Penetrating Face and Neck Trauma
Michael G. Stewart
Head and neck surgeons are often called upon to manage penetrating trauma to the face and neck. Knowledge of ballistics, injury patterns, and pertinent anatomy are all essential to the assessment and management of these potentially serious injuries.
The energy imparted into tissue by a penetrating projectile is determined by its kinetic energy (KE): KE = ½ MV2, where M = mass and V = velocity. Since the velocity term is squared in the equation, high-velocity projectiles can potentially impart significantly larger amounts of energy into the tissue impacted. In other words, a projectile with twice the velocity will have four times the KE of a lowervelocity projectile. However, the actual degree of wounding will also depend on the energy transfer from the projectile into the tissue (1). Typically, firearms are divided into two groups by their muzzle velocity: low velocity (less than 1,000 ft/s) and high velocity (more than 1,000 ft/s) (2). Most handguns are low-velocity weapons, with muzzle velocities between 300 and 800 ft/s. A typical shotgun has a muzzle velocity of 1,200 ft/s, and a 30-30 rifle has a muzzle velocity of 2,200 ft/s.
Gunshot wounds cause tissue injury by two main mechanisms: direct tissue injury and temporary cavitation. In the past, there was some consideration about distant injury from the transmission of shock waves; however, this theory is controversial and has been discounted by many (3). Cavitation refers to the creation of a pulsating temporary cavity surrounding the actual bullet path, as illustrated in Figure 76.1. This temporary cavity results in tissue damage and tissue loss adjacent to the missile path. This is an important concept for the treating physician to understand: anatomic structures may be significantly damaged by a gunshot wound without being actually penetrated by the projectile. Because of their high KE, high-velocity weapon injuries tend to have greater cavitation and transmission effects than low-velocity injuries. Clinically, low-velocity injuries are usually characterized by tissue damage, whereas high-velocity injuries are typically characterized by tissue loss. This can be an oversimplification; for example, a highvelocity, high-energy projectile may pass through tissue and exit with a significant amount of energy remaining. So, high velocity does not always equal high-energy transfer and tissue damage.
In addition, bullets or pellets in flight have several components to their rotation, as illustrated in Figure 76.2. These rotational characteristics increase the potential that a bullet may take an erratic course after impact, and also may increase the amount of direct tissue injury (1,3). Further, projectiles may shatter on tissue impact, resulting in secondary projectiles with the potential for additional injury. Similarly, impacted bone may also shatter, and secondary bone fragments may cause further tissue damage.
GENERAL TRAUMA PRINCIPLES
The basic principles of trauma management apply to all patients with penetrating face and neck trauma. These trauma principles may be remembered using the mnemonic “ABCDE.” “A” denotes assessment of airway and cervical spine, “B” stands for assessment of breathing, “C” refers to assessment of circulation, “D” denotes assessment of disability and neurologic status, and “E” stands for exposure and overall evaluation of the patient for other injuries. The overall prevalence of cervical spine fracture in patients with isolated facial trauma is 5% to 8% (increasing to as much as 11% when two or more fractures were present) (4), but all patients should be considered to have a cervical spine injury until proven otherwise.
In the emergency center, in addition to cervical spine x-rays, all patients with penetrating face trauma should have an AP and lateral skull and face x-ray. These films can identify remaining bullets, pellets, bullet fragments, and bony fragments, and may help define the path of the projectile. In stab wounds where the weapon is still present,
the depth of penetration may be identified. Further, these roentgenograms may reveal the presence of subcutaneous air or tracheal deviation.
the depth of penetration may be identified. Further, these roentgenograms may reveal the presence of subcutaneous air or tracheal deviation.
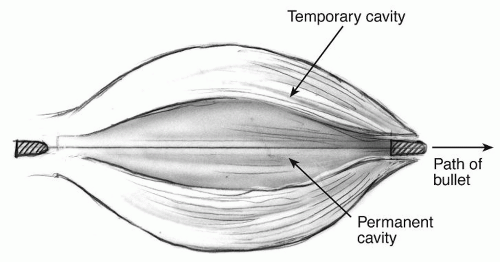 Figure 76.1 Cavitation effects of a bullet wound to soft tissue. |
Evaluation of the airway should be the first priority in the emergency center for all patients with penetrating face or neck trauma. The techniques of airway establishment are discussed in detail Chapters 63 and 64 of this textbook, but most patients can be carefully intubated transorally; if a cervical spine injury is suspected, the patient may be intubated while continuous in-line neck stabilization is applied. If the airway is unstable, and there is significant bleeding or edema in the oral cavity or pharynx, the patient should undergo cricothyroidotomy or urgent tracheotomy in the emergency center. Blind nasotracheal intubation should be avoided, although in the stable patient a fiberoptic-guided transnasal approach may be appropriate. In penetrating injuries to the neck with obvious tracheal injury (e.g., sucking wound, significant subcutaneous emphysema), the trachea may be carefully intubated through the entry wound itself using an armored/reinforced endotracheal tube.
