years to accomplish a full taper in some children. Although there are certainly risks of steroid-induced cataract or glaucoma, the risk of these complications from inadequately treated uveitis is even greater. Our experience with high dose and chronic topical steroid use actually shows a reduction in such complications and better vision outcomes (15).
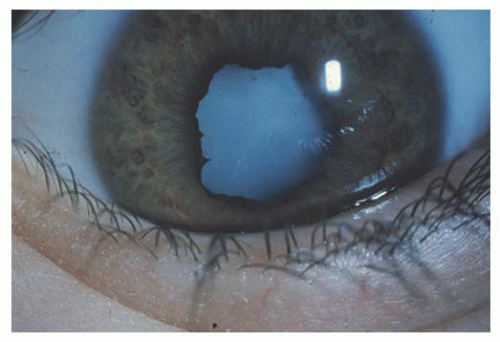 FIGURE 13.1. Child with asymptomatic oligoarticular juvenile idiopathic arthritis who did not present until visual loss was noted by which time she had a dense white cataract, multiple posterior synechiae, and active anterior uveitis. Note the absence of conjunctival inflammation. |
Table 13.1 EVALUATION AND TESTING FOR PEDIATRIC UVEITIS | |||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
and cataract were both observed at significant rates, and the authors recommend close monitoring of pediatric patients on this medication.
Table 13.2 THE SUN WORKING GROUP CLASSIFICATION OF UVEITIS (10) | |||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||
considered. Secondary glaucoma may occur more frequently in children than in adults (19,20). In general, oral corticosteroids are reserved for short course (<14 days) as an acute intervention, to test for steroid responsiveness, or perioperatively. Although nonsteroidal anti-inflammatory medications (NSAIDs) may be a useful adjunct in managing the systemic symptoms of JIA, and there has been some suggestion of ocular benefit, they play a minor role in the management of pediatric uveitis (21).
is continued for 7 to 10 days thereafter, along with a topical regimen of frequent prednisolone acetate (q1-2h) and a cycloplegic agent.
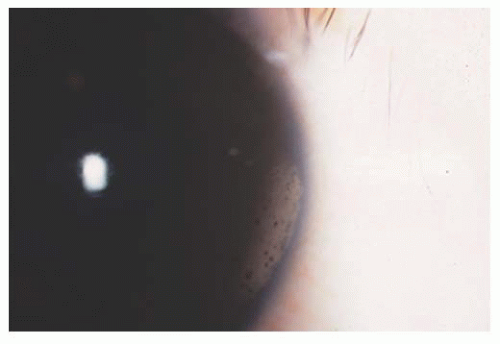 FIGURE 13.2. Typical band keratopathy of chronic pediatric anterior uveitis. Usually starts at medial and temporal limbus and then spreads over interpalpebral cornea. |
screening by ophthalmologists is advised only yearly (49,50). Acquired tenosynovitis of the superior oblique tendon (Brown syndrome) has been described (51).
TABLE 13.3 DIFFERENTIAL DIAGNOSIS OF ANTERIOR UVEITIS IN CHILDREN | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


