The goal of this chapter is to review the etiology, diagnosis, and medical and surgical management of acute and chronic pediatric sinusitis. The diseases associated with rhinosinusitis (or sinusitis) are varied and difficult to differentiate (Table 97.1). It is now recognized that prolonged purulent rhinorrhea is not the norm. Children have an immature immune system and, if they attend day care, have an increased exposure to upper respiratory tract infections and possible recurrent sinusitis. Not infrequently, parents are asked to remove their children from the day care center if purulent rhinorrhea is present. This in turn can result in absenteeism from work and lost revenue for the employee and the employer. Sinuses are present in even the youngest children and can be infected. Chronic sinusitis usually involves both the maxillary and the anterior ethmoid sinuses with almost equal frequency.
SIGNS AND SYMPTOMS
Differentiating recurrent acute and chronic sinusitis is difficult because of a lack of specificity of the signs and symptoms. In addition the symptoms are frequently suppressed with antibiotic therapy, further confusing the diagnosis. Upper respiratory tract infections are frequently confused with sinusitis, and the primary delineation between the two appears to be the chronicity of the infection. Wald (1) noted that symptoms of the common cold improve in 5 to 7 days, and if the symptoms persist longer than 10 days, the symptoms are likely to be secondary to either an acute sinusitis or to persistent symptoms of chronic sinusitis. Acute sinusitis will take as long as 3 weeks to resolve symptoms. Historical documentation becomes confusing when antibiotics are prescribed as they suppress symptoms. Dr. Wald called the two types of sinusitis: persistent and severe, which occur secondary to an upper respiratory tract infection, and more severe infections, which are associated with a temperature of above 103°F rectally and thick, purulent nasal discharge. She argues that most nonsevere sinus infections resolve spontaneously, whereas more severe sinusitis requires treatment with antibiotics (1). Signs and symptoms and their severity may vary with the patient’s age (Table 97.2). The young patient often has nasal congestion and anterior purulent rhinorrhea. The older patient may not be as symptomatic but complains of nasal congestion, postnasal drip, or sore throat secondary to the chronic drainage. Cough is a frequent complaint and is usually more severe at night. Daytime cough is more significant, however, as it is more likely to be associated with sinusitis. The relation between cough and chronic sinusitis is not clear. The symptom of chronic cough is most dramatic in the asthmatic patient, whose asthma attacks are frequently exacerbated by acute infections. Fever is much more common in the younger patient and is a frequent complaint, although rarely documented in the office.
Pain may manifest itself in a variety of ways. Younger children are irritable and may manifest head banging. The older patient complains of headaches and may be able to localize the area of pain. Unrelenting pain isolated over the vertex or back of the head without other symptoms may be associated with sphenoid sinusitis and needs to be ruled out with a CT scan (2,3). A significant problem with symptom assessment in chronic sinusitis is inadequate documentation. Two good validated instruments, SN5 (4) and S5 (5), are available but not frequently used.
PHYSICAL EXAMINATION
Signs of sinus infections include nasal congestion with dilatation of the mucosa, giving it a bluish appearance. Nasal discharge is often present with a variety of viscosities and may be clear, yellowish, or greenish; the clear drainage is generally thought to be associated with allergies, whereas yellow or greenish drainage is thought to be associated with a viral or bacterial infection. Another common but nonspecific sign is dark inferior eyelids with puffiness over the maxilla. The physical examination of the child is difficult primarily because of poor compliance (Table 97.3). The approach to the child must be slow and nonthreatening. Head movements from side to side and the narrowing of the nasal vestibule brought on by crying make the examination virtually impossible. If the child refuses examination, little can be gained by trying to force the examination. The tools used to examine the nasal vault may include a nasal speculum and head mirror, microscope and nasal speculum, otoscope, flexible nasal pharyngoscope, or rigid telescope. The Viroscope, by Welch Allyn, offers a unique method of performing anterior nasal examinations. The light headlight is quite bright, and the anterior nasal airway can be viewed through lenses that narrow the parallax of the observer. This allows good visualization of the anterior nasal airway and middle meatus. Regardless of the method used, anterior rhinoscopy is all that can be accomplished, except for nasal pharyngoscopy, which can be performed with the flexible nasopharyngoscope. The flexible scope is most advantageous in the older postoperative patient.
