Nonneoplastic diseases of the ear are more common than the actual neoplasia; however, they are infrequently sampled and thus seldom seen by pathologists. While the infectious lesions are by far the most frequent of the nonneoplastic conditions, it is most important that pathologists recognize the lesions of the ear that form masses and mimic neoplasms. Some of these disease processes are specific to the ear, such as chondrodermatitis nodularis chronica helicis.
Congenital Abnormalities and Choristomas
Congenital abnormalities of the ear usually present in childhood.
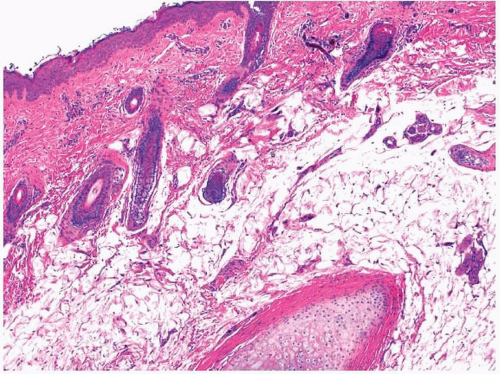
Accessory tragi arise from remnants of the first branchial cleft.
1 These pedunculated lesions are typically less than 1 cm in size and most often are located just anterior to the true tragus. The lesions are either solitary or multiple and are sometimes bilateral. While they are generally not associated with other congenital abnormalities, some patients are also found to have midline abnormalities such as cleft lip or palate. Histologically, accessory tragi have all the components of the normal external ear. They are covered by a stratified squamous epithelium and the underlying dermis
is replete with appendages (
Fig. 16.1, e-
Fig. 16.1).
1 The stroma contains fibroadipose tissue and mature hyaline cartilage.
Other anomalies of the first branchial cleft include
cysts, sinuses, and
fistulas.2 Each usually occurs anterior to the tragus, similar to an accessory tragus; however, their locations vary much more widely. Indeed, these lesions frequently involve the parotid gland and can be confused clinically with parotid tumors. Sinuses and fistulas often drain into the external ear canal or even into the middle ear. First branchial cleft cysts, sinuses, or fistulas are akin to other branchial cleft abnormalities and are lined by ciliated columnar or stratified squamous epithelium surrounded by adnexal structures and lymphoid tissue.
2 Unlike other branchial cleft abnormalities, first branchial cleft cysts sometimes contain cartilage. These remnants are frequently infected at the time of their discovery and the epithelium is sometimes denuded or necrotic; abundant acute inflammation will then be present.
Both
glial and
salivary gland choristomas are found in the middle ear.
3,4,5,6,7,8 and
9 It has been noted by some that true glial choristomas may actually be very rare at these sites and that most reported glial choristomas actually represent either encephaloceles or extruded brain tissue presenting as a middle ear lesion after other local disease processes such as cholesteatomas have led to the destruction of intervening temporal bone.
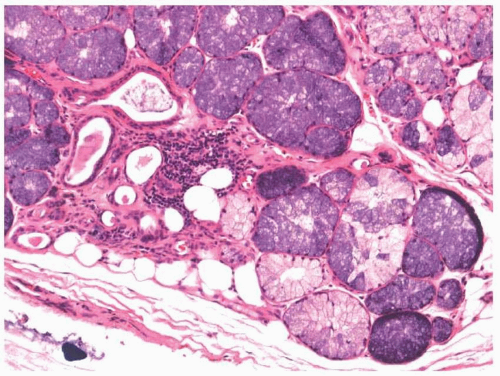
3 Choristomas present in the middle ear behind an intact tympanic membrane and are histologically composed of either glial tissue or salivary gland tissue. The glial choristomas are predominantly composed of astrocytes and neurofibrils.
3,8 Salivary gland choristomas have a mixture
of mucinous and serous glands with ducts (
Fig. 16.2).
