both eyes, use both this table and Table 6–2 because the patient may have the same disease process affecting each eye individually or a single disease process affecting the vision of both eyes together. Table 6–2 is used for persistent loss of vision in both eyes, and outlines categories of disease that are frequently bilateral. If there is visual loss in only one eye, use Table 6–1 for unilateral persistent visual loss. It may sometimes be difficult to decide whether the patient has the same disease process affecting each eye individually, or a single disease process affecting the vision of both eyes together. In this case both tables should be consulted. If the patient is monocular, you should consult both tables. Before using this table, you should establish the following: • Pupil: Is there an afferent pupillary defect (APD)? • Ophthalmoscopy: Is the disc edematous? (Fig. 6–1) 1. A media opacity is a disturbance in the transparent refracting components of the eye. 2. In other words, the patient can’t see out, and you (the examiner) can’t see in. 3. Common reasons for media opacity are cataract, hyphema (blood in the anterior chamber of the eye), corneal scars or ulcers, and vitreous hemorrhage. 4. You can approximate the amount of visual loss from the opacity by assessing how blurred the retinal vessels appear to you when you view the fundus with a direct ophthalmoscope (but not the indirect ophthalmoscope or hand-held lenses at the slit lamp). 5. Media opacities are not discussed further in this book because they are not usually due to neuro-ophthalmic disease (an exception is vitreous hemorrhage from subarachnoid hemorrhage, i.e., Terson’s syndrome). The most expedient course of action is to arrange for the patient to be seen by an ophthalmologist. 1. An acute anterior optic neuropathy causes disc swelling and visual loss in the corresponding eye. There is an afferent pupillary defect, unless there is bilateral and symmetric visual loss. 2. Is there a history of neoplastic or rheumatologic disease? 3. Is the patient immunocompromised or on immunosuppressive medications (corticosteroids, antirejection medications)? 4. Is there pain in or around the eye, and if so, is it aggravated by eye movement? 5. Obtain visual fields for both eyes. FIGURE 6–1 Optic disc edema. Color fundus photograph depicts pale optic disc edema, segmentally worse inferiorly, with associated flame hemorrhage, in a patient with acute, painless visual loss. FIGURE 6–2 Optic atrophy. Color fundus photograph shows diffuse pallor of the optic disc in a patient with chronic, progressive visual loss. • Unilateral loss of vision over days • Pain around or behind eye, especially aggravated by movement. • Patient between the ages of 20 and 50 • Central visual loss most common, but can be altitudinal. • Difficulty with color vision • Disc edema For further information, see Chapter 20. • Unilateral loss of vision, usually over hours to a day • Little or no pain • Age greater than 50 • Altitudinal visual loss (especially inferior) most common For further information, see Chapter 19. • Rapid loss of vision in one or both eyes • Age greater than 60 • Symptoms of giant cell (temporal) arteritis: headache, scalp tenderness, pain on chewing (jaw claudication), weight loss, anorexia, proximal myalgias • Disc edema in affected eye (s) For further information, see Chapter 18. • Unilateral or bilateral visual loss over days • Pain may be present • Age usually under 50 • Afferent pupillary defect • Optic disc edema with macular star figure of retinal exudates • Central visual field loss For further information, see Chapters 20 and 21. • Acute monocular visual loss over days • Second eye involvement within 1 to 2 months • Age under 30 • Painless • Optic disc swelling, mild • Retinal arteriolar tortuosity, peripapillary retinal telangiectasia • Central, cecocentral visual field scotoma For further information, see Chapter 24. • Gradually progressive visual loss • Proptosis • May show eye movement limitation • Afferent papillary defect • Optic disc normal, edematous, or pale • May show optic disc retinochoroidal (optociliary) shunt vessels For further information, see Chapter 14. • Unilateral or bilateral visual loss occurring immediately after hypotension • Lumbar spine surgery, coronary artery bypass grafts, and massive gastrointestinal bleeding are the most common settings for this entity, but it can result from any pathologic or iatrogenic cause of shock. • Poorly reactive pupil (s), unless the visual loss is mild • Disc edema may or may not be present acutely, depending on whether the hypotension is accompanied by severe anemia. • Prognosis is usually poor. Correction of the underlying problem (anemia and/or hypotension) may occasionally be helpful. For information on nonarteritic anterior ischemic optic neuropathy, with which hypotensive optic neuropathy shares clinical features, see Chapter 19. 