Pediatric Cataract Surgery
Kenneth P. Cheng
Albert W. Biglan
The treatment of an infant or child with a cataract requires different decision processes and modifications in surgical procedures compared with the treatment of an adult with a cataract. The developing visual system, growth, and anatomic differences in the eye and related structures, and psychosocial differences between children and adults, contribute to the necessary differences in treatment.
The adult eye is fully developed, and the visual pathways are mature. Management after cataract surgery is principally a process of optical rehabilitation to achieve restoration of vision. In children, however, the eye and the visual pathways are developing, and the operation to remove a cataract is only the first step in a long process aimed at promoting normal development of the visual system and achieving the best possible visual acuity in the affected eye. This chapter reviews the indications, surgical techniques, complications, and expected results of cataract surgery in infants and children.
INDICATIONS FOR SURGERY
In children affected by either unilateral or bilateral cataracts, the indications for surgery and the risk-benefit ratio decisions are more complex than for an adult patient. In an adult, the risks of the procedure are low and the benefits are high, and the presence of a cataract that noticeably degrades vision or alters the patient’s lifestyle is a sufficient indication for surgery.
In a child, additional factors must be considered, such as the health of the child, the availability of resources for perioperative care, and the availability of anesthesiologists who are trained in the care of infants and young children. In adults, the surgery can be scheduled to accommodate the convenience of the patient and the surgeon. In children, the timing of surgery may be dictated by the degree of maturation of the visual system. Surgery may need to be performed urgently to facilitate the effective treatment of amblyopia. In infants with unilateral congenital cataracts, a critical period in visual development exists after birth, during which treatment should be initiated to optimize the possibility for promoting visual development in the affected eye. Evidence suggests that this critical period is before the first 6 to 17 weeks of age, and earlier surgery is felt to minimize deprivation amblyopia.1,2,3
Another difference is the frequent presence of structural abnormalities of the child’s globe and visual pathways. These abnormalities can influence the visual result that is achieved in these affected children. Affecting the results achieved in all young children are the inherent limitations in the available methods of optical correction and problems with compliance with optical correction and amblyopia therapy. Additionally, persistence with treatment of strabismus, glaucoma, and other related complications is needed to maintain a successful visual result.
Because of the difficulties with correction of aphakia in children, surgery may not be advisable in some cases. For example, observation of a monocular partial lens opacity that decreases visual acuity to 20/40 in an amblyopia-susceptible 2-year-old child may be preferable to making that child aphakic and intolerant of contact lenses or even pseudophakic without the ability to accommodate, and intolerant of glasses with bifocal lenses. The reverse also can be true. Irreversible deprivation amblyopia can be caused by a partial lens opacity, for example, posterior lenticonus, in an infant or a young child. In these cases, the opportunity to achieve high levels of central vision may be permanently lost if surgery is delayed.4 Because of these many factors, the accepted 95% success rate for excellent vision following cataract surgery in adults is not possible in children.
Not all cataracts require surgical treatment. Eyes with punctate or small anterior polar cataracts and others with partial opacification of the lens, such as posterior lenticonus, which only slightly interferes with the refraction of light, are best followed and not surgically treated (Fig. 100-1). In preverbal children or in children who are not able to have formal measurements of visual acuity performed, it is up to the surgeon to make the oftentimes difficult decision on the effect that the cataract may have on visual acuity, amblyopia, and visual development. In some cases, it is difficult to determine whether the presence of a partial cataract is responsible for a decrease in visual acuity or whether the refractive error or optical distortion produced by the cataract has produced a mild, reversible form of deprivation amblyopia. In these situations, correction of the refractive error and a trial of occlusion therapy should be attempted. If the visual acuity improves, it may be deduced that amblyopia was responsible for some of the decrease in visual acuity and that the optical distortion produced by the partial cataract is not solely responsible for all of the decrease in acuity.
