Pediatric Voice
Susan Baker Brehm
Melissa M. Statham
Alessandro de Alarcón
Pediatric voice disorders comprise a broad spectrum of problems commonly encountered in pediatric otolaryngology practice. Epidemiologic reports estimate that more than 1 million children in the United States are dysphonic, with abnormalities in pitch, quality, and/or loudness (1,2,3). Given the potentially far-reaching impact that voice disorders may have on the psychosocial development of children, it is imperative that practitioners have a basic understanding of this growing field and a sound working knowledge of contemporary pediatric voice evaluation and management techniques (4,5). To this end, our chapter will present an overview of key voice-related concepts and clinical issues in children.
ANATOMIC CHANGES IN THE LARYNX DURING CHILDHOOD
The Laryngeal Framework
The pediatric larynx continually matures throughout childhood. Maturational changes are particularly rapid during the first several years of life and then gradually slow down until the larynx reaches maturity in young adulthood. Both the thyroid cartilage and the cricoid cartilage undergo significant changes in length, height, width, and weight, though these changes are more pronounced in males. The pediatric larynx is much higher in the airway than the adult larynx and gradually descends with age. In a neonate, the larynx is high in the neck, with the lower border of the cricoid cartilage approximately at the level of C3-C4. By age 2, it descends to approximately C5, and by age 15, it descends to C6-C7. This downward migration is associated with increasing separation between the hyoid bone and the thyroid cartilage, which are contiguous at birth.
Microstructure of the Vocal Fold
Two aspects of the developing pediatric vocal fold play an important role in voice: (a) the relationship between the arytenoid and the musculomembranous fold and (b) the layered vocal fold structure. In neonates, the proportion of the arytenoid and the musculomembranous fold is equal. Over time, this proportion changes, with the musculomembranous fold becoming two-thirds of the vocal fold. The layered structure of the lamina propria also significantly changes. From 2 to 11 months of age, the initial monolayer gradually becomes a bilayered structure. By age 7, it becomes an adultlike three-layered structure (6,7). Collectively, these anatomic and structural changes influence when a voice disorder manifests as well as a clinician’s ability to evaluate and initiate treatment. The relationship between these changes and specific voice disorders will be discussed later in this chapter.
VOICE EVALUATION
Optimally, voice evaluation should be carried out in an interdisciplinary setting. This allows close collaboration between otolaryngologists and speech-language pathologists, thus facilitating a more thorough evaluation and the development of a comprehensive, well-coordinated management strategy. Also, it offers parents the convenience of decreasing the number of clinic visits for their child and the number of endoscopies performed.
A comprehensive voice assessment should include a medical history, an endoscopic or videostroboscopic examination, an acoustic evaluation, an aerodynamic evaluation, a perceptual evaluation, and often, a voice-related quality of life or handicapping evaluation. These combined tests provide clinicians with a global perspective on the disorder, facilitate the categorization of the disorder, and ultimately, play a role in treatment decisions.
History
A thorough medical history often allows the clinician to establish a differential diagnosis before proceeding to the endoscopic examination. This history should include relevant information pertaining to the onset of the voice disorder, the sound quality of the voice, and conditions that may alter the sound quality. Prior intubation, prior airway surgery, and prior voice therapy as well as therapeutic approaches used in this therapy should also be documented. Associated symptoms such as coughing, throat clearing, and globus sensation should be noted.
Endoscopy and Videostroboscopy
A successfully performed pediatric endoscopy depends on the child’s ability to cooperate during the examination. This is influenced by age, the presence of developmental delay, and the overall comfort level of the child (8). Successfully performing a videostroboscopy depends on whether the child is capable of sustaining a sufficiently long phonation. The choice of instrumentation must consider these two factors.
In most children, endoscopy/stroboscopy is well tolerated and easily performed. Pediatric fiberoptic endoscopes (2.2 to 2.4 mm in diameter) are typically used for children younger than age 4. Although these scopes are well tolerated, they sacrifice image quality for comfort. Pediatric chip-on-the-tip endoscopes (3.1 to 3.2 mm in diameter) provide significantly improved image quality and are generally tolerated by children age 4 and older. These endoscopes allow for the evaluation of connected speech, which plays a role in a number of pediatric voice disorders (Fig. 91.1A and B and Fig. 91.2A and B).
Rigid endoscopy is often reserved for more cooperative children, which typically includes those who are older than age 7. It can be performed using a standard adult rigid stroboscope, a smaller Hopkins rod, or a pediatric rigid stroboscope. These scopes offer better imaging of the vibrating vocal fold than fiberoptic endoscopes.
