Pediatric Eyelid Disorders
Forrest J. Ellis
EYELID DEVELOPMENT
Eyelid development is intimately associated with the development of the eye (1). During the fourth week of gestation, the optical vesicle forms as a projection from the side of the forebrain. The optical vesicle invaginates, forming the optic cup. The overlying ectoderm forms the lens placode, which separates and migrates internally to form the lens of the eye. The ectodermal surface overlying the optic cup develops into the cornea. Further development during week 6 results in small folds of the surface ectoderm with its underlying mesenchyme. These two folds become the upper and lower eyelids. These folds grow toward each other and ultimately result in fusion of the upper and lower eyelids between weeks 8 and 10 of gestation. The eyelids remain fused until approximately the sixth month of gestation, at which time separation of the eyelids occurs. In addition to primary eyelid developmental abnormalities, eyelid and ocular development may be affected by abnormalities or defects in facial development. Abnormalities in orbital development can also cause secondary abnormalities in eyelid development.
ANATOMY OF THE EYELIDS
Upper Eyelid
The upper eyelid margin forms a curved arch from the medial canthus to the lateral canthus and overlies the superior 1 to 2 mm of the cornea. The peak of this curve is approximately 1 mm nasal to the center of the cornea. The upper eyelid crease is formed by the attachment of strands of the external levator aponeurosis to the skin (2). An absent upper eyelid crease can be seen in conditions of abnormal levator development such as congenital ptosis. However, the normal Asian eyelid has a low set and less developed eyelid crease. In addition, dehiscence of the levator aponeurosis can result in an abnormally elevated eyelid crease.
The upper eyelid tarsus is approximately 10 mm in its vertical height in the adult and proportionately shorter in children. It is formed of dense fibrous tissue. Medially and laterally the tarsus is attached firmly to the orbital rims by the canthal tendons. The medial canthal tendon attaches to the anterior and posterior lacrimal crests and the fascia of the lacrimal sac. The lateral canthal tendon attaches to the lateral border of the tarsus and to the Whitnall tubercle inside the lateral orbital rim. The lateral canthus is normally even with or just slightly above the medial canthal tendon in the horizontal plane. Externally an extra fold of skin can be seen in the medial canthal area overlying and potentially obscuring the medial canthal tendon. This extra fold of skin is referred to an epicanthal fold.
The anatomy of the upper eyelid overlying the tarsal plate consists of eyelid skin covering the orbicularis oculi muscle. This pretarsal orbicularis is adherent to the underlying tarsal plate. Conjunctiva is also firmly adhered to the tarsus posteriorly. Superior to the tarsus, the skin covers the preseptal orbicularis muscle. Beneath the preseptal muscle is the orbital septum, which defines the anterior boundary of the orbit and overlies orbital fat. The orbital septum is important in eyelid anatomy. In Caucasian upper eyelids, the orbital septum and levator aponeurosis fuse at approximately the superior tarsal boarder 10 mm above the eyelid margin. However, in Asian eyelids, the septum inserts much lower into the levator aponeurosis, resulting in inferior displacement of orbital fat and a lower eyelid crease (3). Posterior to the levator aponeurosis is the underlying Müller muscle.
Lower Eyelid
The lower eyelid margin usually crosses the inferior corneoscleral limbus. Lower eyelid anatomy has similar features to upper eyelid anatomy (4). However, the lower eyelid tarsus is only 5 mm in its greatest vertical height. Arising from the area of inferior rectus muscle is the capsulopalpebral fascia. In a similar, but less well-developed fashion to the levator aponeurosis, this fascia inserts into the lower eyelid tarsus where it retracts and stabilizes the lower eyelid. The orbital septum of the lower eyelid inserts directly onto the tarsus.