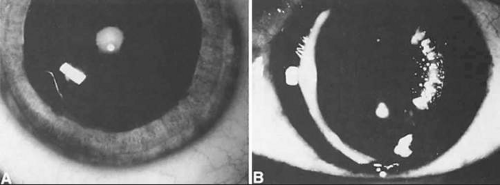 Figure 100-1. Cataracts that do not require surgical treatment. A. Anterior polar cataract. Visual acuity is 20/25. B. Partial punctate or cerulean cataract. Visual acuity is 20/30. |
TREATMENT GUIDELINES
When a cataract is extensive or if a partial cataract is present and the vision does not improve with a trial of occlusion therapy, cataract surgery should be considered. The guidelines for cataract surgery given in this section are based on the extent of the lens opacity and whether the cataract is isolated to one eye or both. Specific indications for cataract surgery, however, should be considered individually for each child.
Unilateral Partial Cataract
Children who have monocular partial cataracts should undergo cataract surgery when visual acuity in the affected eye is judged to be <20/70, when there is a loss of central fixation, or when visual deprivation is sufficient to cause strabismus. In questionable cases or when the cataract is small or only partially obstructs the visual axis, a trial of amblyopia treatment along with optical correction of anisometropia and dilation of the pupil, if necessary, to provide a clear visual axis4 should be performed before the decision is made to remove a partial cataract.
Unilateral Complete Congenital Cataract
Infants and children younger than 8 years of age who have monocular complete cataracts that are present from birth should have cataract surgery performed as soon as they are medically stable (preferably before 17 weeks of age). A child who is older than 8 years of age may have a complete monocular cataract removed to improve peripheral vision, to visualize the fundi, or for cosmesis. Treatment of amblyopia with improvement of central vision in children who have had complete congenital cataracts with surgery after 2 years of age usually is unsuccessful. If there was a possibility that the cataract was only partial during infancy or developed during infancy, with some opportunity for stimulation of the macula with clearly formed images, the cataract should be removed at any age in an attempt to regain central visual acuity.
Bilateral Partial Cataracts
Children younger than 8 years of age who have bilateral partial cataracts should undergo surgery when vision in either eye is judged to be <20/70, if visual deprivation is producing strabismus, or if there appears to be a risk for the development of nystagmus as a result of visual deprivation.
Bilateral Complete Cataracts
If the lens opacity is complete and involves both eyes, the cataract should be removed in the eye with the most complete lens opacity. The fellow eye should be treated as soon as the first eye recovers from surgery. This interval should be brief (5–10 days) in very young children. If a health problem precludes repeated anesthetic sessions, consideration may be given to performing the surgery on both eyes during the same anesthetic session, with the use of different instrumentation and separate operative fields.5,6
OTHER CONTRIBUTING FACTORS
Decisions to perform cataract surgery can be difficult when young or developmentally delayed children cannot provide subjective visual acuity responses. In these situations, the decision to remove a cataract depends on the size, density, type, location, and progression of the opacity and the estimated effect of these factors on vision. Estimates of the effect of a partial cataract on vision can at times be difficult, even for experienced examiners; in difficult cases, second opinions can be helpful.7
Size and Density
Cataracts that are central in location and larger than 1.5 to 2 mm obstruct light entering the eye sufficiently to reduce visual acuity and impede development of the visual system. In this situation, a trial of dilating the pupil with topical applications of 2.5% phenylephrine drops three times a day to allow light to enter around the opacity may result in an improvement in visual acuity. Pupils that dilate poorly with phenylephrine may respond to 0.5% atropine eyedrops; however, the accompanying cycloplegia necessitates the use of bifocals to correct the cycloplegic refractive error and the lack of accommodation. Frequent monitoring of visual acuity and pupil size at different times of the day and under different lighting conditions is recommended. Improvements in acuity may be temporary if the lens opacity progresses in size.
Type and Location
Usually, anterior polar cataracts are visually insignificant and allow normal visual development (Fig. 100-1). However, some affect vision, and all require careful monitoring.8 Centrally located cataracts that are on or near the posterior lens capsule have a greater effect on the refraction of light and visual acuity (Fig. 100-2). Nuclear cataracts associated with metabolic disorders or prenatal infections produce double refracting systems that cause optical distortion and significantly decrease visual acuity (Fig. 100-3).
