Pediatric Ocular Trauma
Gary L. Rogers
Don L. Bremer
Mary Lou Mcgregor
PRINCIPLES OF EMERGENCY OCULAR TRAUMA
Ocular trauma frequent causes emergency department visits at pediatric hospitals. The extent of trauma may range from simple superficial injuries to devastating penetrating injuries of the eyelids, lacrimal system, and globe. Regardless of the severity, it is often difficult to examine a child because of his or her discomfort, inability to understand, and inability to communicate. These problems all result in the label “poor cooperation.” Suspicion of the level of the injury is raised after taking a detailed history of the events surrounding the injury. A full medical and ocular history should be taken. A complete and accurate assessment of the injury must be made with confidence. If this is not possible in the emergency department, the child must be sedated or taken to the operating room for an examination under anesthesia. Never neglect the uninjured eye. Findings of the “normal” eye may have an impact on management of the injured eye.
INCIDENT HISTORY
First, a complete account of the accident should be obtained. In some situations parents or baby-sitters have not witnessed the accident and may be unable to give an exact accounting. The child should be questioned and may be able to provide valuable information regarding the accident. Isolating the child from the parents may reveal a more accurate history of the events. From the history, the nature and extent of the injury can be determined, which aids in how extensive an evaluation is needed. Knowing the type of trauma may alert one to look for secondary ocular effects, such as fat emboli from a crush injury. Injuries caused by large blunt objects may produce contusions to the periorbital region and would favor contrecoup retinal problems and blowout fractures of the orbit along with rim fractures. Missiles or sharp objects would raise the suspicion of a perforated globe or retained foreign bodies in soft tissues or the orbit.
Because of the potential for general anesthesia, pertinent past surgical history of the patient and drug allergies are important to obtain along with current immunizations. Although the incidence of tetanus is rare, in the United States booster doses of tetanus toxoid should be received every 5 years to maintain adequate immunity and should be administered in “dirty” cases.1 A dose of 0.5 ml of tetanus toxoid is appropriate for immunized children. If the child has not been immunized, the tetanus immunization series should be initiated with a 0.5-ml dose of diphtheria-pertussis-tetanus vaccine.
MEDICAL HISTORY
Even in the pediatric age group, a complete medical history is necessary. Although the incidence of transmissible disease is low, the potential exists and one should not hesitate to obtain permission for testing for human immunodeficiency virus and hepatitis. Medical conditions should be considered with particular attention to hematologic and bleeding disorders. Knowing the sickle cell status in black patients is important before general anesthesia is administered.
EXAMINATION
Examination should be as extensive as the injury permits. If there are other injuries that must be addressed, the examination and treatment may be modified as determined by the severity and extent of those injuries. Recording visual acuity should be attempted on all patients with ocular and periocular trauma. Various methods of evaluating the vision include Snellen letters, random Es, Allen pictures, finger counting, and light perception with or without projection. One must consider the child’s age and the severity of the injury when determining the appropriate visual acuity test. The severity of ocular injury can be assessed by its affect on vision. Initial visual acuity is known to be a prognostic indicator of final outcome.
External
The external examination should consist of looking for puncture wounds of the lids and brow, which could be through and through lacerations or punctures that could involve the globe. If there is ever any question of an open globe, a shield should be placed on the eye until the child is placed under general anesthesia for thorough evaluation and possible repair. Lacerations of the eyelid margin must be attended to with particular attention to the nasolacrimal system and its integrity. Palpation of the orbital rim helps to rule out fractures with possible displacement.
Ocular motility, ductions, and versions must be evaluated because of the possibility of muscle entrapment, laceration, or possible paralysis.
When there has been ocular trauma, one should always ask about diplopia. A small child often does not understand the meaning of double vision, and the clinician needs to explain this problem in very simple terms.
Interior Examination
ANTERIOR SEGMENT. A slit-lamp or penlight examination should assess the clarity of the cornea, the anterior chamber depth, distortion of the pupil, and the presence of a hyphema (Fig. 1).
