Chapter 57 Perceptual aspects of cerebral visual impairment and their management
Introduction
Cerebral visual impairment (CVI) is the commonest cause of visual impairment in children in developed countries.1,2 Improved perinatal care and survival of young children with profound neurological disease have increased the prevalence of cerebral causes.3 A large proportion of the brain involves visual processing, and, when affected, visual perception and cognition can be disordered. Affected young children are anosagnostic (unaware) for their perceptual deficits, which cause a range of often disabling visual behaviors.
Retrogeniculate damage to the visual brain can impair visual acuity and contrast sensitivity, and restrict visual fields,4,5 while damage to the posterior parietal and temporal lobes and their pathways gives rise to perceptual and cognitive visual impairment.
The pathology may primarily affect gray matter, white matter, or as in some cases of cerebral palsy, no anatomical abnormality is found on MRI scanning. Perceptual visual dysfunction in children is common but easily missed. It is not always accompanied by visual field deficits and poor visual acuity. Strabismus is a frequent association, and affected children may not be identified.6
Patterns of perceptual and cognitive visual dysfunction vary; many cases manifest unique features. The principal elements of perceptual visual dysfunction include impaired visual search (due to limited visual attention), often associated with inaccuracy of visual guidance of movement of the limbs. Peripheral bilateral lower visual field impairment is a common accompaniment due to posterior parietal pathology. Less commonly, impaired recognition due to disordered image processing of people, shape and objects, frequently associated with disordered orientation and route finding, may occur. The visual system alone may be affected, or associated with cerebral palsy and/or other developmental disorders. Perceptual visual dysfunction also contributes to the features of autistic spectrum disorder,7 and Williams’ syndrome.8
Synesthesia (unformed visual hallucinations while listening to music) is a benign condition, which simply warrants explanation. Normal physiological perceptions can cause concern.9 These include blurring of print, words “swimming” when reading (relaxing accommodation), seeing double (physiological diplopia), or colors (after-image effect) or spots (vitreous floaters), and things looking smaller or bigger than they should (image size flux with accommodation or cortical adaptation). The history with normal clinical examination allows the child and family to be reassured, without recourse to needless investigation.
A clinical model of the perceptual visual system
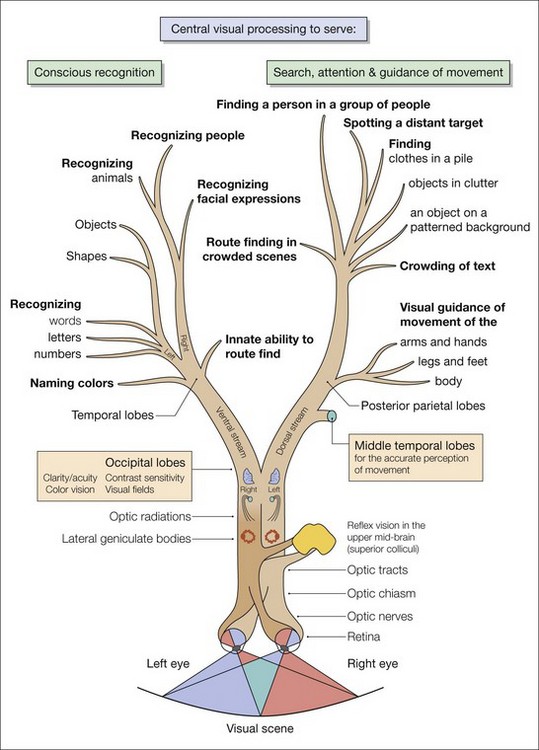
Of the many connections to centers for visual processing, the striate cortex has two principal pathways (Fig. 57.1):
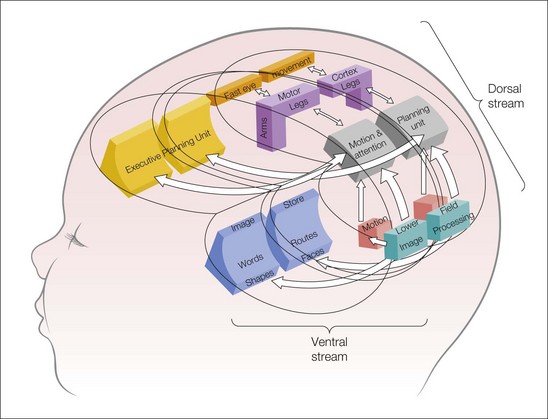
Both are responsible for discrete, separate but closely interconnected perceptual functions (Fig. 57.2).
The ventral stream and its damage
Severe focal damage to the inferotemporal cortices and ventral stream pathways impairs visual recognition and route finding, but visual guidance of movement may remain intact. This has been called “travel vision.” Such residual perception of the moving image is known as the Riddoch phenomenon,10 and the intact visual guidance of movement is served by “blindsight.”11
Diagnosis of perceptual visual dysfunction
History taking
Features of perceptual visual dysfunction
A 51 item inventory (divided into seven groups of questions) has been devised to seek dysfunction in the following areas: visual field or localized attention; perception of movement; visually guided movement of the body; visual attention; coping with crowded scenes or environments; and recognition and orientation) (Table 57.1
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


