Pathogenesis and Control of Blinding Trachoma
Jaya D. Chidambaram
Chandler R. Dawson
Thomas M. Lietman
Trachoma is a chronic infectious keratoconjunctivitis that is a major cause of blindness in many developing countries. It presents initially as a follicular conjunctivitis, with superficial keratitis and corneal vascularization, and gradually progresses to conjunctival scarring and lid distortion. Damage to the cornea occurs from the chronic inflammatory disease and later from exposure and trauma from the distorted lids and inturned lashes.
Endemic trachoma is still a major cause of blindness in poorer rural communities of developing countries, especially in arid areas.1 Trachoma affects about 600 million people,2 with active infectious disease in 84 million and operable trichiasis in 7.6 million.3 There are an estimated 2.3 million blind from trachoma, and even more have partial loss of vision. Clinical criteria can provide an estimate of the current and future impact of the disease on affected communities and thus the need for intervention. It is also possible to distinguish communities with “blinding trachoma” from communities with “nonblinding trachoma.”
Trachoma is a chronic inflammation of the conjunctiva and cornea that progresses to conjunctival scarring and corneal vascularization. Chlamydia trachomatis is the specific and unique etiologic agent of trachoma, but other pathogenic microorganisms may contribute to the disease process.4,5 In its communicable inflammatory phase, the conjunctiva in trachoma is characterized by the presence of lymphoid germinal centers (lymphoid follicles) surrounded by intense and inflammatory diffuse infiltration (papillary hypertrophy) and by the growth of superficial blood vessels over the superior cornea (vascular pannus).
Trachomatous inflammation may undergo spontaneous resolution or progress to severe conjunctival scarring, which leads to distortion of the lids with trichiasis or entropion, corneal surface defects, and corneal opacity. Thus, trachoma may heal with no permanent damage or in its severe forms produce permanent damage to the cornea. The final visual acuity may range from normal vision to total blindness.1
ETIOLOGY
Chlamydia trachomatis eye infections occur in two distinct epidemiologic settings. The first pattern is the potentially blinding disease of developing countries that is spread by eye-to-eye transmission of infection, defined as endemic trachoma. It is caused invariably by the serotypes A, B, Ba, or C of C. trachomatis.6
The second pattern is infection of the eye by sexually transmitted C. trachomatis strains (usually serotypes D, E, F, G, H, I, J, or K), which produce an eye disease that can be similar to the early inflammatory phases of endemic trachoma. Mild cases are usually called inclusion conjunctivitis, but the term paratrachoma has been used to describe the whole spectrum of disease resulting from eye infections with sexually transmitted C. trachomatis strains. Sexually transmitted C. trachomatis also infects newborns during delivery and can cause conjunctivitis, pneumonia, and gastrointestinal infection. Although the sporadic eye infections associated with sexually transmitted C. trachomatis strains rarely produce permanent visual loss, the respiratory tract infections in infants and genital tract infections in adults are important health problems in affected populations.
The A through K strains of C. trachomatis were formerly referred to collectively as TRIC (TRachoma-Inclusion Conjunctivitis) agents because they share most characteristics, particularly replication limited to columnar epithelium. The lymphogranuloma venereum biovar of C. trachomatis (strains L1, L2, and L3) initially infects the mucosal epithelium but also invades the deeper lymphoid tissues. Lymphogranuloma venereum biovar only rarely involves the eye, where it can cause a Parinaud oculoglandular–like conjunctivitis with diffuse inflammatory conjunctivitis and massive enlargement of the preauricular and submandibular lymph nodes.7 The other chlamydial species (C. psittaci and C. pneumoniae) can also cause chronic follicular conjunctivitis.8
Communities with trachoma often have a high rate of bacterial and viral conjunctivitis, which is closely associated with large populations of eye-seeking flies.5,9,10 These factors may escalate nonblinding trachoma into blinding trachoma.11 Furthermore, in such communities, bacterial corneal ulceration is common and constitutes an acute pathway to blindness.
PATHOLOGY
Conjunctiva
Chlamydial infection in trachoma is limited to the epithelium, but the major inflammatory and cicatricial changes appear in the subepithelial connective tissues. In the inflammatory phase, attachments between conjunctival epithelial cells become loosened, so the epithelial cells are often separated in conjunctival smears rather than in attached cell sheets. The epithelium thickens from three to four cell layers to six or eight layers12 except directly over follicles, where it is considerably thinned.13 The conjunctival epithelial cells become irregular in size and may form multinucleated giant cells.14 The conjunctiva is also infiltrated heavily with lymphocytes and polymorphonuclear leukocytes.