Levator Palpebrae Superioris and Müller Muscle
The levator muscle has its origin at the lesser wing of the sphenoid. It runs posterior to anterior in the superior aspect
of the orbit. Just inside the superior orbital rim, the levator muscle crosses and fuses with the Whitnall ligament. This attachment provides support to the levator muscle and aponeurosis. At this point, the levator muscle turns in an inferior direction while becoming more fibrous. The levator aponeurosis spreads out horizontally to form a fan-shaped structure with attachments medially and laterally, the medial and lateral horns, which insert in the periosteum. The levator aponeurosis inserts broadly across the anterior surface of the upper eyelid tarsus. Small strands of the levator aponeurosis also project anteriorly, inserting into the eyelid skin and forming the eyelid crease.
of the orbit. Just inside the superior orbital rim, the levator muscle crosses and fuses with the Whitnall ligament. This attachment provides support to the levator muscle and aponeurosis. At this point, the levator muscle turns in an inferior direction while becoming more fibrous. The levator aponeurosis spreads out horizontally to form a fan-shaped structure with attachments medially and laterally, the medial and lateral horns, which insert in the periosteum. The levator aponeurosis inserts broadly across the anterior surface of the upper eyelid tarsus. Small strands of the levator aponeurosis also project anteriorly, inserting into the eyelid skin and forming the eyelid crease.
The Müller muscle complex arises from the posterior aspect of the levator muscle, lies along the posterior surface of the levator aponeurosis, and inserts into the superior border of the tarsus.
Eyelid Innervation
Cranial nerve VII (the facial nerve), which divides into six branches, innervates the facial musculature. The temporal branch of the facial nerve provides innervation to the orbicularis oculi, frontalis, pars ciliaris, and corrugator muscles. However, the superior division of cranial nerve III innervates the levator palpebrae superioris muscle. The Müller muscle is innervated by the sympathetic nervous system. Interruption of ocular sympathetic supply causes ptosis, miosis, and anhydrosis. This triad of signs is known as Horner syndrome (5).
Vascular Supply to the Eyelids
The vascular supply to the eyelids is rich with many collaterals. The supraorbital, supratrochlear, lacrimal, and dorsal nasal branches of the ophthalmic artery supply the eyelids, forehead, and orbit. An anastomosis between the dorsal nasal and lacrimal arteries in the upper eyelid forms the marginal arcade, which lies 2 mm above the eyelid margin between the tarsus and orbicularis oculi muscles. A peripheral arcade is located at the superior border of the tarsus between the levator aponeurosis and Müller muscle. The lower eyelid has a similar anatomic configuration of the arterial arcades. A rich venous drainage network exists throughout the eyelids. Because of the rich vascular supply, ischemic necrosis of the eyelids is rare.
EYELID DISORDERS
Anophthalmos and Microphthalmos
True anophthalmos is an extremely rare condition and results from an absence of the development of the optic vesicle. Most cases of clinical anophthalmos likely represent severe microphthalmos when careful histology is obtained from serial orbital sections. Microphthalmos represents a range of ocular developmental abnormalities from near complete absence of identifiable ocular structures to a small normally formed eye, a condition referred to as nanophthalmos. Approximately 25% of patients with anophthalmos/microophthalmos have a diagnosable genetic syndrome (6,7). Because eyelid and orbital development are dependent on the underlying ocular development, microphthalmos often is associated with abnormal or reduced orbital bony size. Eyelid deformities that result include shortened horizontal palpebral fissure lengths. The mainstay of treatment involves serial prosthetic conformers to enlarge the cul-de-sacs. In more severe cases, the orbital volume can be expanded using dermis fat grafts, orbital implants, and orbital expanders (8). Soft tissue growth will parallel bone growth. Using these various techniques, an acceptable cosmetic appearance is often achieved.
Cryptophthalmos
Cryptophthalmos is an extremely rare condition in which there is complete failure of development of the eyelid folds. One of the most distinct features of cryptophthalmos is failure of the brow to develop normally, resulting in fusion of the hairline and brow. This is distinct from an abnormal separation of the eyelid folds. Without development of the normal eyelid folds, the underlying cornea and conjunctiva do not normally form. The anterior segment of the globe is severely malformed, and the posterior segment of the globe is sometimes disorganized. If attempts are made to separate the eyelids, then the globe will often require corneal transplantation to close the anterior segment defect and mucous membrane grafting to form conjunctival cul-de-sacs (9). Preoperative evaluation with an electroretinogram, visual evoked potentials, imaging studies, and ultrasound may provide preoperative insight into the structure and function of the underlying globe. While reconstructive surgery may allow for an improved cosmetic result, useful vision is occasionally achieved. When associated cutaneous syndactyly, malformations of the larynx and genitourinary tract, craniofacial dysmorphism, orofacial clefting, mental retardation, and musculoskeletal anomalies occur, Fraser syndrome should be considered (10).