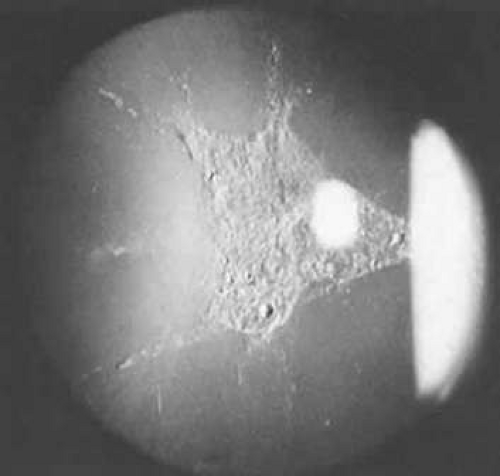 Figure 100-2. A posterior subcapsular cataract that has reduced visual acuity in healthy illumination to 20/60. |
 Figure 100-3. A nuclear cataract present in both eyes of a child with esotropia. The retinoscopy reflex was irregular, and cataract surgery was recommended. Metabolic evaluation and TORCH titer findings were negative. |
Progression
Not all cataracts in children increase in size or density. Premature neonates may have partial opacification (transient neonatal opacities) that may disappear over the first 1 or 2 weeks of life.9 Other cataracts that may regress are those due to galactosemia. These cataracts have the morphologic features of oil droplets. If early dietary restriction of galactose is observed, the opacity may regress.10 Anterior polar cataracts typically remain stable in size and density.
Other types of cataracts characteristically progress in size and density. Cataracts caused by rubella, uveitis, diabetes, exposure to radiation, and use of corticosteroids usually show progression with time.
Visual Acuity and Signs of Visual Function
Ultimately, it is the measured or estimated level of visual acuity or acuity potential that determines the need for cataract surgery. If either the measured or the estimated decrease in visual acuity produced by the cataract is sufficient to prevent adequate visual development or if signs of significantly decreased visual acuity, such as strabismus or poor central fixation, are present, cataract surgery is indicated. Use of the Teller visual acuity cards at periodic intervals can help to measure visual acuity.11 In some children, visual acuity that is below normal or decreasing can be documented accurately to support the decision to perform cataract surgery (Figs. 100-4 and 100-5). Care must be taken in interpreting Teller visual acuity data because the normal levels in young infants and children are low and span a wide range. It is important to note, however, that the Teller acuity card measurement of grating visual acuity may severely underestimate the level of visual loss in patients with cataracts and amblyopia,12 and this limits this usefulness of this measurement.
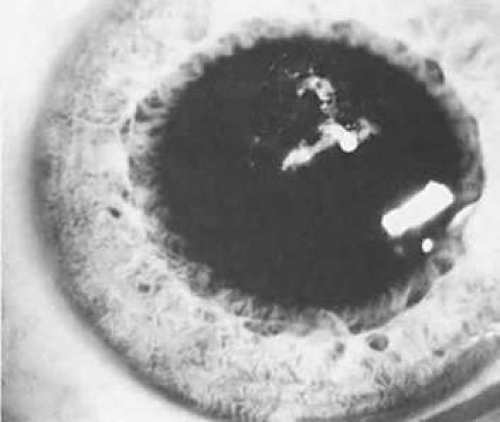 Figure 100-4. Posterior lenticonus type of cataract. When the child was 1 year old, the cataract increased in size, and the posterior portion of the lens became increasingly opaque. Surgery was recommended. |
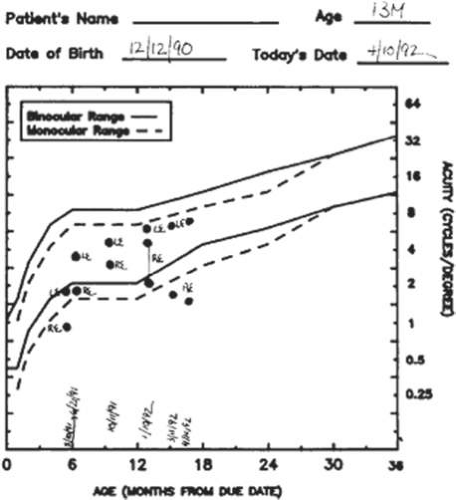 Figure 100-5. Acuity card results. Visual acuity was measured repeatedly in the right eye with the Teller visual acuity cards. The visual acuity decreased despite occlusion of the sound eye, and cataract surgery was recommended. |
Coexisting Ocular Defects
Infants with cataracts may have coexisting defects of the globe or visual system that influence the decision to proceed with cataract surgery. If a cataract exists in an eye with other major structural anomalies and the fellow eye is normal, the visual benefits of proceeding with surgery are negligible, and the child should not be subjected to the risk of anesthesia and perioperative morbidity. If both eyes have major structural defects and complete cataracts, cataract surgery may be indicated to allow the child some opportunity for the development of vision, even if it is limited.