Once the airway has been stabilized, the remainder of the examination may be completed, including a careful assessment of entry and exit wounds. When possible, information on the number of stab or gunshot wounds, the type of weapon, distance from assailant, etc., may be helpful in wound assessment. In patients with a stable airway, flexible fiberoptic laryngoscopy is a very helpful part of the evaluation, and helps assess the presence and extent of laryngopharyngeal injury. The physician should be aware that projectiles and bones may fragment or shatter, and projectiles may ricochet and change directions through the tissue—both of which may lead to secondary injuries. Probing entry and exit wounds or removing blood clots in the emergency center should be avoided, because this may precipitate significant bleeding. In addition, all patients with penetrating face or neck trauma should be considered for tetanus prophylaxis.
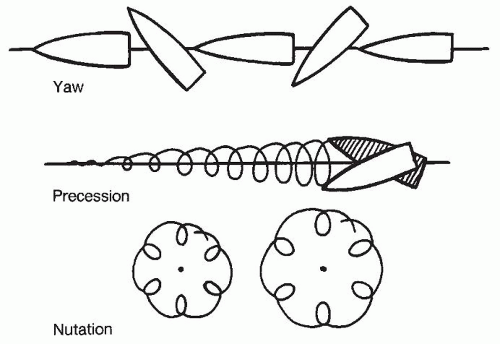 Figure 76.2 The rotational ballistics of a missile, demonstrating yaw, precession, and nutation. |
PENETRATING FACIAL INJURIES
Although much attention has been focused on treatment algorithms for patients with penetrating trauma to the neck, chest, and abdomen, there is less written about penetrating injuries to the face. The first attempt to create a staging system for penetrating facial trauma was made by Gant and Epstein in 1979 (5) and later demonstrated pictorially by Gussack and Jurkovich (6). The Gant and Epstein system divided the face into entry zones I, II, and III, which was potentially confusing since neck entry zones used the same nomenclature. Further, zone I was superior to the supraorbital rims—which actually could be considered a penetrating intracranial (rather than facial) injury. The Gant and Epstein system was modified by Dolin et al. (7) into entry zones A, B, and C, but the demarcation points between zones were unclear, and two zones (A and B) actually had similar patterns of injury. Subsequently, Chen et al. (8) attempted to simplify facial zoning by designating two entry zones, “midface” and “mandible” (Fig. 76.3).
Injury patterns to these zones are distinct, and the system is easy to remember. An algorithm for the care of patients with penetrating facial trauma is depicted in Figure 76.4.
Injury patterns to these zones are distinct, and the system is easy to remember. An algorithm for the care of patients with penetrating facial trauma is depicted in Figure 76.4.
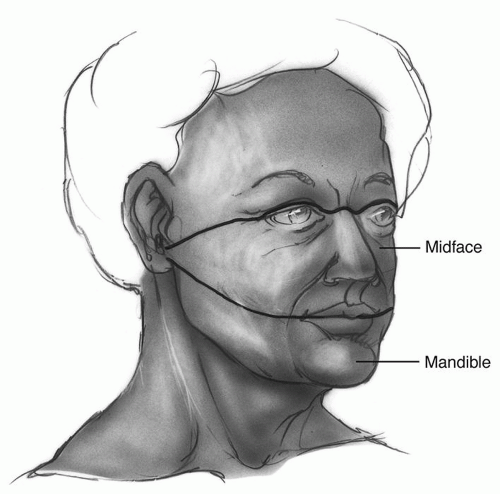 Figure 76.3 Midface and mandible zones for penetrating injuries to the face. Reprinted from Chen AY, et al. Penetrating injuries of the face. Otolaryngol Head Neck Surg 1996;115:464-470, with permission. Copyright 1996 by C.V. Mosby Year Book, Inc. |
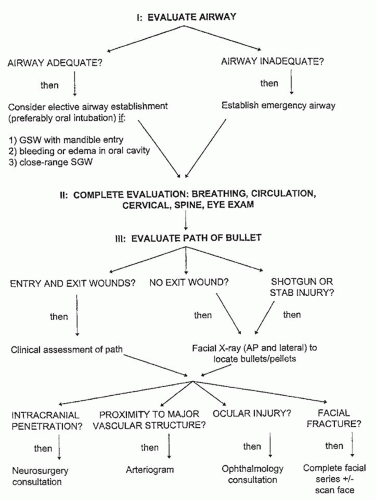 Figure 76.4 Algorithm for the initial management of patients with penetrating injuries to the face. Reprinted from Chen AY, et al. Penetrating injuries of the face. Otolaryngol Head Neck Surg 1996;115:464-470, with permission. Copyright 1996 by C.V. Mosby Year Book, Inc. |
Shotgun Injuries
It is important to remember that shotguns have fairly high muzzle velocity, and close-range shotgun injuries may impart significant KE to facial tissue. Recognizing that the distance from weapon to victim was a key point in shotgun injuries, an early classification system classified shotgun injuries into three groups: long-range injuries (type I— more than 7 yards distance between weapon and victim) were characterized by subcutaneous or deep fascia injuries only, medium-range injuries (type II—3 to 7 yards distance) were characterized by injuries to structures deep to the deep fascia, and close-range injuries (type III—under 3 yards distance) typically created massive tissue destruction. Currently, trauma surgeons usually divide shotgun wounds into only two groups: close range and long range (9). The concept is the same: close-range injuries have very high kinetic injury and behave similarly to highvelocity rifle injuries. In addition, in close-range shotgun injuries, the “wadding” material from the shotgun shell may become imbedded into the soft tissue, and must be thoroughly removed to avoid subsequent problems with infection.