TABLE 97.1 DIFFERENTIAL DIAGNOSIS OF DISEASES COMPATIBLE WITH PEDIATRIC CHRONIC SINUSITIS
Chronic sinusitis
Adenoid hypertrophy
Recurrent upper respiratory (viral) infections
Allergies
Immune deficiencies
Ciliary dyskinesia
It is best to examine the ears first with an otoscope. If the child tolerates otoscopy, the physician has gained the child’s confidence, and anterior rhinoscopy can then be attempted with the otoscope. If all goes well, then vasoconstriction can be best accomplished with 0.05% oxymetazoline. A mixture of 1:1 0.05% oxymetazoline and 4% lidocaine will effectively anesthetize and vasoconstrict the nose for nasopharyngoscopy. After several minutes, the nose is reexamined to evaluate for possible purulence that has flowed into the anterior nasal vault. In children, polyps usually signal cystic fibrosis or allergic fungal sinusitis. It is encouraging if the middle meatus is clear and without edema, but this does not assure a disease-free sinus. Examination with a rigid telescope can be performed in the unusually cooperative child with local anesthesia. Rolling a 2.7-mm telescope into the middle meatus, as is frequently recommended in adults, is virtually impossible in children.
TABLE 97.2 SIGNS AND SYMPTOMS OF CHRONIC SINUSITIS
Purulent nasal discharge
Day and night cough
Nasal airway obstruction
Headache, irritability, or facial pain
Fever
Postnasal drip
TABLE 97.3DIAGNOSIS PHYSICAL EXAMINATION IN CHRONIC SINUSITIS
1.
Only anterior rhinoscopy can be performed in most children.
2.
Visualize the septum then middle turbinate and then the middle meatus laterally.
3.
A clear middle meatus does not ensure that no sinus disease is present.
4.
Look for purulent discharge at the middle meatus.
5.
Polyps are unusual in children. Think of cystic fibrosis, fungal sinusitis, and NARES syndrome.
The physical examination, therefore, gives clues to the diagnosis of possible sinusitis but is not diagnostic.
OTHER DIAGNOSTIC AIDS
Table 97.4 lists other diagnostic modalities useful in the evaluation. Transillumination in children is useless as the sinuses are quite small, do not transilluminate, and offer no diagnostic advantages. Ultrasound can be used only in the maxillary sinus and has been found to be inconsistent with plain radiography. Plain films have been found to be inaccurate when compared to computed tomography (CT) scans (Fig. 97.1). McAlister et al. (6) at St. Louis Children’s Hospital prospectively studied 70 children with symptoms of chronic sinusitis and compared the plain films with the coronal CT scans. They found a discrepancy between CT scans and plain films of 29% to 23% and concluded that the plain films both over- and underestimate the amount of sinus disease noted on CT scans. Similar findings have been reported by Lazar et al. (7) and Goldstein and Phillips (8). CT scan has become the gold standard for the evaluation of chronic sinusitis in children. There is increasing concern that children are receiving significant doses of radiation from CT scans. Brenner et al. (9) raised the concern that radiation in infants increased the risk of cancer later in life. This was highly controversial; however, Rogers (10) noted that children were getting doses similar to adults and the smaller heads were associated with greater doses of radiation (11). This is particularly important when it is understood that 25% to 30% of a child’s bone marrow is located in the skull. Pediatric radiologists are acutely aware of this issue and now practice ALARA or “as low as reasonably achievable” to obtain the desired results.