Health of the Child
An assessment of the general health of a child is important when considering cataract surgery because general anesthesia is required for the operation. Premature infants with severe bronchopulmonary dysplasia may have unacceptable risks associated with the use of general anesthesia, and surgery may have to be delayed until the patient can better tolerate the general anesthesia. Other children who have systemic diseases such as galactosemia, homocystinuria, congenital heart disease, and Marfan syndrome or who have experienced trauma have additional risks associated with general anesthesia. For these children, appropriate consultation is needed to assess the risks of the procedure before proceeding with surgery.
Social Situation
Because the success or failure of visual rehabilitation of an infant or young child with a cataract depends on postoperative care, acceptance of optical correction, and compliance with occlusion therapy, the capabilities of the family unit and its support structures must be considered. For example, if one parent has bilateral familial cataracts and poor vision and the other parent also has a visual impairment, delivery of postoperative care may be problematic. If the delivery of adequate postoperative care is likely to be a problem, cataract surgery must be considered carefully because the risk for amblyopia and visual loss produced by uncorrected aphakic refractive errors or even pseudophakia may outweigh the amblyopia and visual loss produced by a partial cataract.
CONTRAINDICATIONS TO SURGERY
There are few contraindications for performing cataract surgery in children. If a severe life-limiting disease, such as Lowe syndrome or Edward syndrome, is present, cataract surgery should be deferred. Surgery is contraindicated in cases of severe microphthalmia (corneal diameter <5 mm) and in eyes in which the retina is irreparably detached or the posterior segment is disorganized (Fig. 100-6). Because of the risk of extraocular spread of tumor, another contraindication is the presence of untreated retinoblastoma. Surgery is not contraindicated in eyes with successfully treated tumors.13
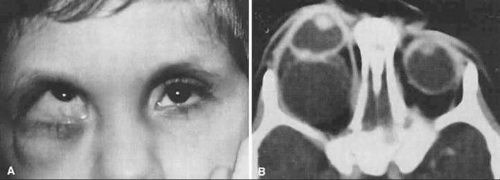 Figure 100-6. A. A 2-year-old boy who has microphthalmia with a cyst on the right side and a dense lens opacity. B. CT scan shows a large cyst that communicates with the vitreous. This finding was confirmed with B-scan ultrasonography. Cataract surgery was not performed. |
Until three decades ago, it was widely believed that the prognosis for visual rehabilitation of any child with a unilateral congenital cataract was poor.14,15 Frey et al16 re-evaluated the treatment of children with monocular cataracts. They were encouraged when three children who had congenital monocular cataracts had 20/40 or better visual acuity. Some surgeons believe that surgery is not indicated when a monocular cataract is first diagnosed in an adolescent. However, a cataract that is presumed to be congenital or of undetermined onset may not have been visually significant at birth or early in infancy, and some visual development may have occurred. In such cases, visual results after cataract surgery on a visually mature child or adult may be much better than assumed.17 Additionally, cataract surgery should be considered for adults, even when irreversible deprivation amblyopia precludes recovery of central visual acuity. In these situations, the increase in the peripheral visual field on the side of the affected eye may be useful and desirable (Fig. 100-7). An attempt at visual rehabilitation of an eye with a monocular cataract is warranted unless medical contraindications are present, the globe is structurally disorganized, or the risk of complications is high.