1. An acute retrobulbar optic neuropathy causes visual loss without any obvious change to the disc or retina. The only objective finding on examination is the presence of an afferent pupillary defect, and even this will be absent if there is bilateral symmetric visual loss. 2. Is there a history of neoplastic or rheumatologic disease? 3. Is the patient immunocompromised or on immunosuppressive medications (corticosteroids, antirejection medications)? 4. Is there pain in or around the eye, and if so, is it aggravated by eye movement? 5. Obtain visual fields for both eyes. • Unilateral loss of vision over days • Pain around or behind eye, especially aggravated by movement • Patient between the ages of 20 and 50 • Central visual loss most common, but can be altitudinal • Difficulty with color vision • Normal appearing disc, although may be pale if eye was involved in a prior attack of optic neuritis
PERSISTENT VISUAL LOSS
 Is the disc pale? (Fig. 6–2)
Is the disc pale? (Fig. 6–2)
BROAD CATEGORY 1: MEDIA OPACITY
QUESTIONS TO ASK AND POINTS TO KEEP IN MIND
BROAD CATEGORY 2: ACUTE ANTERIOR OPTIC NEUROPATHY
QUESTIONS TO ASK AND POINTS TO KEEP IN MIND
ANTERIOR OPTIC NEURITIS (PAPILLITIS)
Classic Presentation
Red Flags
 Patient greater than 50 years of age
Patient greater than 50 years of age
 Absence of any pain or discomfort
Absence of any pain or discomfort
 History of rheumatologic or neoplastic disease, or immunosuppressed state
History of rheumatologic or neoplastic disease, or immunosuppressed state
 Bilateral visual loss, including a visual field abnormality in the other eye
Bilateral visual loss, including a visual field abnormality in the other eye
 Visual loss progressive over more than 2 weeks (suggests compressive or infiltrative optic neuropathy)
Visual loss progressive over more than 2 weeks (suggests compressive or infiltrative optic neuropathy)
ARTERITIC ANTERIOR ISCHEMIC OPTIC NEUROPATHY (AAION)
Classic Presentation
Red Flags
 Patient less than age 50 (unless there is a history of diabetes)
Patient less than age 50 (unless there is a history of diabetes)
 Significant pain
Significant pain
 Bilateral disease
Bilateral disease
 Symptoms of giant cell (temporal) arteritis: headache, scalp tenderness, pain on chewing (jaw claudication), weight loss, anorexia, proximal myalgias
Symptoms of giant cell (temporal) arteritis: headache, scalp tenderness, pain on chewing (jaw claudication), weight loss, anorexia, proximal myalgias
 Absence of disc edema (disc edema is necessary for diagnosis of acute NAION)
Absence of disc edema (disc edema is necessary for diagnosis of acute NAION)
ARTERITIC ANTERIOR ISCHEMIC OPTIC NEUROPATHY (AAION)
Classic Presentation
Red Flags
 Age less than 50
Age less than 50
 Slowly progressive visual loss (suggests compressive or infiltrative optic neuropathy)
Slowly progressive visual loss (suggests compressive or infiltrative optic neuropathy)
NEURORETINITIS
Classic Presentation
Red Flags
 Significant anterior ocular inflammation
Significant anterior ocular inflammation
 Systemic hypertension (suggests hypertensive papillopathy/retinopathy)
Systemic hypertension (suggests hypertensive papillopathy/retinopathy)
 Headache (suggests papilledema)
Headache (suggests papilledema)
 Pain on eye movements or other symptoms characteristic of optic neuritis
Pain on eye movements or other symptoms characteristic of optic neuritis
LEBER’S HEREDITARY OPTIC NEUROPATHY
Classic Presentation
Red Flags
 Visual recovery over weeks
Visual recovery over weeks
 Optic disc leakage on fluorescein angiography
Optic disc leakage on fluorescein angiography
 Pain on eye movements or other symptoms characteristic of optic neuritis
Pain on eye movements or other symptoms characteristic of optic neuritis
ORBITAL CONGESTION
Classic Presentation
Red Flags
 Acute visual loss
Acute visual loss
 Pain on eye movements or other symptoms characteristic of optic neuritis
Pain on eye movements or other symptoms characteristic of optic neuritis
HYPOTENSIVE OPTIC NEUROPATHY (SHOCK OPTIC NEUROPATHY)
Classic Presentation
Red Flags
 Normal pupils
Normal pupils
 Normal discs (unless the hypotension was accompanied by anemia)
Normal discs (unless the hypotension was accompanied by anemia)
 Visual field defects respecting the vertical meridian (suggesting an occipital lobe infarct)
Visual field defects respecting the vertical meridian (suggesting an occipital lobe infarct)
BROAD CATEGORY 3: ACUTE RETROBULBAR OPTIC NEUROPATHY
QUESTIONS TO ASK AND POINTS TO KEEP IN MIND
RETROBULBAR OPTIC NEURITIS
Classic Presentation
Red Flags
 Patient greater than 50 years of age
Patient greater than 50 years of age
 Absence of any pain or discomfort
Absence of any pain or discomfort
 History of rheumatologic or neoplastic disease, or immunosuppressed state
History of rheumatologic or neoplastic disease, or immunosuppressed state
 Bilateral visual loss, including a visual field abnormality in the other eye
Bilateral visual loss, including a visual field abnormality in the other eye
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