TABLE 97.4 OTHER DIAGNOSTIC AIDS FOR PEDIATRIC CHRONIC SINUSITIS
Transillumination: No help in children
Ultrasound: Not a viable option
Plain films: Inaccurate assessment of ethmoid sinuses
CT scan: Most accurate assessment of the sinuses
MRI applicable for acute disease extending beyond sinuses; into the orbit and brain
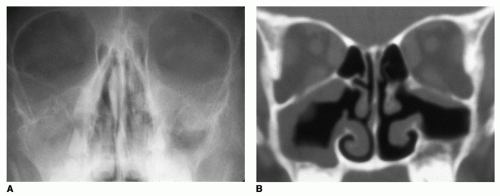
Figure 97.1 A: Plain radiograph of a child who has had endoscopic sinus surgery. Notice the opacification of the right maxillary sinus and significant mucous membrane thickening of the left maxillary sinus. The ethmoid sinuses are difficult to assess on this film. B: Computed tomography scan of the same patient, taken about 20 minutes later. No disease is seen in the ethmoid cells, and true mucous membrane thickening of the right maxillary sinus was represented as opacification on the plain films. The right maxillary sinus is clear, except for thickening along the roof of the sinus. Note that the maxillary antrostomies are widely patent.
ETIOLOGY
Our understanding of the etiology of chronic sinusitis continues to evolve. A principle that is now a cornerstone in our understanding of chronic sinusitis is that initially an inflammatory obstruction occurs in the natural ostium of the sinuses. The cause of the inflammation may be multifactorial but is usually secondary to a viral or bacterial infection. An area that appears particularly prone to obstruction is the ostiomeatal complex. This narrow channel, the infundibulum, drains the frontal, anterior ethmoid, and maxillary sinuses. The infundibulum is bordered by the uncinate process anteriorly and arches posteriorly where it is bordered by the ethmoid bulla. The frontal sinuses drain most frequently into the superior portion, and the maxillary sinuses drain into the posterior half of the infundibulum. Edema from any cause can narrow the infundibulum or the ostium and cause obstruction, which could result in a secondary infection. The viruses most frequently encountered are in patients with acute sinusitis: rhinovirus, parainfluenza, influenza, and adenovirus. The obstruction may be secondary to anatomic abnormalities or inflammation secondary to upper respiratory tract infections, allergies, or barotrauma. It was thought for many years that an anatomic variation of the anatomy around the ostiomeatal complex is associated with a higher incidence of chronic sinusitis. Children with septal deviations, paradoxical turbinates, and infraorbital cells do not have a higher incidence of chronic sinusitis (12,13,14).
We know that normal ciliary function is necessary for healthy sinuses; we also know that chronic sinusitis is associated with abnormal cilia. The cilia beat more slowly and less efficiently in patients with mucosal infections. When two ciliated surfaces come together, a localized disruption of the ciliary clearance and a secondary pooling of secretions occur. In the area of the ostium, the secretions may become secondarily infected and cause an acute or chronic sinusitis. Ciliary function is important because the ostia are often small and located in positions that are not conducive to spontaneous drainage. The best example of this is the maxillary sinus, where the ostium is located at the superior medial border. Kartagener syndrome is an example of significant ciliary dysfunction, and virtually all of these patients have evidence of chronic sinusitis. Some investigators believe that gastroesophageal reflux disease (GERD) plays a vital role in the etiology of chronic sinusitis. Barbero (15) noted that the parallel existence of upper airway inflammation, intractable sinusitis, and gastroesophageal reflux suggests a causal relation. Another possible explanation is GERD causes interruption of the normal mucosa over the adenoid pad allowing the formation of biofilms deep within the crypts of adenoid tissue. This in turn could be associated with a nidus for seeding of the nose with pathologic bacteria. It is likely that a relation exists between GERD and sinusitis in some patients, but the overall frequency is not understood. The presumed etiology for this association is once again inflammation followed by ostial obstruction and subsequent infection. Gastric secretions are very caustic to nasal mucosa, and only occasional, once every few days, regurgitation may be enough to result in a diseased state. Infrequent exposure will not be noted with our current methods of diagnosis.