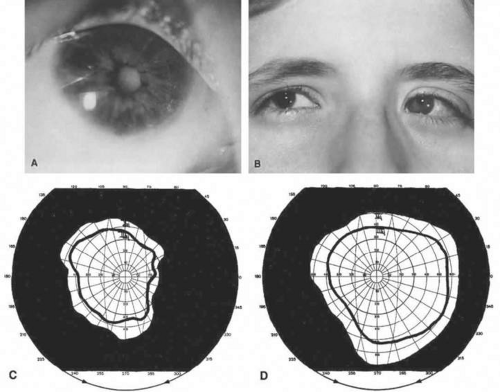 Figure 100-7. A. A 31-year-old patient with bilateral congenital cataracts. The left cataract was removed early in life, but glaucoma and retinal detachment occurred after surgery. B. A complete cataract was removed in the fellow right eye when the patient was 31 years old. The resulting visual acuity was counting fingers at 3 feet, but the patient was pleased with her increased field of binocular vision. C. The visual field before cataract surgery. D. The binocular field of vision after cataract surgery. |
TIMING OF SURGERY
The immature visual system of a young child is sensitive to defects that interrupt the focusing of light on the retina. Studies conducted in animals as well as in humans have identified a critical period in visual development during which the immature visual system must be stimulated with focused images on the retina to permit normal visual development.18,19 If this stimulation does not occur, profound amblyopia develops. When early treatment of a cataract is followed by accurate optical correction and occlusion therapy, stimulation of the retina occurs during the critical period, and a complete reversal of deprivation amblyopia is possible. Conversely, if treatment of a complete cataract is delayed beyond the critical period, complete reversal of the amblyopia may not be possible.
In infants who have complete unilateral congenital cataracts, the critical period for visual development ends at around 17 weeks.2 Therefore, the length of the critical period removes infantile cataract surgery from the category of emergency surgery. However, amblyopia is more amenable to treatment when treatment begins as early as possible.1 An extension of this rationale applies when monocular partial cataracts occur after birth. In these patients, the amblyopia is reversed more easily and completely when treatment begins as soon as possible after the onset of visual deprivation. Therefore, we can assume the existence of similar critical periods in visual development related to visual deprivation, either complete or partial, with an onset not at birth but later during the course of visual development. These periods may be much longer or less rigid because at least some stimulation and development of the visual system occurred. In children who are susceptible to amblyopia, cataract surgery should be performed soon after a visually significant lens opacity is identified.
A critical period for complete reversal of deprivation amblyopia caused by complete bilateral congenital cataracts also exists. Surgery must be performed before the patient is 2 to 3 months old. After this time, the onset of nystagmus owing to sensory deprivation occurs.20 Once this form of nystagmus develops, obtaining visual acuity better than 20/50 is unlikely. Birch et al3 have demonstrated that earlier surgery performed on patients between birth and 14 months of age is associated with improved visual acuity and less amblyopia and that visual acuity when surgery is performed between 14 and 31 weeks of age is independent of age at surgery for these older children with a mean visual acuity of 20/80. Young children with bilateral cataracts should undergo surgery on the eye with the most opaque lens as early in life as safety permits. After surgery has been performed and no untoward effects have been identified, the fellow eye can be treated.
In adolescent patients who have bilateral partial cataracts, surgery may be indicated for the eye with the worst vision to enhance distance visual acuity. If the near visual acuity in the second eye is acceptable, surgery may be delayed for this eye. This treatment plan allows the patient to have the benefit of accommodation and also may allow the patient to take advantage of future advances in surgical techniques or developments in intraocular lens (IOL) technology if the lens opacity increases.