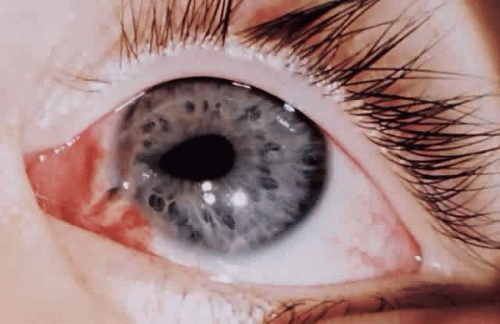 Fig. 1. A 3-year-old child with a “peaked” pupil indicating a full-thickness corneal laceration requiring surgical intervention. |
PUPILS. The size and shape of the pupil can aid in evaluation of an open globe. The reaction of the pupil, depth of the anterior chamber, consensual pupillary response, and afferent defect are critical in the initial evaluation.
RETINA. If possible, the retina must be evaluated for tears, hemorrhage, perforation, and retained foreign bodies. No retinal examination or manipulation of the globe should be attempted if there is a concern about a lacerated globe. The nature of the injury would also direct the need for appropriate diagnostic tests: roentgenography, computed tomography (CT), or ultrasonography.
If the retina is unable to be visualized and there is no obvious penetrating injury to the globe, B-scan ultrasonography can help in assessing the status of the retina. This plays a role in patients with hyphemas and vitreous hemorrhages. If a retained foreign body is suggested, plain films or CTs are helpful in localizing metallic foreign bodies. Magnetic resonance imaging is preferred when localizing glass but should never be ordered if one suspects a metallic foreign body.
PLAN OF ACTION
After all information has been gathered, a definitive plan of action can be considered. If surgery is needed for a rupture, repair must be made as soon as possible. Correction of external problems involving the eyelids and lacrimal system can be delayed for 24 to 48 hours without increased risk of infection.
After a thorough history and examination have been performed, it is important to document all this information to help in the management of the patient and also be available if any legal action regarding the injury is taken.
REPAIR OF LACERATED GLOBE
A perforated globe is a true ophthalmic emergency. Missile injuries from children playing with BB guns or sharp projectiles are the most common cause for lacerated globes. Any eye suspected of being lacerated should be treated as such until it can be proven that the globe is intact.
HISTORY
A detailed history of the trauma may indicate the nature and extent of the injury. The initial questioning should be directed toward the child, with the parents present to corroborate the story. Children may not readily volunteer the exact cause of the accident for fear of parental reprisal. In this case, it is helpful to repeat the questions to the child in a nonthreatening manner away from the parents. This gives the child an opportunity to provide more accurate details about the accident. The history should always probe for the possibility of an intraocular foreign body with the appropriate ancillary test of roentgenography, CT, or ultrasonography. Plain films are of little value except as a screening device. It is important to note whether eyeglasses or contacts were worn at the time of the injury.
It is especially important to know the visual status of both eyes before the injury and whether there is a history of amblyopia or previous ocular surgery. Any medications the child is taking or any hematologic or clotting problems should also be ascertained.2
EXAMINATION
In our experience, most ruptured globes in children that involve sclera are evident because of severe chemosis and poor vision. These ruptures are often associated with a protruding iris and flat anterior chamber. There may be difficulty in diagnosing a small corneal perforation, which can be self-sealing. As in any ocular injury, the best corrected vision should be determined either with lenses or pin hole testing. Noting whether the pupil is round, eccentric, miotic, or mydriatic or has an altered reaction to light may lead to the realization of a ruptured globe, even if the puncture wound is small.
Motility examination, manipulation of the lids, and intraocular pressure measurements should be avoided in a patient suspected of having a perforation. Shields should be immediately placed on the eye to minimize the possibility of extruding intraocular contents.
Slit-lamp examination can help determine the status of lacerations and hemorrhages of the conjunctiva, corneal defects, foreign bodies, and depth of the anterior chamber. The Seidel test for evaluation of a corneal wound leak is important in determining whether the wound has sealed itself or whether aqueous is being emitted.
