Pediatric Ophthalmology
Edited by P. F. Gallin
Thieme Medical Publishers, Inc.
New York ©2000

1

Pediatric Eye Examination
The examination of the pediatric patient brings a host of challenges not incurred during the adult examination. Children are able, even from infancy, to give us a large amount of information. All children, independent of age, can have a complete ophthalmological examination. It is our job as ophthalmologists to learn how to glean this information effectively. There are significant differences between the design and function of the adult and pediatric exam. It is the goal of this chapter to arm the general ophthalmologist and ophthalmologist-in-training with the techniques needed to perform a standard eye exam on children of all ages. This chapter is a guide to the eye exam and must be adapted to specific problems and situations.
To begin, it is important to be equipped with some essential tools. It is highly recommended that you assemble the following “shopping list” before embarking on your first exam. You can create many items on this list inexpensively on your own.
Two or three medium-sized colorful toys—plush stuffed animals work well
Three or four tongue depressors decorated with a variety of cartoons
Pictures (near targets)
Tongue depressor with number chart or letters
Occluder with and without pinhole
Wall eye charts, including Snellen, Illiterate E, and Allen figures
Hand-held Allen cards
Prism bars or individual prism box
Pediatric trial frames
Titmus test
+ 3.50 spectacles (single vision)
 Rapport
Rapport
Once you have obtained the necessary materials for a pediatric exam, it is important to establish the appropriate rapport with a child. Good rapport can allow you to gain the most information. A child who is made to feel comfortable will assist the examiner during the exam. The following are several guidelines, which we have found as effective techniques to decrease a child’s anxiety level and increase his or her interactions with the examiner.
1. Make the child feel comfortable as soon as he enters the room. A cheerful and friendly hello immediately places the child and parent at ease.
2. Ask the child a question to which he knows the answer. Once a child begins to speak, his anxiety level decreases dramatically. In addition, a question that he knows the answer to will build confidence. School-aged students usually respond to questions about grade, teacher, and favorite subject. Younger children enjoy telling you about their favorite television program or their age. Ask them if they are older than you know they are.
3. Allow the child to be comfortable in the examination chair. Offer young children the opportunity to sit on a parent’s lap.
4. Do not talk “down” to older children. Try to speak to them in an age appropriate manner and avoid a sing-song voice.
 History
History
It is vital when examining children not to miss a window of opportunity. Most children have a limited attention span, and, once they have lost interest in the examination, obtaining information becomes very difficult. Therefore, it is not recommended to start your examination with a long history-taking session between yourself and the parent.
History can be obtained by a questionnaire distributed to a parent in the waiting area. The sample included here can be adapted for your particular practice situation (Fig. 1-1). It is important to include pregnancy and delivery information (including medications). A family history of strabismus and amblyopia as well as developmental and family histories are important. The past medical and ocular histories are also necessary. A parent’s statement of the chief complaint is helpful and ensures that you will address the parent’s primary concern.
It is important to understand that the indirect nature of the history (mainly from parents) presents unique problems in the pediatric exam. Children will rarely complain of unilateral visual loss and surprisingly do not usually complain of severe bilateral visual loss. Therefore, the pediatric exam may yield surprises that are not presented during history taking.
 Examination
Examination
Visual Acuity
The pediatric ophthalmic exam should begin as soon as the patient enters the room. Observing the patient’s approach to the examination chair allows the examiner to note head position, eye position, gait, and other clues to the diagnosis of ocular disease. Watching a child inspect your office can also yield important clues.
Visual acuity in a child should always be assessed by the ophthalmologist. The examiner’s subjective assessment is extraordinarily important. This is used as a standard against which the results are measured. Children are eager to please; therefore, poor vision in one eye may be missed by the child’s peeking around the occluder (Fig. 1-2). Always watch a child while checking visual acuity. In addition, decreased visual acuity due to occlusion nystagmus may be missed by a technician. Also, it is important to be aware that some children must be constantly coaxed throughout checking visual acuity. A few words of encouragement can sometimes move a child ahead several lines. A suspicion of malingering can also be noted at the time visual acuity is checked. Inconsistent acuities may clue the examiner to this situation. The acuity can be repeated again later in the examination beginning with the “worse” eye.
Visual acuity testing must be tailored to the child’s age and ability. Infant visual acuity is the most challenging for an examiner, but important information may be gleaned from observing the infant. The ability to fix and follow an object should be present by 2 to 3 months of age (Fig. 1-3). Yet it can be present at birth in a very healthy, alert infant. Unfortunately, infants from birth to several months of age often show no response to inanimate objects such as toys or a flashlight. The human face is generally the strongest visual stimulus for the young infant. It is important to be aware that young infants may not be capable of producing the normal slow, smooth pursuit movements seen in older children and adults.
