OVERVIEW
- Chronic rhinosinusitis with or without polyposis is diagnosed by considering the history and examining the nose with a nasendoscope
- Coronal CT scanning is the imaging investigation of choice for rhinosinusitis particularly where surgical treatment is being considered
- Medical therapy for chronic rhinosinusitis with or without polyposis normally includes nasal douching with intra-nasal steroids for longer term maintenance therapy and the intermittent use of systemic steroids and macrolide antibiotics regimes
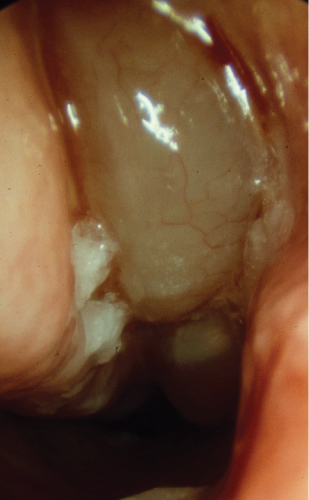
- Nasal polyposis is usually bilateral, unilateral polyposis may indicate a neoplasm rather than benign polyposis
- FESS surgery is the surgical approach of choice for treatment of refractory chronic rhinosinusitis
Anatomy and physiology
The paranasal sinuses are air spaces within the bony facial skeleton with ventilation and drainage channels communicating with cleft-like spaces within the lateral wall of the nasal cavity (Figure 11.1). At birth, the ethmoidal sinuses are relatively well developed with 2–3 cells evident, the maxillary sinuses reach full size after the eruption of the secondary dentition, the frontal sinuses increase in development from 8 years old and the sphenoid sinuses develops from 3 years of age. All the paranasal sinuses continue to develop until the age of 18–20 years. About 5% of patients may not develop frontal sinuses as a normal variation.
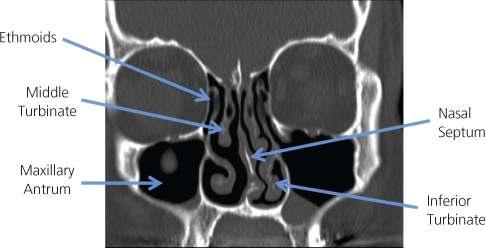
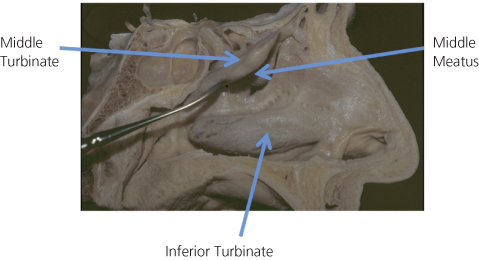
The paranasal sinuses drain into cleft-like air spaces within the lateral wall of the nasal cavity. These lie beneath and lateral to the middle turbinate and the superior turbinate and are known as middle and superior meati. The normal mucus produced by the mucosal lining of the nose and paranasal sinuses is transported through the meati to the posterior aspect of the nose and nasopharynx; this is an active process controlled by the mucociliary system, which is an integral part of the respiratory mucosa lining the nose and paranasal sinuses. The maxillary antra, frontal sinuses and anterior ethmoidal sinuses drain into the middle meatal region and the posterior ethmoid and sphenoid sinuses drain into the superior meatus and spheno-ethmoidal recess region (Figure 11.2). The naso-lacrimal duct drains the lacrimal sac into the inferior meatus anteriorly.
The exact function of the paranasal sinuses is unclear, however, these air spaces allow expansion of the facial skeleton to produce our recognisable facial features and may also act as a ‘crumple zone’ for facial trauma, so that the cranial cavity is adequately protected.
The osteomeatal complex (OMC) is an area comprising the middle turbinate medially and the mucosal-lined clefts and recesses of the maxillary antrum laterally. This is a critical area which must remain clear to allow adequate drainage of mucus from the maxillary antrum, anterior ethmoids and frontal sinuses. OMC obstruction, due to mucosal oedema, causes drainage obstruction from the sinuses, subsequently producing mucosal stasis and infection with acute and subsequent chronic rhinosinusitis.
The mucociliary mechanism within the paranasal sinuses and nasal cavity is of considerable importance to the health of the paranasal sinuses. It includes the pseudostratified ciliated mucosal lining—respiratory mucosa—with the overlying mucus, which is secreted by the seromucinous glands and mucosal goblet cells within the mucosa. The mucus forms two layers, a gel layer (viscous mucus blanket) which overlies a sol layer (thin mucus, bathing the cilia) and which allows movement of the viscous blanket of mucus through the sinuses into the lateral nasal wall clefts and subsequently into the nose and nasopharynx. The mucociliary system produces pathways within the paranasal sinuses and nasal cavities which are genetically predetermined and cannot be rerouted, thus allowing pathways of mucus to flow through the paranasal sinuses and nose. It is this mucociliary mechanism that fails in cystic fibrosis (due to excessive mucus viscosity), and in primary ciliary dyskinetic disorders (ciliary dysmotility), for example Young’s syndrome. The mucus blanket may also become static due to acute infections, allergy, drugs and temporarily after nasal/sinus surgery. Subsequent stasis of the mucus blanket predisposes to acute and chronic rhinosinusitis.
Nose and paranasal sinus examination
Anterior rhinoscopy: This is (Figure 11.3) normally undertaken with a nasal speculum and allows a view of the anterior third of the nasal cavity. However, only a relatively limited view of the lateral nasal wall is possible. In children this can be achieved by pushing the nasal tip upwards to reveal the anterior nasal cavity.
Posterior rhinoscopy: This is achieved using a post-nasal mirror in conjunction with depression of the tongue. This provides a limited view of the nasopharynx and posterior aspect of the nasal cavity.
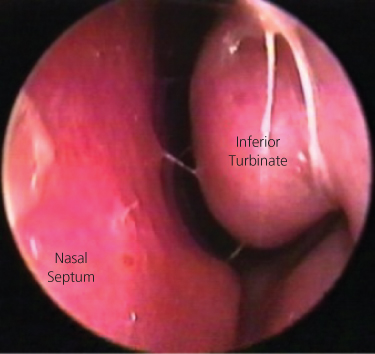
Nasendoscopy: This is performed with a narrow (2–4 mm diameter) rigid or flexible endoscope with or without surface anaesthesia/decongestion as a nasal spray and provides an excellent view of all the nasal cavity and the nasopharynx (Figure 11.4).
Sinoscopy: This is achieved by direct access to the specific sinus by puncture into the sinus cavity with a trocar and cannula and then subsequent insertion of a rigid endoscope, either with local or general anaesthesia and provides a full view of the specific sinus, usually the maxillary antrum.
Rhinosinusitis
Patients with rhinitic or sinusitic conditions normally would have similar mucosal changes within the nose and paranasal sinuses, hence the use of the term rhinosinusitis. There can be a dominance of symptoms arising from the nose or from the paranasal sinuses.
Symptoms and definitions of rhinosinusitis
Rhinosinusitis is considered an inflammation of the nose and paranasal sinus mucosa where two or more symptoms are evident. The main symptoms include nasal blockage or congestion and anterior or posterior nasal discharge; and facial pain or pressure, reduction or loss of sense of smell. Further symptoms which may be evident are sneezing, watery rhinorrhoea, nasal/palatal itch and eye irritation. Symptoms which resolve within 12 weeks can be regarded as acute and symptoms which are present for more than 12 weeks can be regarded as chronic.
Aetiology of rhinosinusitis
Allergy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