Posterior segment examination should be avoided in cases of ruptured globes to prevent possible extrusion of intraocular contents. However, it may be necessary to look for choroidal and retinal ruptures or vitreous foreign bodies.3
PREOPERATIVE PLAN
Depending on the age and cooperation level of the child, the examiner selects the approach needed to correct the problem. Partial thickness lacerations or small self-sealing corneal lacerations may be managed conservatively with patching, a contact lens, or cyanoacrylate adhesives. These solutions avoid the use of general anesthetics and possible corneal irregularities, which may lead to amblyogenic factors, depending on the age of the child. Admission to the hospital with close observation and antibiotic administration is ideal.
One must consider when faced with the self-sealing wound that a wound leak may develop when the edema from the cornea subsides. The ocular status could also be compromised by the activity of the child.
However, after a surgical decision has been made, it is best to proceed immediately with the repair to avoid possible endophthalmitis. A shield should be worn at all times by the patient to prevent additional complications to the eye. It is also prudent to wait until the laceration is repaired before adding medications to the eye, either in the form of antibiotics or mydriatics, which could prove toxic to the retina.
Every open globe should be treated as a potentially infected case until cultures, which should be taken at the time of surgery, are proven negative and no clinical signs of infection are present. Ideally, antibiotics should not be given until cultures are taken. If there is a delay in taking the child to the operating room, one must use clinical judgment. Broad-spectrum parenteral antibiotics should be initiated either before or during surgery as a precaution against endophthalmitis. Intravenous antibiotics should be continued for 2 to 3 days and then oral antibiotics continued for another 7 days. Cefazolin at a dosage of 50 to 100 mg/kg/day intravenously divided every 8 hours would provide broad spectrum coverage until culture results are available. There are many other choices for broadspectrum coverage. With time and availability of culture results, an antibiotic can be selectively targeted to the specific pathogen found.
OPERATIVE PLAN
The extent of the wound should first be explored so the surgeon understands the complete limits of the laceration. The operating microscope has facilitated this end and when possible it should be used at the time of surgery. The goal is a watertight globe with the lacerated tissues restored to as closely as possible to the original anatomy to help regain normal function.4
We have found that most prolapsed tissue can be repositioned within the first 48 hours. Repositioning of uveal tissue is contraindicated when tissues appear necrotic or infected; when this occurs they should be excised. Although a theoretical risk exists, it has not been documented that the risk of infection is greater if prolonged exposed tissue is repositioned so long as there is no evidence of necrosis or infection.5
Wound closure should begin by identifying landmarks that can be approximated. Lacerations through the sclera and cornea should first be closed at the anatomic limbus, thus securing normal apposition of the wound and preventing sliding and malapposition of the anatomy. Exposed uveal tissue can be repositioned with an iris or cyclodialysis spatula along with the use of viscoelastics. A close-as-you-go technique for long scleral-corneal lacerations is acceptable as well as halving techniques, in which you approximate the midline of the wound and approximate the two halves. This helps prevent “dog-ears” at the end of the wound.
Nonabsorbable suture (8-0 silk or 9-0 nylon) is preferable at the limbus. The suture of choice for corneal wounds is 10-0 nylon. The knots should be buried when possible. It is preferable to use longer suture bites at the limbus with smaller suture bites closer to the center of the cornea. This aids in preserving normal corneal architecture and prevents severe flattening, which can occur with longer central suture bites.
Vitreous prolapse through a scleral or corneal wound can occur. It is best excised at the lips of the wound using cellulose sponges and scissors. Tugging of the vitreous should be kept to a minimum to prevent retinal complications. As the vitreous is removed, the uveal structure can be repositioned. The use of a viscoelastic may assist in hydraulically repositioning uveal tissue.