In one series (8), all patients with shotgun wounds to the face invariably had pellet penetration of both midface and mandible entry zones, so the zoning system was not helpful in predicting injury pattern. Therefore, shotgun wounds should probably be considered as a separate group. This high prevalence of ocular injury has been noted in other series as well (9,10). Shotgun wounds to the face also have a relatively high prevalence of globe injury, so careful ophthalmologic assessment is important. Shotgun wounds to the face may also cause facial fracture or vascular injury, or rarely may achieve intracranial penetration.
Stab Wounds
Stab wounds to the face may result in globe injury, vascular injury, and even intracranial penetration. If the weapon is still in place, AP and lateral skull x-rays can help predict the depth of penetration and direct further evaluation. Many authors have noted that in cases where the knife or weapon is still in place, it is important to not remove or dislodge it, since it may be providing tamponade of injured vascular structures. Rather, the patient should be taken for angiography with the protruding weapon in place. If major vascular injury is identified, intravascular balloons may be placed by the interventional radiologist (or proximal vessels may be isolated by the surgeon), and the weapon may then be removed under controlled circumstances in the operating room (11).
Gunshot Wounds
The midface/mandible zoning system is particularly applicable for gunshot injuries to the face, since the two entry zones have distinct patterns of injury. Gunshot wounds to the midface have a high prevalence of vascular injury, globe injury, intracranial penetration, and facial fracture requiring open reduction and internal fixation (8,10,12).
The indications for vascular evaluation in penetrating wounds to the face can be remembered as the two “P”s:
Proximity to a major vascular structure
Penetration posterior to the mandibular angle plane (MAP).
If the path of a penetrating projectile traverses near a major vascular structure, vascular evaluation is indicated. This may be difficult to assess because the path of a projectile after tissue penetration is not always predictable, and due to cavitation, the bullet may be somewhat distant from the vessel and still cause a significant injury. A useful anatomic landmark is the MAP as described by Gussack and Jurkovich (6). The MAP is an imaginary
vertical coronal plane at the level of the angle of the mandible (Fig. 76.5) and penetration of a projectile or weapon posterior to this plane is an indication for vascular evaluation. The appropriate radiologic test depends on the situation, and this point is discussed later in the chapter.
vertical coronal plane at the level of the angle of the mandible (Fig. 76.5) and penetration of a projectile or weapon posterior to this plane is an indication for vascular evaluation. The appropriate radiologic test depends on the situation, and this point is discussed later in the chapter.
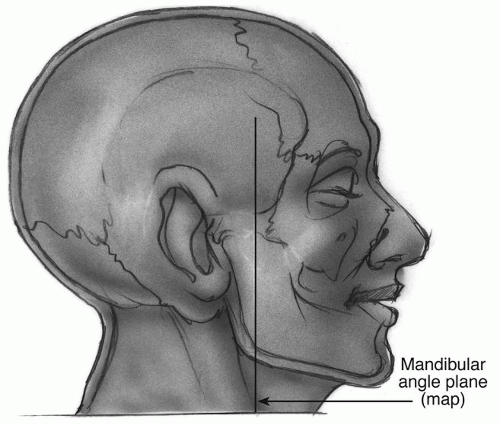 Figure 76.5 Lateral view of the face demonstrating the Mandibular Angle Plane (MAP). |
Gunshot injuries to the mandible entry zone often require emergency establishment of an airway because of bleeding, edema, or hematoma formation in the oral cavity or pharynx (8,12). Although these patients may appear initially to have a stable airway, they can quickly decompensate and require an emergency airway. Although more common with mandible entry, patients with midface gunshot wounds may also require an emergency airway (8,10,12). Therefore, a high index of suspicion and early elective airway establishment are important in patients with gunshot wounds to the face.
The computed tomography (CT) scan has significantly changed the management of penetrating facial injuries. Although airway establishment, hemodynamic stabilization, treatment of other serious injuries, and vascular evaluation should take precedence, axial and coronal CT scans of the face often significantly aid the head and neck surgeon in the assessment of damage, and improve treatment planning. In addition, CT scans clearly demonstrate the extent and severity of bony fractures.
Management of Specific Injuries
Facial Nerve Injury
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