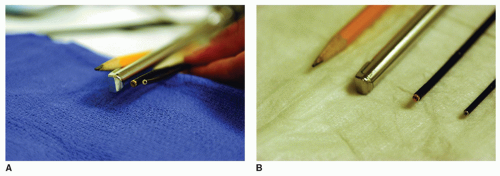 Figure 91.1 A: Endoscopes size tip view. From right to left, a no. 2 pencil, adult rigid stroboscope, 3.2 mm chip scope, 2.4 mm fiberscope. B: Endoscope size lateral view. From right to left, a no. 2 pencil, adult rigid stroboscope, 3.2 mm chip scope, 2.4 mm fiberscope. |
Videostroboscopy can be employed with either rigid or flexible endoscopes. This technique differs from standard endoscopy, as it uses a strobe light source that is synchronized with the acoustic signal produced during phonation. Furthermore, a video system is used to record the examination. The resulting images show a slow-motion glottal cycle artificially assembled from multiple glottal cycles. These images can then be reviewed to assess vocal fold vibration. Given that videostroboscopy depends on the ability of the child to cooperate, it is often difficult to obtain. Some children may be unable to provide sustained phonation of sufficient duration to allow the strobe light source to synchronize. (For a more in-depth discussion of videostroboscopy, see Chapter 65.)
Acoustic and Aerodynamic Evaluations
Acoustic and aerodynamic evaluations are best performed in a sound-treated, quiet room or a sound booth. Several software programs are available for the completion of the acoustic assessment such as the KayPENTAX computerized speech lab (Lincoln Park, New Jersey). Typical acoustic measures include maximum phonatory frequency range, fundamental frequency, loudness, perturbation (jitter and shimmer), and acoustic signal typing. These measures assist in characterizing voice problems and in helping the clinician make decisions regarding therapeutic interventions (9).
The aim of the aerodynamic assessment is to describe the relationship of the voice disorder to aspects of airflow and pressure during phonation. This assessment measures the rate of airflow through the vocal folds during phonation, breath support, and estimated subglottic pressures. Optimally, this assessment is performed by a speech-language pathologist using instrumentation available through Glottal Enterprises (Syracuse, New York) or KayPENTAX (Lincoln Park, New Jersey).
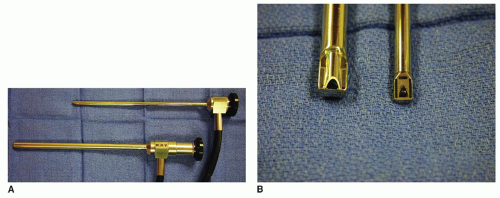 Figure 91.2 A: Rigid adult and pediatric stroboscopes lateral view. Images provided courtesy of KayPENTAX. B: Rigid adult and pediatric stroboscopes tip view. |
Perceptual Evaluation of Voice
A perceptual evaluation can best be described as a standardized expert rating of how voice is perceived. The two most frequently used perceptual tools are the GRBAS (Grade, Roughness, Breathiness, Asthenia, Strain Scale) and the CAPE-V (Consensus Auditory-Perceptual Evaluation of Voice) (10). The CAPE-V evaluation comprises six core perceptual aspects of voice, which include overall severity, roughness, breathiness, strain, pitch, and loudness. Each of these elements is rated using a visual analog system. Ideally, the rating should be performed by at least two speech-language pathologists with expertise in voice disorders.
Voice-Related Quality of Life/Handicapping
Voice-related quality-of-life/handicapping assessments are designed to measure the impact of a voice disorder on a child’s daily life. This assessment is more complicated in children than in adults because parental perspectives may be quite different from those of children. These perspectives may be colored by factors such as the child’s past airway history, the duration of the voice disorder, and societal influences.
Instruments that have been validated and are widely used include the PVOS (Pediatric Voice Outcomes Survey), the PVRQOL (Pediatric Voice-Related Quality of Life), and the pVHI (Pediatric Voice Handicap Index). A fourth instrument currently being developed is the voice-related PEDS QL 4.0 (Physical, Emotional, Social, Work/School Functioning) (11,12,13,14,15). This differs from the above-mentioned instruments in that it takes into account both the parent’s and child’s perspectives. At least one voice-related quality-of-life evaluation should be included in the battery of tests used by the practitioner in assessing a voice disorder.
PEDIATRIC VOICE DISORDERS
Laryngopharyngeal Reflux and Eosinophilic Esophagitis
The most common esophageal disorders associated with pediatric dysphonia are laryngopharyngeal reflux (LPR) and eosinophilic esophagitis (EE) (16,17). Children with these disorders generally present with chronic coughing, throat clearing, and globus sensation. These symptoms are often worse in the morning and may improve during the course of the day. The dysphonia is usually perceived as a rough, harsh-sounding voice. Voice quality fluctuates; however, it typically worsens with voice use. Although endoscopic findings are often variable, they may include vocal fold edema, erythema, vocal fold nodules, interarytenoid pachydermia, pseudo-sulculus vocalis, and thickening of the vocal fold cover (Fig. 91.3A-C).