Two suture techniques can be used to close the corneal wound. The round circular bite is probably the best but is the hardest to achieve. It is recommended that the box suture be used, which is a through-and-through suture with even bites on either side of the wound. A running suture technique should be avoided in these situations because it may distort the ends of the wounds.
Determining the status of the lens is important. If the lens capsule has been lacerated, the surgeon must decide whether to remove the lens now or later. Removal of the lens can only be attempted after watertight closure has been achieved. A severe corneal laceration may prevent good visualization or stabilization of the wound. Under such circumstances, it may be advisable to wait until the wound has had a chance to heal and can withstand the intraocular pressure generated during lens aspiration. Once the lens appears cataractous, it is best to remove it as early as possible because of the difficulties associated with a hard calcified lens that occur when cortex is exposed to aqueous, as well as the associated risk of amblyopia. Fibrinous precipitation can occur on the anterior lens capsule and masquerade as a cataract. This can be difficult to differentiate from a lens capsule rupture. A lens should only be removed at the time of the initial wound repair if there is evidence of anterior capsule rupture. It is best to wait until a cataract is definitely confirmed in the postoperative period (Fig. 2). Children older than 1 year who have a cataract and corneal laceration that precludes fitting with a contact lens are candidates for intraocular lenses. Only a surgeon with experience in treating pediatric cataracts with intraocular lenses should consider this. A safer situation occurs when the child is older than 3 years of age and will cooperate with a slit-lamp examination. If a lens needs to be removed, it is best to leave the posterior capsule intact for a secondary posterior chamber intraocular lens. If a cataract is mild and there is no capsule rupture, it is best to wait to perform the cataract extraction with intraocular lens insertion until a later date. This allows the posttraumatic inflammation to quiet as well as to decrease the risk of postoperative complications. Extreme care must be taken when removing a traumatic cataract in that there may be an associated zonular weakness increasing the possibility of nuclear loss into the vitreous.
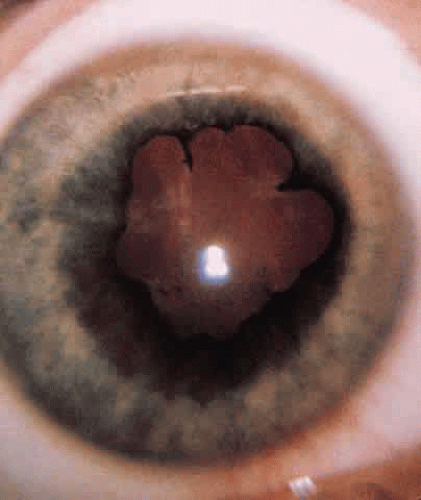 Fig. 2. A 5-year-old child with a traumatic cataract with posterior synechia that developed 3 months after blunt injury to the eye. |
Cefazolin (0.2 ml of 50-mg/ml concentration) should be injected under the conjunctiva at the end of the surgical procedure. Aminoglycosides should be avoided because of the risk of retinal toxicity.6 Subconjunctival injection of corticosteroids should be avoided until the surgeon is certain that no infection is present. Atropine ointment (0.5% for children younger than age 1 year and % for children older than 1 year) should be placed to ensure maximal cycloplegia.
POSTOPERATIVE MANAGEMENT
Control of postoperative inflammation with restoration of vision in the pediatric age range is critical. Many successful procedures have been performed but have resulted in poor vision because of irregular astigmatism and secondary amblyopia. In visually immature children (younger than 8 years old), plans must be made for visual rehabilitation as soon as the situation permits. This includes the use of contact lenses, patching of the normal eye, and a possible keratoplasty procedure to clear the pupillary space.7 Patching the injured eye for more than 24 hours following injury should also be avoided to prevent the risk of iatrogenic amblyopia. Corticosteroids, both topical and systemic, can be used early in the course of treatment. Treating severe inflammation and returning the child to a comfortable condition is paramount.
Children seem to heal much sooner than adults. It has been our experience that corneal sutures can be removed as early as 2 to 4 weeks after trauma. One should monitor signs of healing, such as suture loosening and early vascularization along the corneal wound. Clearing the visual axis and correcting any abnormal refractive errors are essential for a good visual outcome.