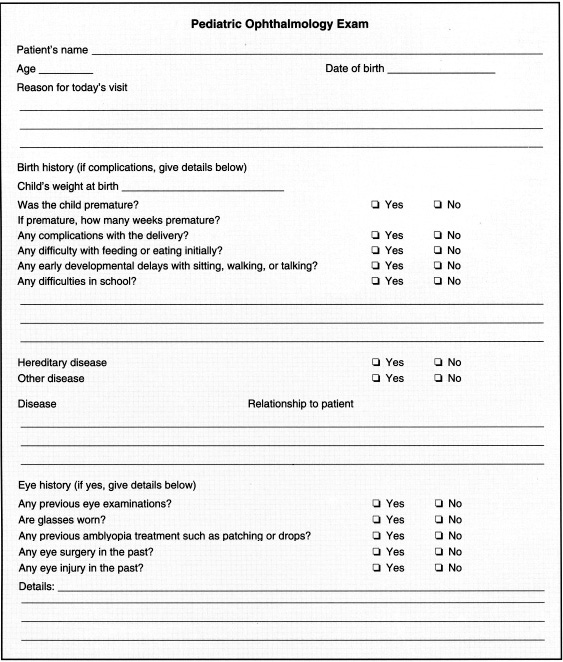
FIGURE 1-1. Sample parent questionnaire used to obtain patient history.
Ask the parent if the child “sees” his or her face. In the case of a “blind” baby the parents will answer “no” or be uncertain. Young infants may display jerky, hypometric saccades in the same direction as the target. By 6 months of age, the average child should be able to fixate on moving toys and small targets within 6 feet.
Fixation of each eye should be evaluate fixation is central steady maintained (CSM).
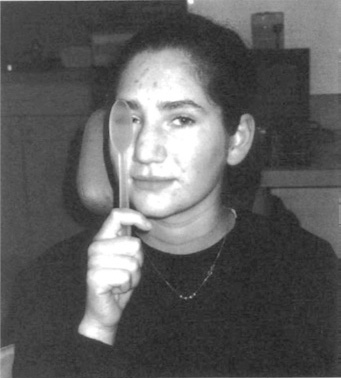
FIGURE 1-2. Peeking around occluder.
1. Central—as opposed to eccentric fixation
2. Steady—as opposed to nystagmus
3. Maintained—if fixation is held by the eye even when the other is uncovered
Cover the left eye first and note if the child follows a light or an object. It is also helpful to gauge how disturbed the infant is when the eye is covered. An infant with a severely amblyopic eye may become very anxious when his preferred eye is covered. An infant will push away the patch when the seeing eye is covered, yet remain passive when the same is done to a poorly seeing eye. Check for occlusion nystagmus at this time. In a strabismic patient, you must watch both the covered and the uncovered eyes closely, especially as the occluded eye is uncovered. The assessment of vision in an infant is very subjective and exceedingly difficult, requiring much judgment.
Optokinetic nystagmus (OKN) can be used as evidence of very gross visual acuity. The examiner may use an OKN drum or tape to elicit OKNs in an infant. A simple method of eliciting OKNs is to carefully turn the infant while the examiner holds the infant approximately 10 to 45 inches from the face. Also, visual evoked responses (VERs) may be used to assess vision. These techniques use checkerboard or striped gratings of various spatial frequencies combined with electrode monitoring of the brain. (See Chapter 21 on visual acuity testing.)
Preferential looking is based on observations that infants are more interested in looking at a pattern than at homogeneous fields. The infant is exposed to a particular black and white striped pattern and an identically sized gray field of equal luminance. The observer under specific lighting conditions and at a fixed distance quantifies the amount of time that the infant focuses on each field. Preferential looking is useful in the evaluation and follow-up of preverbal patients with disorders affecting visual acuity. It is especially useful to compare relative acuity between the two eyes. Unlike VER, preferential looking is dependent upon eye movements.
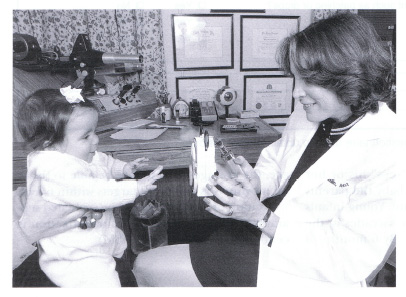
FIGURE 1-3. Baby looking at near target.
Snellen Visual Acuity
The American Academies of Ophthalmology and Pediatrics recommend a vision screen at the age of 3. The age at which a child can participate in acuity testing varies widely. Some 2-year-olds can read the Snellen letter or number chart, whereas some 6-year-olds cannot. A hierarchy of increasing difficulty and accuracy in testing begins with the Allen cards (Fig. 1-4). The illiterate E game is extraordinarily accurate, although some 3-year-olds cannot cooperate. Often a normal child with a perfectly normal exam will only read up to the 20/30 line. Symmetry in acuity on vision screens is of more importance than the actual acuity.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