OPTICAL REHABILITATION
After a decision to perform surgery has been made, it is necessary to decide on the type of aphakic optical correction that will be used. For a child, the ideal optical correction for aphakia should be safe and provide a constant, undistorted focused image on the fovea. This correction should remain effective with growth of the eye, should have optical power and magnification effects similar to those of the natural lens of the fellow eye, and should provide accommodation. Finally, it should provide protection from ultraviolet light and be long lasting and cost-effective.
Available measures for optical correction of aphakia include glasses, contact lenses, and IOL implants. Epikeratoplasty, once used for the optical correction of pediatric aphakia, is essentially no longer performed. All of these forms of aphakic correction have advantages as well as limitations. The decision as to which method of correction is best for any particular patient must be made on a case-by-case basis. Consideration should be given to whether the patient is affected by monocular or binocular cataracts, both now and in the foreseeable future; the patient’s age; and the family or social situation. The optical problems of anisometropia and aniseikonia and concerns for safety and complications with the use of bilateral intraocular lens implants also dictate the choice of optical correction (Tables 100-1 and 100-2).
 |
 |
Aphakic spectacles with bifocals are used principally to correct binocular aphakia in patients who are unable to tolerate contact lenses. In infants and young children, there are difficulties with fitting thick aphakic glasses, and these glasses have optical disadvantages when compared with contact lenses. Patients with monocular cataracts are better rehabilitated with a contact lens or an IOL, avoiding the aniseikonia that a monocular aphakic eyeglass lens would produce.
Contact lenses had previously been the mainstay of treatment of either unilateral or bilateral aphakia in children. Developing confidence in the feasibility and safety of IOL implantation has led to a more widespread use of IOLs in children in recent years; however, contact lenses remain the optical rehabilitation method of choice in infants younger than 1 year of age because of their excellent optical properties, safety, and ability to be changed in power with the changing needs of the growing infant eye. Although the use of contact lenses in older children is being supplanted by IOL implantation, contact lenses remain a viable alternative to IOLs in all patients and are indicated when contraindications to IOL use are present, such as chronic inflammatory disease and some cases of glaucoma. Silicone soft contact lenses and rigid gas-permeable contact lenses are available in powers high enough for the correction of aphakia in the small infant eye, and each type of lens has its advantages and disadvantages.21 Silicone lenses can be worn on an extended-wear schedule with removal of lenses only every several weeks for cleaning or, preferably, they may be worn on a daily wear schedule. These lenses are, unfortunately, available only in a limited number of fit and power parameters, and compromises must be made in many patients. Eyes of young infants and especially microphthalmic eyes may have very steep corneal curvatures requiring contact lens base curves of >50.00 D and powers of >30.00 D. Rigid gas-permeable lenses are readily available in custom designs for fit and power, are relatively lower in cost, and with their smaller diameter may be easier for parents to insert and remove. Rigid gas-permeable lenses neutralize astigmatism better than soft contact lenses. Although naps and an occasional night with rigid gas-permeable lenses in place are acceptable, a daily wear schedule is recommended with this type of lens.
Patients with dry eyes, lid abnormalities, or irregular or scarred corneas are poor candidates for contact lenses, as are children with large-amplitude nystagmus. Extensive family commitment is required for the insertion, removal, and care of contact lenses, and lost or damaged lenses are an ongoing financial responsibility. Contact lens intolerance seldom occurs in infants younger than 1 year of age if the parents are motivated and well instructed in the care of the lenses. Some children are, however, psychologically and physically resistant to the insertion, wear, and removal of lenses, either on their initial use or sometimes after an extended period of successful wear. Delayed intolerance of contact lenses occurs most frequently when a child reaches the age of 18 to 36 months and begins to assert more independence. If the family can be motivated to continue over a period of several difficult months, the child frequently gives up fighting over the lenses. Children between the ages of 2 and 5 years are perhaps the most difficult to start using contact lenses, especially traumatic cataract patients, and primary IOL implantation should strongly be considered for these patients. Predicting which children and families will be poorly suited to contact lens wear is difficult, and even the most experienced practitioners and contact lens technicians frequently are surprised by contact lens successes in the seemingly most difficult and resistant of children, provided that the physician, technical help, and parents are motivated for the effort required.