Congenital Eyelid Coloboma
A congenital defect involving the absence of a portion of the eyelid margin is an eyelid coloboma (Fig. 17.1). Coloboma may affect either the upper or lower eyelids and may vary in size from a small eyelid marginal defect to a near complete absence of the eyelids. Coloboma more typically occur in the nasal aspect of the upper eyelid, and large eyelid coloboma can result in corneal exposure and ulceration.
The etiology of colobomas is varied. Abnormal migration patterns of ectoderm and mesoderm may cause abnormal development of the eyelid margin. Colobomas may also result from a mechanical disruption of eyelid development such as amniotic bands or facial clefts (Fig. 17.2). Eyelid colobomas can be seen in association with other abnormalities
including dermoids, cleft lip, microphthalmia, and ocular colobomata. Coloboma of the upper eyelids occur commonly in Goldenhar syndrome.
including dermoids, cleft lip, microphthalmia, and ocular colobomata. Coloboma of the upper eyelids occur commonly in Goldenhar syndrome.
 FIGURE 17.1. Upper eyelid coloboma. |
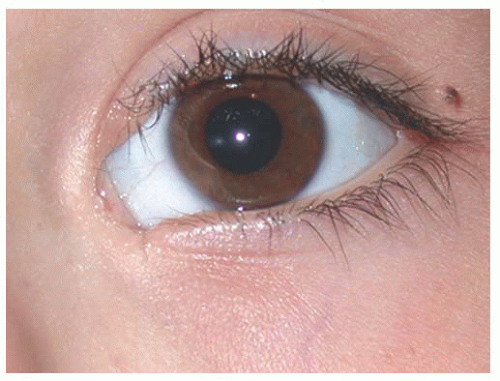 FIGURE 17.2. Small medial lower eyelid congenital cleft, resulting in canalicular atresia. |
Treatment of upper eyelid coloboma should be directed at maintaining lubrication and protection for the ocular surface. Surgical correction is not emergent as long as the corneal surface is being protected. A larger coloboma may require more aggressive lubrication and perhaps occlusive dressing prior to surgical closure. For smaller colobomas, surgical repair during the latter half of the first year of life is preferable to allow for tissue growth. For defects less than 25% of the horizontal eyelid width, direct closure after excision of the defect is all that is required. The edges of the defect are excised to form a pentagonal defect and then the tarsus is closed with three interrupted absorbable sutures. The eyelid margin is closed with sutures anterior to, through, and posterior to the gray line. The skin is reapproximated with interrupted sutures. Larger defects up to 40% of the eyelid margin can be closed by a lateral canthotomy and cantholysis with medial rotation of the eyelid. Larger eyelid defects often require a free tarsal conjunctival graft. Eyelidsharing procedures (e.g., Hughes procedure), which occlude the line of sight, should be avoided in children as they will induce occlusion amblyopia. Because most eyelid colobomas causing corneal exposure are in the upper eyelid, a lateral canthotomy usually can be performed and the eyelid defect closed nasally as described above. If necessary, a temporal tarsal conjunctival sharing procedure can then be performed, taking care not to occlude the visual axis.
Pseudocoloboma
More commonly, pseudocoloboma of the lower eyelid are seen in craniofacial synostosis (Treacher Collins syndrome) (Figs. 17.3 and 17.4). With these pseudocolobomas, the eyelid margin is intact but there is a facial cleft laterally, which results in an inferior and lateral displacement of the lower eyelid. Treacher Collins syndrome is caused by a first brachial arch abnormality. Ophthalmic findings include microphthalmos, iris coloboma, and absence of the puncta. Hypoplasia of the maxilla and zygoma are common with an antimongoloid slant to the palpebral fissures. Deformations of the external ear and hearing loss are associated with this syndrome. Simple soft tissue tightening and elevation of the lateral canthal tendon is frequently ineffective in correcting the lateral dystopia of the eyelid because there is often an absence of vertical and horizontal eyelid tissue. For this reason, transposition flaps from the upper to lower eyelids are useful in addition to resuspension of the lateral canthal tendon.