6,7,9 Some amount of adipose tissue is often noted.
Congenital cholesteatomas resemble their acquired counterparts described below.
10,11,12,13 and
14 They present in patients who are younger than those presenting with acquired cholesteatomas and are much less common, representing less than 5% of cholesteatomas. An intact tympanic membrane is usually but not universally present. The lesions are discovered incidentally either during otologic examination or because of unilateral hearing loss. Some believe that these lesions develop from epidermoid remnants found in the middle ear. Regardless, they are histologically identical to acquired cholesteatomas and samples are composed of fragments of stratified squamous epithelium and keratin. A foreign body reaction is sometimes seen.
Infectious Disease
Infections of the external and the middle ear are relatively common, but histologic sampling is rarely performed. They can be caused by a variety of organisms including viruses, bacteria, and fungi. Most disease is selflimited, although severe life-threatening infections sometimes develop, especially in immunocompromised patients.
Abscesses or
furuncles of the external ear are usually associated with sebaceous glands and hair follicles and thus present within the auricle or outer canal.
15,16 These are red, inflamed nodules that may be exquisitely painful. Although they are most often secondary to infection due to
Staphylococcus aureus, a number of bacteria can be linked etiologically
to these pustules. Histologically, pockets of neutrophils and debris are surrounded by abundant acute and chronic inflammation, typically with some degree of fibrosis and granulomatous inflammation. Involved pilosebaceous units are usually seen.
Otitis externa, both benign and “malignant,” is most often caused by infection due to
Pseudomonas aeruginosa.15,17,18 and
19 Both forms of the disease represent variants of cellulitis. The benign or more common form develops most often in the lateral portion of the external auditory canal and may be secondary to predisposing factors such as local trauma and disruption of the ceruminal barrier. The disease develops most often in tropical climates and in humid weather. Swimming is a risk factor for the development of the disease. The “malignant” or necrotizing form is much more aggressive and typically involves the more medial portion of the external auditory canal. It occurs in older patients, many of whom are immunocompromised secondary to diabetes mellitus. These infections may spread along tissue and fascial planes, along cranial nerves and vessels, and eventually involve the parotid gland, surrounding bone or brain. Thrombophlebitis of the cavernous sinus even develops in some cases. Histologically, the findings correspond to the extent of the infection. Edema and acute and chronic inflammation are seen throughout the involved soft tissue. Ulceration, necrotizing vasculitis, and tissue necrosis are all seen as the process worsens.
As with otitis externa,
otitis media is very unlikely to be sampled. This extremely common disease of childhood presents with ear pain and bulging, erythematous, or exudative tympanic membranes on otologic examination.
20 Recurrent and chronic infections secondary to blockage of the eustachian tubes sometimes lead to complications, including cholesteatoma.
21 Causative agents include bacteria, such as
Streptococcus pneumoniae, Haemophilus influenzae, and
Moraxella catarrhalis, along with various upper respiratory tract viruses.
20 Sampling shows a nonspecific acute and chronic inflammatory infiltrate within the epithelial and stromal tissues. Rarely,
Mycobacterium tuberculosis infects the middle ear and, when sampled, a granulomatous reaction is seen.
22 Finally, it should be noted that otitis media in adults is frequently associated with neoplasia.
Viral infections sometimes involve the external ear and the tympanic membrane (myringitis). The ear canal and the tympanic membrane can be affected by
Varicella zoster (Ramsay-Hunt syndrome) and, oddly,
Herpes simplex virus.19,23 The clinical and pathologic findings are identical to those seen at other sites. The telltale nuclear inclusions within the squamous cells of the vesicles or ulcerated areas should lead one to the correct diagnosis. Occasional hemorrhagic vesicles can be seen on the external tympanic membrane in cases of influenza.