The first contact lens is placed on the eye between 1 and 2 weeks after surgery. The fit of the first lens is determined either from keratometry measurements or from a trial lens fit obtained before surgery. The power of the first lens is determined from the spherical equivalent refraction between 3 and 7 days after surgery. An adjustment in the lens is almost inevitable in the immediate postoperative period, and frequent lens power and fit changes may occur, especially during the first 6 months of life.22 In infants, the power of the contact lens is chosen to produce an overcorrection of -2.50 to -3.00 diopters (D) spherical equivalent to allow clear vision in the near range. When distance acuity becomes of greater importance and growth of the face allows the wear of glasses incorporating a bifocal, around 18 months to 2 years, the contact lens power is then chosen to produce a spherical equivalent overcorrection equal to whatever eyeglass lens may be required for the fellow eye. A bifocal of +2.50 to +3.00 D is then prescribed.
IOL implants provide immediate, constant, high-quality, no-maintenance optical correction of similar magnification to the natural lens. These are all important advantages in children in whom visual rehabilitation and development are influenced by the pediatric issues of amblyopia, development of binocular function, compliance, convenience, and the need for familial care. Although the first implantation of an IOL in a child was performed more than 50 years ago, only over the past 15 years has IOL use in children approached common practice. IOLs are becoming the preferred means of optically correcting older children.23 Questions, however, remain that are not yet fully answered concerning growth of the eye, power considerations, potential complications, and long-term safety. For economic and legal reasons, the use of IOL implants in patients younger than 18 years of age is not approved by the United States Food and Drug Administration. Nevertheless, with continued investigation and experience, the minimum age at which IOL implantation is recommended and recommendations for bilateral implantation continue to evolve, making IOL use in children more common. IOL implants are an essential option for many, and probably most, pediatric patients older than 1 to 2 years of age.
PREOPERATIVE MEASURES AND PREVENTION OF COMPLICATIONS
EVALUATION
Because children with congenital or developmental cataracts frequently have associated ocular defects as well as physical abnormalities, a comprehensive physical evaluation should be performed along with a complete assessment of the eye and function of the visual system (pupillary responses and visual acuity or behavior). In some infants and children who are not cooperative during a thorough office examination, added information can be obtained by examination of the eyes while the patient is under anesthesia.
Microphthalmia contributes to increased technical difficulty with surgery and limits the forms of optical correction that can be used. Microcornea has been reported as a risk factor for the development of aphakic glaucoma, 45 (94%) of 48 eyes in one series.24 All children undergoing cataract surgery should have their corneal diameters recorded as rapidly increasing corneal diameter is one of the markers for glaucoma. The presence of iris abnormalities, posterior synechiae, and pupillary membrane remnants may alter the placement of the surgical incision or necessitate the placement of additional corneal incisions to lyse adhesions or to place iris hooks or retractors.
When possible, the intraocular pressure (IOP) should be measured in the office. If measurement in the office is not feasible, it should be done in the operating room with the patient under anesthesia with a Perkins handheld tonometer, Tono-Pen, or Schiotz tonometer. IOP should be measured as soon as the child has been anesthetized so that manipulation of the globe does not cause an inaccurately low reading. If glaucoma is suspected, gonioscopy is performed with a three-mirror pediatric contact lens and the surgical microscope or a Koeppe lens and a Barkan handheld illuminator.