Most episodes of sinusitis occur during the winter when viral upper respiratory tract infections are at their greatest. This lack of correlation with the incidence of peak allergy calls into question the overall role of allergies in sinusitis. In some patients, seasonal allergy plays a role. Environmental and food allergies, which are not seasonal, may also play a significant role in some patients. A variety of immune deficiencies and ciliary dysfunction also may be associated with chronic sinusitis.
BACTERIOLOGY
Despite the importance of sinusitis, relatively few studies investigated the microbiology of chronic sinusitis in children. This is probably because of the inaccessibility of the sinuses except the maxillary, which is accessible through a puncture but requires a general anesthetic in younger patients.
The literature focusing on chronic versus acute sinusitis is inadequate, but some useful information can be ascertained from studies performed on acute sinusitis. Investigations of acute sinusitis found that Streptococcus pneumoniae was the most common organism (30%), followed closely by Moraxella catarrhalis and Haemophilus influenzae (20%). H. influenzae is usually nontypeable. Both M. catarrhalis and H. influenzae have a high incidence of β-lactamase-producing enzymes and are therefore resistant to many antibiotics. Anaerobes were infrequently found (only one in 79 sinus aspirates), and Staphylococcus also was rare. One-fourth of patients with bilateral maxillary sinusitis had discordant bacterial cultures. Because the cultures were taken about 10 days after the onset of symptoms, viruses were not often found. The bacteria involved with subacute infections (i.e., infections lasting between 10 and 21 days) are similar to those of acute sinusitis, with S. pneumoniae, M. catarrhalis, and H. influenzae being the most common (Table 97.5).
The bacteria of chronic sinusitis are similar, with notable exceptions. Brooks et al. (16) found a high incidence (˜50%) of anaerobic bacteria in the culture of maxillary sinus contents. Most of the anaerobes were anaerobic cocci and Bacteroides sp. Nord (17) also cultured only the maxillary sinus and found a high incidence of anaerobic bacteria. The use of broad-spectrum antibiotics has resulted in an increase in the incidence of resistant bacteria of the upper respiratory tract. There is evidence that H. influenzae is now much more resistant to ampicillin in pediatric rhinosinusitis (18). There is also an increase in the incidence of S. pneumoniae serotype 19A, which has an unusually high resistance rate (19). There are also multiple studies reporting an increased incidence of MRSA-positive cultures (20,21,22). PCV7 vaccinations have resulted in vaccine-specific serotype eradication of bacteria, but there has been a shift to other resistant H. influenzae-resistant strains (23).
TABLE 97.5 MOST COMMON BACTERIA OF CHRONIC PEDIATRIC SINUSITIS
Aerobic Bacteria
Streptococcus pneumoniae
Moraxella catarrhalis
Haemophilus influenzae
Staphylococcus aureus, increasing incidence of MRSA
α-Hemolytic streptococci
Pseudomonas aeruginosa
Anaerobic bacteria
Peptococci
Peptostreptococci
Bacteroides
MEDICAL MANAGEMENT
Mechanical cleaning of the nasal airway with saline irrigation is increasingly recognized as a valuable factor in treatment of chronic sinusitis (24,25). The problem is patient compliance in the pediatric age group. Kassel et al. (26) reported, in a metaanalysis report, a 40% incidence of noncompliance. Studies however have failed to show that it helps with acute sinusitis (27). There is a general consensus that buffered normal saline is better for ciliary function and therefore is preferable to hypertonic solutions. Treatment for other possible causes of sinusitis, including allergies and immune deficiencies, should also be instituted before endoscopic sinus surgery. In a recent questionnaire of pediatric otolaryngologists (28
Only gold members can continue reading. Log In or Register to continue
 DIAGNOSIS PHYSICAL EXAMINATION IN CHRONIC SINUSITIS
DIAGNOSIS PHYSICAL EXAMINATION IN CHRONIC SINUSITIS