EYELID LACERATION
Laceration of the eyelids may or may not involve the lacrimal drainage system. The clinician should assume that if a laceration involves the medial canthal area, the lacrimal system is involved. Repair in the operating room with the opportunity to address the lacrimal system should be arranged.
If one is certain that the lacrimal system is not involved, the physician must use judgment to determine whether the child could tolerate repair in the emergency department. If anesthesia is required, it is wise to remember that a delay of even 48 to 72 hours is well tolerated. The eyelid has excellent blood supply, and this delay does not compromise the healing process. Therefore, if the child has eaten recently, one must not declare the case an emergency. It is best to wait until the conditions are more favorable. The child is placed on antibiotics and the repair is scheduled.
The first step is to clean the wound well. This should be done with minimal disruption to the surrounding tissue. When there are a large number of foreign particles, one should first try to irrigate the material from the wound. The next step should be the removal of individual particles with the use of fine forceps. Scrubbing tends to destroy the tissue and make repair more difficult.
It is usually not necessary to debride or “freshen” the wound edges. The more tissue left to close the wound, the more favorable the results. In a situation in which tissue has already been lost due to the injury, one should not consider primary grafts unless the extent of the injury threatens the integrity of the cornea. Major reconstruction should be delayed for 6 to 9 months.
EYELID MARGIN
An assessment of the laceration as well as a complete eye examination should be done. Concomitant ocular injuries are common. The laceration should be described according to its length, level or depth of involvement, loss of tissue, and mechanism of action (e.g., dog bite, knife wound). This aids in the plan of treatment. A barbed object, such as a fishhook, must be pushed forward and not pulled out. After the barb of the hook enters through the skin, wire cutters can be used to remove the barb and the remainder of the hook can be pulled backward through the entrance site.
The best approach is to close layer by layer, which helps maintain function and promote good cosmesis. Extruding fat should be excised because it increases the risk of infection. The orbital septum need not be closed so long as care is taken to close the other layers.
With a lid laceration involving the margin, the first step is to align the margin to avoid notching. With the use of 5-0 or 6-0 chromic catgut, the first suture is placed through the tarsal plate and as closely as possible to the lid margin (Fig. 3A). The sutures should remain intratarsal and one should avoid full-thickness bites, which can cause corneal abrasion during the healing process. This suture is left untied to allow access to the remainder of the wound. The next step is to close the length of the tarsus with interrupted sutures (see Fig. 3B).
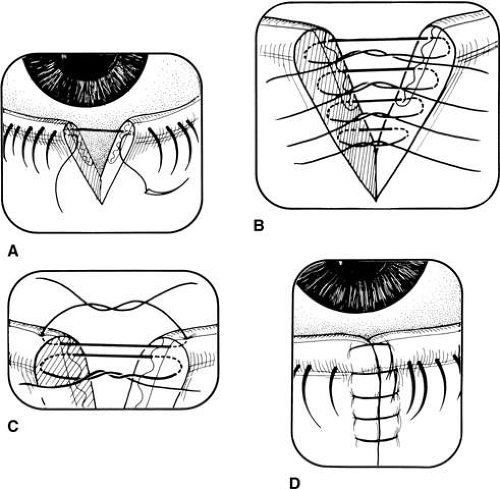 Fig. 3. A. Interrupted sutures are placed intratarsally. B. Silk suture is placed at the gray line. C. Intratarsal sutures are tied. D. Silk suture is used to align the margin anterior to the gray line. |
Next, the lid margin is aligned, and a 6-0 silk suture is placed at the level of the gray line into the tarsus on either side of the wound (see Fig. 3B). Now the physician can return to the first tarsal suture and tie it. The silk suture is tied loosely and left long to avoid corneal contact. A 6-0 Vicryl suture is also acceptable in children and may eliminate having to remove the suture at a later date.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