In the subepithelial tissues, there is marked vascular dilation and infiltration of the subepithelial tissue by lymphocytic cells and other inflammatory cells. This infiltration elevates the conjunctiva into flat summits with deep folds of epithelium between to form papilla.12,13 Over the tarsal plates where the conjunctiva is bound down to connective tissue, there is only moderate elevation; in the fornices and at the edge of the upper tarsal plate, rolls of elevated hyperemic tissue develop.
The pathognomonic lesion of trachoma is the lymphoid follicle, which forms in the subepithelial tissue. Small follicles consist only of masses of lymphoid cells.12 In larger follicles, the center consists of large lymphocytic cells, with abundant cytoplasm and a few macrophages. Surrounding this is a zone of small lymphocytes, which may extend to the layer immediately below the basement membrane of the epithelium. The cells in the center of these larger follicles sometimes appear to degenerate; with slight pressure, the contents may be expressed onto the conjunctival surface (mature follicles).13 The center follicles appear clinically avascular, but dilated vessels are often seen at their periphery. These vessels are often friable and bleed easily when large follicles rupture under slight pressure.
Fibrosis in the subconjunctival connective tissue occurs by fibroblast formation from blood vessels and by cicatrization of necrotic follicles.12 This scar formation often forms a network, leaving islands of relatively unscarred conjunctiva that protrude above the depressed scars. Scarring also obliterates the layer of subconjunctival vessels, grossly deranging the normal vascular architecture.
Folds of epithelium between papillae may become trapped between by the scar tissue to form deep pseudoglands or pseudocysts in the new connective tissue. Epithelium is sloughed into these cystic structures, which appear clinically as yellow concretions or subepithelial lesions that discharge their contents onto the conjunctival surface and are referred to clinically as posttrachomatous degeneration.13 The greasy material from these cysts can cause irritation and form calcified concretions, which may abrade the cornea.
The bulbar conjunctiva undergoes similar inflammatory and cicatricial changes but to a lesser extent. Bulbar follicles occur frequently in children with active trachoma. Scarring of the episcleral tissue results in adhesions between the conjunctiva and sclera, so that during surgical procedures involving separating conjunctiva from the sclera, numerous fibrous bands must be cut, with resultant bleeding.
Cornea
Chlamydia trachomatis may infect corneal epithelial cells but to a lesser extent than conjunctiva. The cornea, however, is constantly exposed to the chlamydial infection and to inflammatory mediators from the tears and palpebral conjunctiva. Thus, keratitis in trachoma comprises focal, anterior, infiltrates in the limbal stroma and corneal vascularization, which is more extensive at the upper limbus. The keratitis in trachoma due directly to C. trachomatis infection is limited to the epithelium and anterior stroma. It is likely that infection with other ocular pathogens also contributes to this process.4,14
The epithelium during infectious trachoma becomes edematous with focal collections of polymorphonuclear leukocytes. Near the limbus, inflammatory cells are present in Bowman membrane and superficial stroma, and this inflammation may cause destruction of the corneal stem cells at the limbus.
Superficial vascularization occurs from the vessels of the conjunctival limbus in conjunction with lymphocytic infiltrates. This vascular pannus consists of new vessels and connective tissue and lies between the epithelium and Bowman membrane. In some cases, it appears to replace the Bowman membrane.15
Lymphoid follicles occur in the conjunctival limbus and cause the absorption of the underlying connective tissue. When these limbal follicles regress, they leave circular depressions (Herbert pits) in the scleral overhang at the limbus, so the clear cornea is apparent beneath.15 These follicles can also form in the pannus where it overlies the cornea, so that some patients have a double row of Herbert pits. Epithelium may fill these depressions, so that the surface is smooth, but loss of connective tissue is still apparent on clinical examination.12
In milder cases, the pannus is not extensive and the overlying epithelium is relatively normal. With extensive pannus, however, the surface epithelium can become rough, thickened, and irregular—probably due to replacement of corneal epithelium by conjunctival epithelium after destruction of the corneal stem cells at the limbus. In patients with healed trachoma, the pannus vessels become attenuated and lose their blood column, appearing as ghost vessels.
The lacrimal gland can be infiltrated during active trachoma. There also may be inflammatory involvement of the canaliculus and lacrimal duct by follicles and scar formation, with blockage of tear outflow and subsequent episodes of dacryocystitis.