If the IOP is >35 mm Hg before surgery, topically applied beta-blocking eyedrops, oral or intravenous carbonic anhydrase inhibitors (acetazolamide, 5 to 10 mg/kg), or intravenous mannitol (250 mg/kg intravenous push) should be used before the surgical incision is made. This treatment reduces the risk of expulsive choroidal hemorrhage. In eyes with opaque media, ultrasonography should be performed to determine the status of the posterior structures of the globe and to exclude the presence of an intraocular mass.
OPTICAL PROPERTIES OF THE EYE
Before surgery, keratometry and axial length measurements are recorded to fit a contact lens postoperatively or calculate the power of an IOL. In uncooperative children, these measurements are made in the operating room with the patient under general anesthesia. The central corneal curvature is measured with a handheld or microscope-mounted keratometer. If this equipment is not available, a standard keratometer can be used with the child’s head stabilized in the lateral decubitus position. Contact lenses also can be fit in patients with a trial contact lens set, fluorescein dye, and a cobalt blue light25 (Table 100-3 and Fig. 100-8).
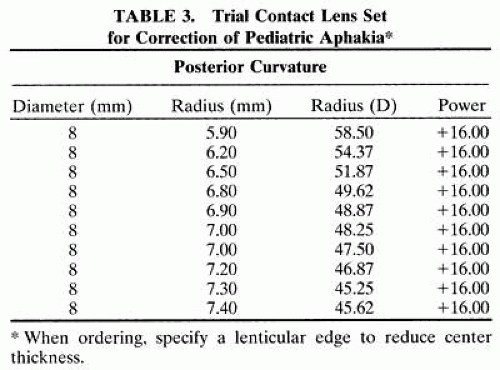 |
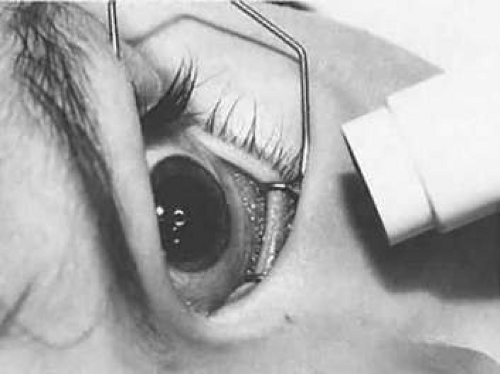 Figure 100-8. The fit of a trial contact lens is being checked with fluorescein and a cobalt blue light. The presence of an air bubble between the lens apex and the cornea indicates that the contact lens is too steep. |
PUPIL DILATION
Pupil dilation of 5 mm or more facilitates cataract surgery. When attempting to achieve maximum pupil dilation, care must be taken not to overdose infants younger than 1 year with strong concentrations of anticholinergic eyedrops, such as 2% cyclopentolate. Concentrations of 10% phenylephrine should not be used because it can elevate blood pressure, increase myocardial irritability, and potentiate the effects of atropine used during the anesthetic induction.
For infants younger than 6 months who have little iris pigment, the recommended mydriatic dosage is 1 drop of Cyclomydril (cyclopentolate 0.2% and phenylephrine 1%) repeated two or three times 30 minutes before surgery. In older children and in infants with particularly dark irides, 2.5% phenylephrine and 1% tropicamide or 2% cyclopentolate is used. If the dilation is not adequate, these drops are reinforced by instilling one or two additional dilating drops after intubation of the airway is accomplished. To maintain mydriasis during the procedure, 1 ampule (1 mL) of preservative-free epinephrine 1:1,000 can be added to a 500-mL bottle of irrigation solution (BSS Plus).
Failure of a pupil to dilate fully is common because of the presence of synechiae (Fig. 100-9) or relatively atonic pupillary dilator muscles (young infants, rubella, and Marfan syndrome). If the pupil is small or synechiae are noted, the location of the incision can be adjusted or a paracentesis tract or tracts can be placed to allow iris manipulation with instruments or the insertion of iris retracting hooks(Figs. 100-10, and 100-11). If the pupil remains small, a sphincterotomy may be necessary. This procedure can be accomplished by cutting the iris sphincter with the anterior vitrectomy handpiece, intraocular or iris scissors.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