Ankyloblepharon
Ankyloblepharon is caused by failure of eyelid separation or from an abnormality in the migration of the mesodermal elements of the eyelid. Ankyloblepharon filiforme adnatum may
be isolated, demonstrating fine bands of tissue between the upper and lower eyelids, or it may be seen with trisomy 18 or other chromosomal abnormalities (11,12). In addition, ankyloblepharon may be part of the Hay-Wells syndrome, which is characterized by congenital ectodermal dysplasia, alopecia, scalp infections, dystrophic nails, hypodontia, ankyloblepharon, and cleft lip and/or cleft palate (13). The treatment of ankyloblepharon is entirely surgical. The bands of the eyelid are separated, and the eyelid margins are reformed as necessary. Figure 17.5 shows ankyloblepharon in a newborn.
be isolated, demonstrating fine bands of tissue between the upper and lower eyelids, or it may be seen with trisomy 18 or other chromosomal abnormalities (11,12). In addition, ankyloblepharon may be part of the Hay-Wells syndrome, which is characterized by congenital ectodermal dysplasia, alopecia, scalp infections, dystrophic nails, hypodontia, ankyloblepharon, and cleft lip and/or cleft palate (13). The treatment of ankyloblepharon is entirely surgical. The bands of the eyelid are separated, and the eyelid margins are reformed as necessary. Figure 17.5 shows ankyloblepharon in a newborn.
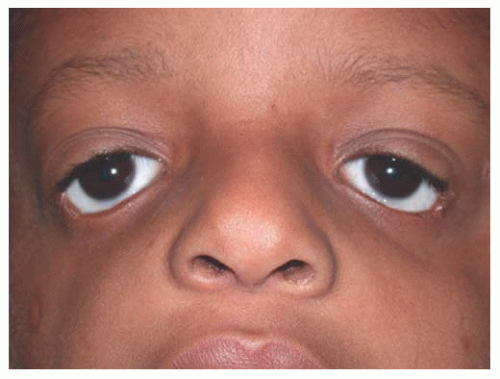 FIGURE 17.3. Pseudocolobomata of the lower eyelids associated with Treacher Collins syndrome. |
 FIGURE 17.4. Small partial coloboma of the upper eyelid. |
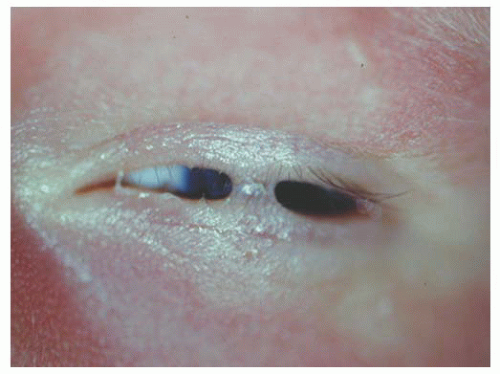 FIGURE 17.5. Ankyloblepharon in a newborn. |
Distichiasis
Distichiasis occurs when a developmental abnormality results in cilia formation in association with metaplastic meibomian glands. This condition is often asymptomatic although these lashes may cause superficial corneal irritation and abrasion. In an acquired form, distichiasis may occur with chronic eyelid inflammation such as blepharitis, trachoma, and Stevens-Johnson syndrome (Fig. 17.6).
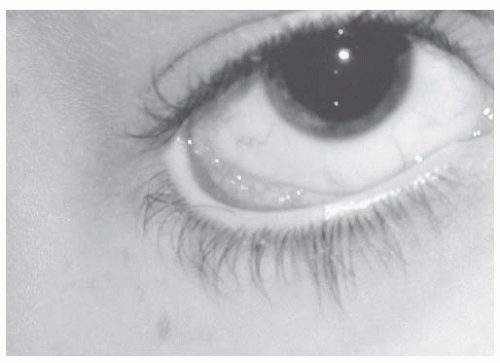 FIGURE 17.6. Acquired distichiasis. Eyelash in association with a meibomian gland orifice. |
Trichiasis
Trichiasis refers to an acquired eyelash abnormality resulting from normally located but misdirected cilia. Chronic eyelid inflammation is the most common cause for trichiasis.