24
Fungi rarely infect the squamous epithelium of the external ear
(otomycoses).15,23,25,26 Most of these infections are caused by
Aspergillus or
Candida species. In general, these infections present as typical cases
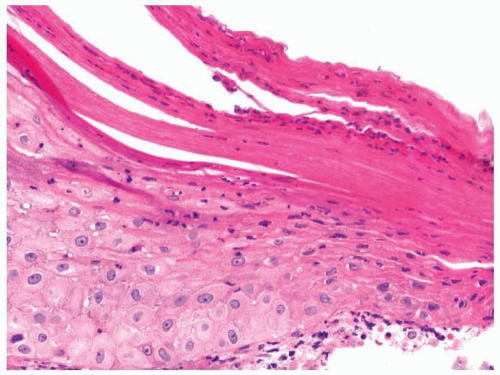
of otitis externa, and it is estimated that 2% of cases of otitis externa are caused by fungi. Histologically, the squamous epithelium is thickened with parakeratosis and focal collections of intraepithelial neutrophils (
Fig. 16.3). Hyphal and yeast forms are then found within the parakeratotic plaques. Subepithelial chronic inflammation is also typically noted. The fungi should not extend into the subepithelial tissues in uncomplicated cases of otomycosis. Deeper infections due to a number of organisms such as
Cryptococcus and
Blastomyces are rare but have been reported.
Inflammatory and Reactive Conditions and Other Abnormalities
The lengthy designation
chondrodermatitis nodularis chronica helicis describes a painful, inflammatory lesion of the external ear.
27,28 and
29 The lesion occurs somewhat more frequently in older men and typically involves the outer portion of the helix, but any portion of the auricle may be involved. It most often presents as a painful, solitary nodule that is less than 1 cm in size. A surface crust is typically seen, and clinicians often believe that the lesions are malignant prior to biopsy. The pathogenesis of the condition is uncertain. Most believe that it arises from localized ischemia related to chronic conditions such as sun damage and repeated pressure-related trauma. This process is benign and is typically cured by limited local resection.
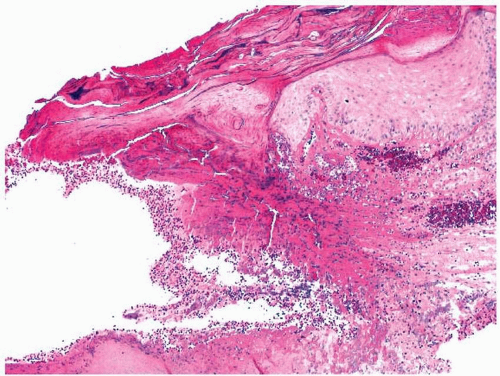
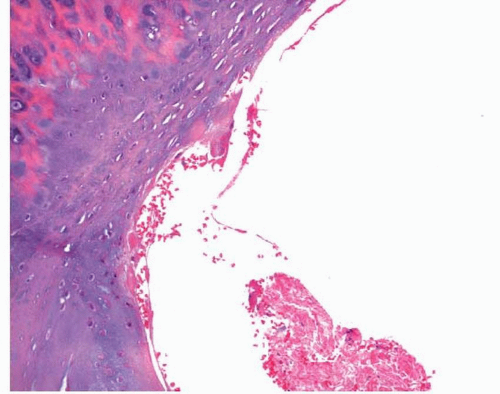
Histologically, the centrally ulcerated and crusted area is surrounded by thickened and parakeratotic squamous epithelium.
27,28 and
29 The fibrinous debris of the ulcer base extends centrally to the perichondrium and auricular cartilage and is surrounded by granulation tissue and acute and chronic inflammation. Some degree of erosion of the cartilage is often seen with
surrounding necrosis and basophilia (
Fig. 16.4, e-
Figs. 16.2 and
16.3). Reactive changes such as stromal cellular atypia and fibrosis can be seen.
Idiopathic cystic chondromalacia, also known as pseudocyst of the auricle, typically presents as a swelling of the auricle in young to middleaged adults.