Patients with a suspected diagnosis of LPR or EE are often initially managed with a proton pump inhibitor for a 1- to 2-month period. Parents should be advised that this medication must be taken on an empty stomach 30 minutes before a meal. Most important, it should be given at times which offer maximal convenience and consistency to both the parent and the child. Additionally, the clinician should discuss dietary changes and lifestyle modifications with patients and their families (Chapter 66).
When the dysphonia and related symptoms persist, the patient should be referred to a gastroenterologist for an esophagogastroduodenoscopy (EGD), impedance probe testing, and biopsies. These diagnostic tests will distinguish between LPR, EE, and other disorders. Optimally, otolaryngologists and gastroenterologists work collaboratively to manage these patients. For a detailed discussion of the management of patients with EE, see Chapter 59.
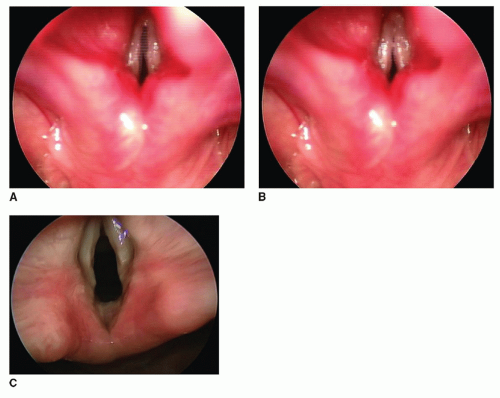 Figure 91.3 Endoscopic views of a child with refluxinduced dysphonia. (A, B) show sequential images from stroboscopy. (C) shows operative microlaryngoscopy performed during an EGD, impedance probe, and biopsies, which confirmed significant reflux. |
Vocal Fold Nodules, Cysts, and Polyps
Vocal fold nodules are the most commonly encountered cause of pediatric dysphonia (5% to 40%) (18). Patients generally present with a harsh, breathy voice. They often have limited pitch range and may have voice breaks and aphonia at specific pitches. Also, voice quality often worsens with heavy voice use. These children may be either heavy voice users or vocal abusers who frequently scream and yell. Endoscopic examination often reveals fairly symmetric bilateral lesions in the midmembranous vocal fold. During vocal fold closure, a typical hourglass closure configuration is often seen. (Fig. 91.4A and B) The location and size of the lesions variably affects mucosal wave, vocal fold vibration, and pitch. The perceptual assessment of voice quality varies from mild-to-severe dysphonia (19,20).
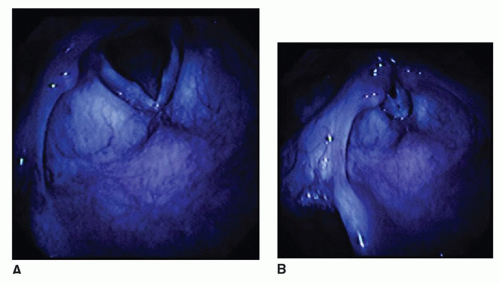 Figure 91.4 Vocal fold nodules. A: Open glottis with midmembranous nodules. B: Hourglass closure during phonation. |
The voice perception of patients with vocal fold cysts and polyps is often similar to that of patients with vocal fold nodules. In some cases, however, there may be a history of an acute phono-traumatic event associated with the development of dysphonia. Cyst and polyps are much less common than nodules. Endoscopic examination often demonstrates a large unilateral lesion and a smaller contralateral reactive lesion (Fig. 91.5A-D). As with vocal fold nodules, the size
and location of the lesion are often related to the effect on voice. Vocal fold cysts can be mucous or epithelial, and their location can vary from fairly superficial to very deep within the vocal fold. Vocal fold polyps are often exophytic, more pedunculated, and may have an obvious vascular supply. In some cases, imaging of pediatric vocal fold nodules, cysts, and polyps may not accurately differentiate these lesions. The lack of a uniformly accepted nomenclature in pediatric laryngology may also hamper diagnosis and treatment. For a more in-depth description of these benign lesions, see Chapter 68.
and location of the lesion are often related to the effect on voice. Vocal fold cysts can be mucous or epithelial, and their location can vary from fairly superficial to very deep within the vocal fold. Vocal fold polyps are often exophytic, more pedunculated, and may have an obvious vascular supply. In some cases, imaging of pediatric vocal fold nodules, cysts, and polyps may not accurately differentiate these lesions. The lack of a uniformly accepted nomenclature in pediatric laryngology may also hamper diagnosis and treatment. For a more in-depth description of these benign lesions, see Chapter 68.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