PATHOGENESIS
Chlamydial Infection
Chlamydia trachomatis cannot be identified in all cases of clinically active trachoma. With the highly sensitive and specific DNA amplification technology (polymerase chain reaction [PCR], ligase chain reaction [LCR]), C. trachomatis is found most frequently in severe-intensity cases (80% positive), less often in moderate cases (60%), but also in clinically inactive cases (15% to 30%).16 A study of extraocular chlamydial infection determined by isolation in cell culture showed that C. trachomatis was present in the nasopharynx or rectum of 15% of young children with active trachoma in Egypt.17 After local or systemic antibiotic treatment, the prevalence of chlamydial eye infection is substantially reduced (2% to 15%), although the clinical signs of trachoma activity continue at high levels (40% to 60%).
Immunology
Immunologic studies of trachoma and other chlamydial infections have had two main goals: (1) understanding the pathology of the disease, and (2) identifying protective mechanisms to develop effective vaccines. Both humoral and cell-mediated immune responses to chlamydiae occur in trachoma, but consensus is that protective immunity to chlamydia is a type 1 helper T-cell–mediated response.18
The antibody response measured by the microimmunofluorescence (micro-IF) test may be to a broad range of C. trachomatis serotypes or limited to the infecting serotype.19,20,21 In one hyperendemic population, 80% of children had IgG antibody to C. trachomatis.19 In most studies of chronic trachoma, serum IgG antibodies are present at the highest titers; when they appear, IgM antibodies indicate recent infection and occur rarely in trachoma cases.22
In human and experimental C. trachomatis infections, the serum antibody appears to have a protective role, but it cannot eliminate the infection. The main immunogenic protein in the chlamydial outer membrane is the major outer membrane protein (MOMP or ompl).23 Antibody to C. trachomatis strains that vary by one amino acid only may lose its ability to neutralize infectivity, however.24 Thus, vaccines based only on a single epitope of MOMP are unlikely to be effective.
Tear antibodies also have been extensively studied. In trachoma, IgG antibody in tears occurs only rarely in the absence of serum antibody; IgA (secretory) antibody is found more often in tears than in serum but almost always with tear IgG antibody.19 Tear antibodies (IgG) reflect trachoma intensity accurately; in one study of endemic trachoma, 80% of severe cases, 31% of moderate cases, and 17% of mild cases had tear antibody, but serum IgG antibody varied from 81% to 88% in all three groups.19 The titers of both serum and tear antibody are highest in severe cases and lowest in those that are mild. Tear antibody also correlates more highly with presence of chlamydia than does serum antibody.19 Thus, tear antibody reflects more closely the intensity of the disease and the presence of chlamydial infection.
Tears from patients with trachoma also have a low molecular weight substance (less than 10,000 Daltons [Da]) that inhibits C. trachomatis growth in tissue culture.25 Other studies showed that this inhibition is probably caused by γ-interferon, which inhibits growth of C. trachomatis in cell culture and speeds recovery from experimental infection in mice.26,27 In primary human conjunctival cell cultures infected with a type B (trachoma) serovar of C. trachomatis, γ-interferon (but not α– or β-interferon) inhibited growth of C. trachomatis; this effect was reversed by adding tryptophan.28
Other studies have shown that a chlamydial vaccine capable of inducing γ-interferon–secreting T cells in mucosal tissue was highly associated with resistance to challenge infection by C. trachomatis.29 Several other studies have also confirmed that resistance to chlamydial infection is mainly attributable to cell-mediated immunity.18 The consensus of studies of human and experimental chlamydial infections is that the protective response is mainly type I helper T-cell response.18,30
Infection of cultured endocervical (genital) epithelial cells by C. trachomatis (serotypes L2, D, and I, and C. psittaci) induces the prolonged secretion of γ-interferon and other proinflammatory cytokines (IL-6, IL-8, GRO alpha, and granulocyte-macrophage colony-stimulating factors).31 In contrast, exposure of these cells to other bacterial cells causes them to have a quick but transient secretion of γ-interferon. The secretory response to chlamydial infection, however, develops more slowly and is sustained as long as chlamydial protein is being synthesized (50 to 100 hours). The mRNA transcripts for inflammatory cytokines (IL1-β, TNF-α, IFN-γ) were found in inflammatory trachoma, but only transcripts for IL1-β were present in scarred trachoma.32 It is probable that this sustained cytokine response causes the chronic conjunctival inflammation in trachoma, the subsequent scarring, and other complications.
Most lymphocytes in conjunctival smears from patients with active trachoma are T lymphocytes (associated with cell-mediated immunity), and there are fewer B cells. Helper, suppressor-cytoxic, and natural killer T cells have been identified in the conjunctival infiltrates. If these smears reflect the cell population in the conjunctiva, the predominant inflammatory response supports the idea that the immunity is predominantly mediated by T-cell mechanisms.