30,31 Although any portion of the auricle can be involved, the helix is the most commonly affected site. The pathogenesis of these lesions is unknown, but as with chondrodermatitis nodularis chronica helicis, trauma may play some role. Histologically, these are pseudocystic spaces within the auricular cartilage with surrounding normal cartilage, degenerated cartilage, or granulation tissue (
Fig. 16.5, e-
Fig. 16.4).
As was discussed in the chapter describing nonneoplastic disease of the larynx (
Chapter 15),
relapsing polychondritis is a rheumatic disease characterized by episodic and progressive inflammation of cartilage.
32,33 The ears are often affected and the involvement is typically bilateral. Diagnosis requires a combination of clinical and pathologic findings. Histologically, the cartilage will typically appear necrotic or degenerated with surrounding acute and chronic inflammation.
Kimura disease is a chronic inflammatory condition that frequently involves the head and neck region at or just behind the ear.
34,35,36,37 and
38 Patients are more often men, and the disease appears to be much more common in Asian populations. The lesions typically present as painless masses averaging 2.5 cm in size and located deep within the dermis with associated regional lymphadenopathy and parotid involvement. Although the pathogenesis is unknown, patients are frequently noted to have peripheral eosinophilia and elevated serum concentrations of IgE.
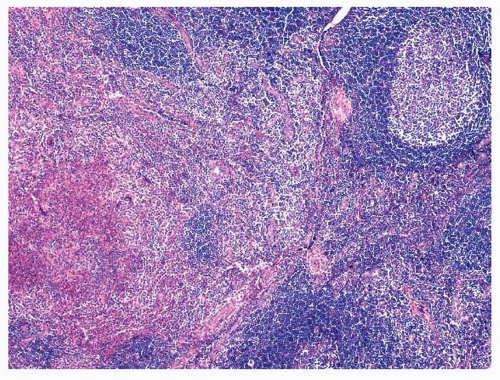
Histologic sections of Kimura disease usually show some degree of residual lymph node architecture, with follicular hyperplasia and wellformed mantle zones (
Fig. 16.6).
34,35,36 and
37 The inflammatory infiltrate most often extends into the perinodal soft tissues, and capsular and stromal fibrosis is typically present. Eosinophilic folliculysis is usually seen with
necrosis and proteinaceous debris noted within the germinal centers. Abundant eosinophils are also present in the interfollicular areas, sinusoids, and perinodal tissue, and these frequently aggregate into small eosinophilic microabscesses (e-
Figs. 16.5 and
16.6). An increased number of vessels are frequently noted, as is a postcapillary venular proliferation. Immunohistochemistry supports the diagnosis of a reactive process and the test for Epstein-Barr virus is usually negative.
Kimura disease should be distinguished from angiolymphoid hyperplasia with eosinophilia (epithelioid/histiocytoid hemangioma), as the two are distinct clinicopathologic entities (
Table 16.1).
34,35,36 and
37 Kimura disease occurs more frequently in Asians and in men, more often is deep in the dermis, and is associated with adenopathy and salivary gland involvement, increased serum IgE levels, and peripheral eosinophilia. Angiolymphoid hyperplasia with eosinophilia occurs equally in all races, is more common in women, presents as a superficial papule, and is not associated with peripheral eosinophilia, increased serum IgE levels, or adenopathy. In Kimura disease, the vascular component is much less prominent than it is in angiolymphoid hyperplasia with eosinophilia, and the endothelial cells are typically flattened rather than epithelioid.
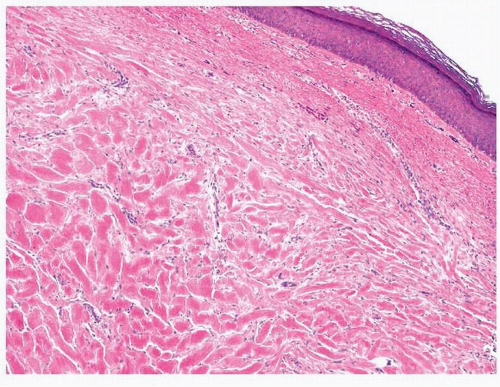
Keloids of the ear resemble those seen throughout the rest of the body, both clinically and pathologically.