Treatment of eyelash abnormalities is not required in the absence of any abnormality of the corneal surface. Electrolysis or split thickness eyelid resections can be used to remove the lash follicles (14). In addition, direct excision of the lash follicles is possible.
Congenital Ectropion
Congenital ectropion is rarely found in isolation. When the lower eyelid is involved, it is often part of the blepharophimosis syndrome or Treacher Collins syndrome. Also, congenital eyelid ectropion may be seen in patients with neonatal erythroderma (collodion baby) (15). When secondary to an insufficiency in the vertical extent of the skin and orbicularis layers, a full-thickness skin graft or transfer flap is usually required in addition to a lateral tightening of the eyelid.
Congenital Entropion and Epiblepharon
Epiblepharon results from an extra fold of pretarsal lower eyelid skin and orbicularis, which rotates the lower eyelid cilia and margin inward (Fig. 17.7). Epiblepharon is more common in Asian eyelids. With downward pressure over the excess skin, the eyelid margin assumes a normal appearance. This condition is typically self-limited and resolves with facial growth. Most children are relatively asymptomatic without corneal injury. If corneal surface changes occur with persistent corneal irritation, a small ellipse of subciliary skin and orbicularis muscle can be removed. Since lower eyelid retraction can result from excessive skin excision, only a minimal amount of skin is removed.
Congenital lower eyelid entropion is caused when preseptal orbicularis overrides the pretarsal orbicularis (Fig. 17.8). In
addition, there is laxity of the lower eyelid retractors, allowing a true inward rotation of the lower eyelid. Correction requires reattachment of the lower eyelid retractors to the lower border of the tarsus, elimination of horizontal eyelid laxity when present, and resection of overriding skin and orbicularis.
addition, there is laxity of the lower eyelid retractors, allowing a true inward rotation of the lower eyelid. Correction requires reattachment of the lower eyelid retractors to the lower border of the tarsus, elimination of horizontal eyelid laxity when present, and resection of overriding skin and orbicularis.
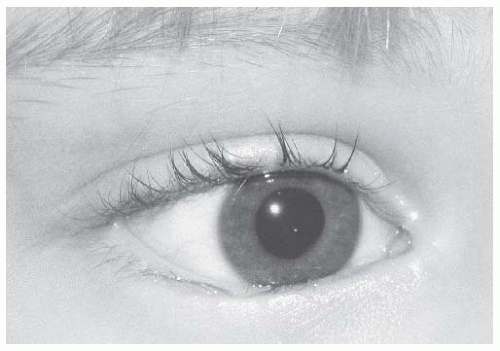 FIGURE 17.7. Epiblepharon, which typically resolves spontaneously. |
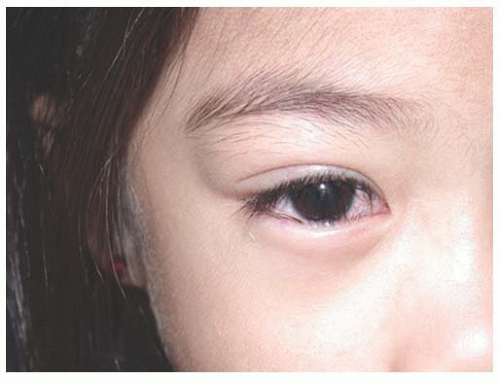 FIGURE 17.8. Lower eyelid entropion with inward rotation of the eyelid, necessitating surgical correction. |
Congenital horizontal tarsal kink results in entropion of the upper eyelid and may be associated with congenital levator aponeurotic disinsertion. More important, corneal ulceration occurs in 50% of cases (16).
Congenital Eyelid Retraction
Congenital eyelid retraction, especially of the lower eyelid, may occur in isolation or secondary to structural anomalies, resulting in very shallow orbits and proptosis (Fig. 17.9). While some infants will have transient upper eyelid retraction, persistent superior scleral show in the absence of a structural cause warrants a medical evaluation for thyroid or neurologic disease. Options to correct eyelid retraction are müllerectomy and levator recession. Spacer grafts are occasionally necessary.