Host Susceptibility
It is likely that susceptibility to infection or tendency to develop scarring in trachoma, intercurrent infections (measles), or other causes of a decreased immune response (e.g., vitamin A deficiency) may increase the susceptibility of individuals to infection. Because trachoma clusters in families, there is the possibility that host genetic factors may also affect susceptibility to chlamydial infection. In Gambia, those with the A*6802 allele of HLA-A28 (class I) have been hypothesized to have more trachomatous scarring.33 Scarring from trachoma in Gambia may also be associated with a polymorphism in the TNF-α genes promoter, independent of the HLA type.34
In Oman, blinding trachoma (trichiasis and corneal opacity) may be associated with HLA-DR16 (a DR2 subtype).35 Blinding trachoma was lower in patients in the HLA-DR53 group. Thus, it appears that there are multiple genetic factors that affect susceptibility to infection and the risk of developing scarring and visual loss in trachoma. It should be noted that in some hyperendemic areas, essentially all adults have evidence of severe scarring, so it is not clear that a genetic predisposition is important epidemiologically.
Associated Bacterial Infections
Laboratory tests for bacteria are very useful in communities with trachoma because they provide information on other causes of conjunctival inflammation. The more important ocular bacterial pathogens include Haemophilus influenza (particularly the H. aegyptius subtype), Streptococcus pneumoniae, Neisseria species, Moraxella species, and Staphylococcus aureus; other pathogens such as Gram-negative rods and beta streptococci are less frequent.4 Bacterial pathogens occur in higher frequency in the eyes of children with trachoma who have a significantly greater inflammatory response (trachoma intensity); however, bacterial pathogens are also present in lower numbers in mild and inactive cases of trachoma.4 Infection with these bacteria may contribute to the overall degree of inflammation and to the apparent persistence of inflammatory signs (follicles and papillary reaction) when the chlamydial infection has been reduced or eliminated by antibiotic treatment.36 Bacterial pathogens are far more likely to be found in the conjunctivae of individuals with trichiasis.37 Inturned lashes may abrade the cornea in these individuals, and bacterial pathogens colonizing the scarred conjunctiva may predispose to the development of corneal ulcers.11 In addition, such colonization has been associated with increased severity of conjunctival scarring in cicatricial trachoma.37
CLINICAL DISEASE, CLASSIFICATION, AND DIAGNOSIS
The onset of trachoma is gradual, and symptoms of active infection are often less apparent than would be expected from the clinical findings. Young children with active trachoma may have photophobia because of the associated keratitis and prefer to stay indoors. Patients with trichiasis and entropion, however, experience constant pain and discomfort from the inturned lashes that abrade the cornea. These corneal abrasions can become infected with bacterial or fungal pathogens, resulting in corneal ulceration. Corneal ulcers can produce severe pain and marked photophobia.
In the early stages, trachoma presents as a follicular conjunctivitis (Fig. 1), with papillary hypertrophy and diffuse inflammatory infiltration involving the whole conjunctiva, including the upper tarsal conjunctiva (Fig. 2).1 As trachoma progresses, cicatrization of the conjunctiva appears as fine linear and small stellate scars in mild cases and as broader confluent deep scars in severe cases (Figs. 3 and 4).
 Fig. 1. Early trachoma in a preschool child. The conjunctiva of the everted upper lid margin has numerous lymphoid follicles, which appear as small elevated avascular lesions in the midst of the tarsal conjunctiva (TF; Table 3). |
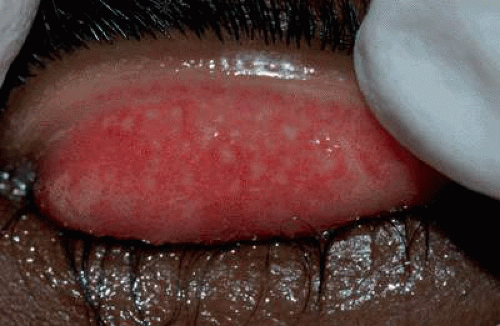 Fig. 2. Severe active trachoma, with marked inflammatory infiltration of the conjunctiva. The lymphoid follicles are visible but partially covered by the infiltrated conjunctiva (F3, P3 or TF, TI; Table 4). |
 Fig. 3. Active trachoma in an Ethiopian child with conjunctival scarring. The small round avascular follicles and diffuse conjunctival inflammation indicates on-going disease activity (F2, P2 or TF, TI; Tables 1 and 4). Conjunctival scars often develop as stellate bands of fibrosis bridging resolving follicles. These scars continue to contract throughout life, eventually leading to entropion and trichiasis.
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|