39,40 As such, they develop more frequently in African Americans and often arise after local trauma, such as ear piercing. They present as firm, pink nodules, usually covered by an intact epithelium. The histologic features are rather distinct with thick, eosinophilic bands of collagen present throughout the dermal tissue, often obliterating adnexal structures and flattening the surface epithelium (
Fig. 16.7, e-
Fig. 16.7). As such, the lesions appear quite hypocellular and are composed predominantly of collagen with occasional intermixed fibroblasts.
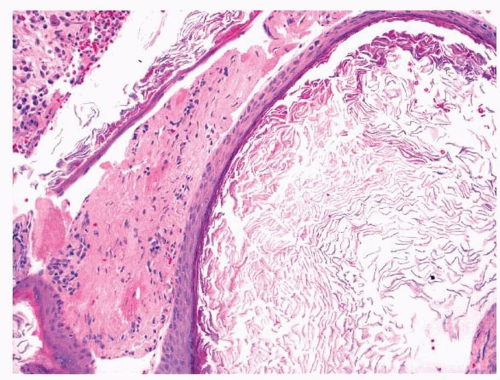
Keratin accumulation in the external ear canal can cause obstruction either secondary to the keratin itself or secondary to the body’s response to the keratin. Some individuals apparently have impaired lateral extrusion of external canal keratin, which then accumulates and plugs the canal
(keratosis obturans).41 The keratin in such cases actually accumulates to such a degree as to widen the canal and cause pressure ulceration of the surrounding epithelium. Secondary infections of the keratin debris are common. The histologic features are as unexciting as one would expect. There is abundant keratinous debris, sometimes with cholesterol clefts, inflammation, and evidence of epithelial ulceration (
Fig. 16.8, e-
Fig. 16.8). Keratinous cysts of the external ear can also cause obstruction. As with the more common middle ear lesions, they are called
cholesteatomas here.
41 Histologically, they are cystic structures, lined by a bland, stratified squamous epithelium. With rupture of these cysts or through ear canal trauma, keratin can come into contact with the stroma and abundant foreign body reaction can be formed
(keratin granulomas).41,42 These further lead to obstruction of the canal and can cause hearing loss and pain.
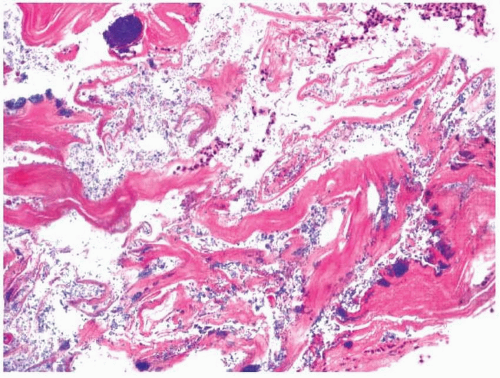
Acquired cholesteatomas of the middle ear are nonneoplastic masses caused by the production of keratin by stratified squamous epithelium.
11,13,29,43,44 Given the small volume of the middle ear, even very small lesions can easily result in clinical problems. Acquired cholesteatomas are distinguished from congenital cholesteatomas through assessment of the tympanic membrane. As acquired cholesteatomas are believed to result from severe otitis media or, rarely, trauma, and entry of squamous epithelium from the external ear into the middle ear, they are typically associated with ruptured tympanic membranes. Clinically, acquired cholesteatomas appear white and pearly. Histologically, they are composed of keratin and stratified squamous epithelium that is sometimes fragmented (
Fig. 16.9). They occasionally present as intact cystic structures (e-
Fig. 16.9). Calcification, inflammation, and foreign body reaction are also commonly present.