 FIGURE 17.9. Lower eyelid retraction associated with shallow orbits and relative proptosis in a patient with Pfeiffer syndrome. |
Euryblepharon
Euryblepharon is a condition characterized by increased vertical separation of the temporal aspect of the palpebral opening such that the palpebral conjunctiva is not in apposition with the eye. The lateral canthus is usually displaced inferiorly. This condition is characterized by a lack of vertical skin height, and treatment requires a lateral canthoplasty as well as possible skin graft into the lower eyelid to provide additional vertical height.
Epicanthus
The epicanthus consists of a fold of skin in the medial canthal region overlying the medial canthal tendon. This condition can occur in isolation or it can be associated with multiple genetic disorders such as trisomy 21 and blepharophimosis syndrome. Epicanthal folds are generally classified as being one of the four types: epicanthus supraciliaris, epicanthus inversus, epicanthus palpebralis, and epicanthus tarsalis.
Epicanthus tarsalis is the normal medial canthal structure seen in many Asian eyelids (Fig. 17.10). The eyelid fold arises in the region of the upper tarsal plate and extends to the skin of the medial canthus. Epicanthus inversus is seen in isolation and in patients with blepharophimosis syndrome. This occurs when the fold of skin begins in the lower eyelid tarsal region and extends up through the medial canthal region toward the brow. Epicanthus palpebralis occurs when a fold runs from the upper eyelid tarsal region to the lower border of the orbit. Epicanthus supraciliaris occurs when the fold arises in the brow and terminates in the area of the lacrimal sac.
Epicanthal folds can be corrected with a variety of techniques, including a YV plasty most simply (Fig. 17.11). In addition, the Mustarde (17) and Roveda techniques have been described.
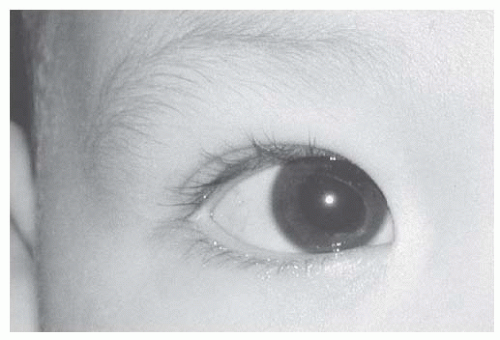 FIGURE 17.10. Epicanthal fold, most consistent with epicanthus tarsalis. |
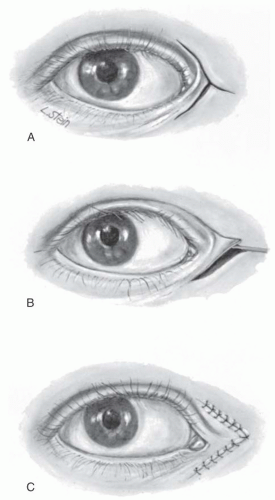 FIGURE 17.11. Surgery for epicanthus. A: Incision for preparing the skin flap. B: Undermining of skin to allow for movement of the tip. C: Skin sutures in a V-shape, flattening the epicanthal fold. The skin at the junction of the Y flap is rotated medially to the apex of the V, thus flattening the epicanthus. |
Telecanthus
Telecanthus refers to a wide intercanthal distance, differentiated from hypertelorism, which describes an increased interorbital bony separation. Telecanthus is often associated with epicanthus and blepharophimosis. When associated with epicanthal folds, telecanthus may be corrected using the same procedures that are used to treat epicanthus. However, medial canthoplasty and/or transnasal wiring may be necessary in more severe cases.
Blepharoptosis
Ptosis of the child’s upper eyelid is most often congenital. It is occasionally due to congenital myasthenia, congenital fibrosis of the extraocular muscles, syndromic associations, or acquired abnormalities such as loss of innervation to Müller or levator muscle. In addition, mechanical factors can contribute to ptosis, such as relative enophthalmos following an orbital fracture, tumor, or traumatic injury. Congenital ptosis of the upper eyelid is typically seen in association with abnormal development of the levator palpebral complex (Fig. 17.12). Although typically sporadic, familial ptosis has been linked to chromosome 1p (18). Perhaps abnormal neurologic innervation during development of the levator muscle results in abnormal development of the muscle complex, similar to what occurs in congenital fibrosis syndrome (19). Congenital ptosis occurs either unilaterally or bilaterally. Superior rectus muscle weakness can occur in association with congenital ptosis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