Chronic otitis media is sometimes associated with middle ear
cholesterol granulomas.45 These yellow, nodular lesions are believed to be secondary to hemorrhage. Histologically, they are composed of red blood cells, hemosiderin-laden macrophages, cholesterol clefts, and a foreign body reaction. It is important that these lesions are not mislabeled as cholesteatomas, as they are not locally aggressive.
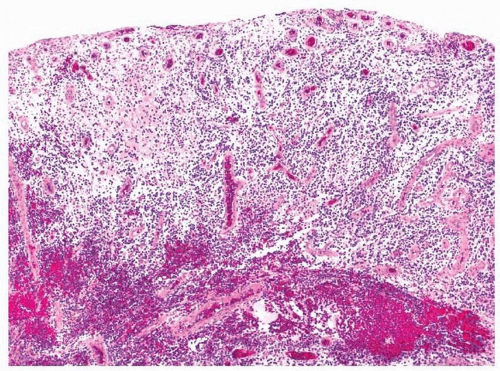
Chronic otitis media is also associated with the formation of an
inflammatory polyp (aural polyp) of the middle ear.
46 These nonneoplastic lesions frequently extend through the tympanic membrane into the external auditory canal. They are polypoid masses of granulation tissue and inflamed stroma (
Fig. 16.10, e-
Fig. 16.10). Edema, fibrosis,
foreign body reaction, hemosiderin-laden macrophages, and cholesterol granulomas all may be present within the body of the polyp. The surface epithelium is often eroded but, if present, is either ciliated columnar or squamous. Inflammatory polyps may be associated with cholesteatomas or neoplasms.
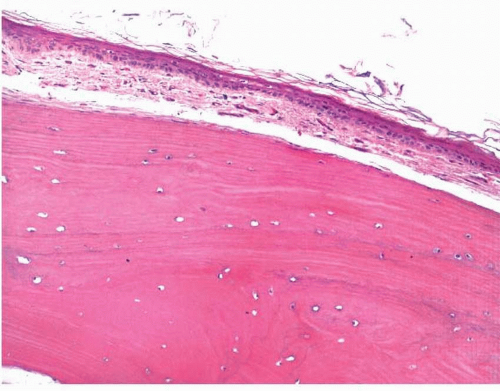
Most masses composed of mature bone within the ear canal are classified as
osteomas or as bony
exostoses.47,48 External ear osteomas are more common in men, occur over a broad age range, and present as solitary, pedunculated bony lesions attached to underlying bone. Bony exostoses are broad-based, often bilateral lesions of the external auditory canal that are also more common in men and often present with obstructive hearing loss. Both lesions are composed of mature, lamellar bone present beneath the intact squamous epithelium of the canal (
Fig. 16.11, e-
Fig. 16.11). Osteomas have been noted to have larger interlamellar spaces. These lesions are difficult to confuse with other entities, although some have noted that lesions such as fibrous dysplasia should be excluded.
Many other inflammatory processes affect various or all portions of the ear. The auricle can be easily traumatized, sometimes chronically such as with the earpieces of glasses
(spectacle frame acanthoma or
granuloma fissuratum).
49 Chronic trauma also sometimes leads to calcification or ossification of the earlobe
(petrified auricle).50 Malakoplakia and
xanthomas51,52 and IgG4-related sclerosing lesions
53 have been reported in the ear. Ulcers secondary to cold and humid weather
(chilblains) have also been reported.
54 Elastic nodules can form on the external ear secondary to severe sun damage.
55 The external auditory canal may exhibit a foreign body reaction to any of the many things that are placed within it and
myospherulosis, akin to that seen in the sinonasal area, has been seen.
56,57 Finally, systemic processes, such as
sarcoidosis and
Wegener’s granulomatosis, sometimes involve portions of the ear.
58