11

Palatal Myoclonus
Palatal myoclonus (PM) refers to the involuntary rhythmic muscular contraction of the soft palate. It was categorized as palatal tremor at the First International Congress of Movement Disorders in 1990, though the terms are often used interchangeably in the literature.1 Palatal tremor (PT) is subclassified into symptomatic palatal tremor (SPT) and essential palatal tremor (EPT). SPT is typically one facet of a complement of symptoms involving the head, neck, and face. SPT is infrequently symptomatic at the level of the palate, and rarely requires medical treatment. EPT, however, generates a symptomatic ear clicking from the inappropriate palate contractions. The end-organ difference between SPT and EPT is thought to be the reason for the variance of symptoms: SPT is posited to involve the levator veli palatini (cranial nerves IX and X), whereas EPT is presumed to involve the tensor veli palatini (cranial nerve V) (Fig. 11.1; Table 11.1). Contraction of the tensor is associated with the rapid opening of the eustachian tube, creating a sudden drop in tubal surface tension resulting in the audible snap, crack, or pop as often described2 (Fig. 11.2). Palatal tremor may involve one or both sides of the soft palate, oscillating at a frequency of 0.5 to 300 Hz. The typical age for EPT is 25 years compared with 45 years for patients with SPT.3 Despite the subclassification of palatal tremor into SPT and EPT, there is evidence supporting a spectrum of palatal tremor disorders, as some patients do not clearly fit into one subclass or the other.1
 Diagnosis
Diagnosis
Diagnosis of palatal myoclonus relies on the history and a neuro-otorhinolaryngologic evaluation. The most common complaint is the characteristic clicking tinnitus, which may be audible to the examiner. When the tremor is symptomatic (i.e., essential palatal tremor), imaging and laboratory evaluations are usually normal. Despite the paucity of diagnostic findings, neurologic assessment is often indicated to define or exclude any associated or underlying abnormality. Symptomatic palatal tremor is usually devoid of any palate-specific symptoms, though it is associated with other neurologic movement disorders of the head and neck. These associated movements may include the larynx, pharynx, face, or other structures controlled by the brainstem or cerebellum. SPT is often synchronous with the extrapalatal myoclonic structures.3 Symptomatic palatal tremor warrants a full neurologic evaluation.
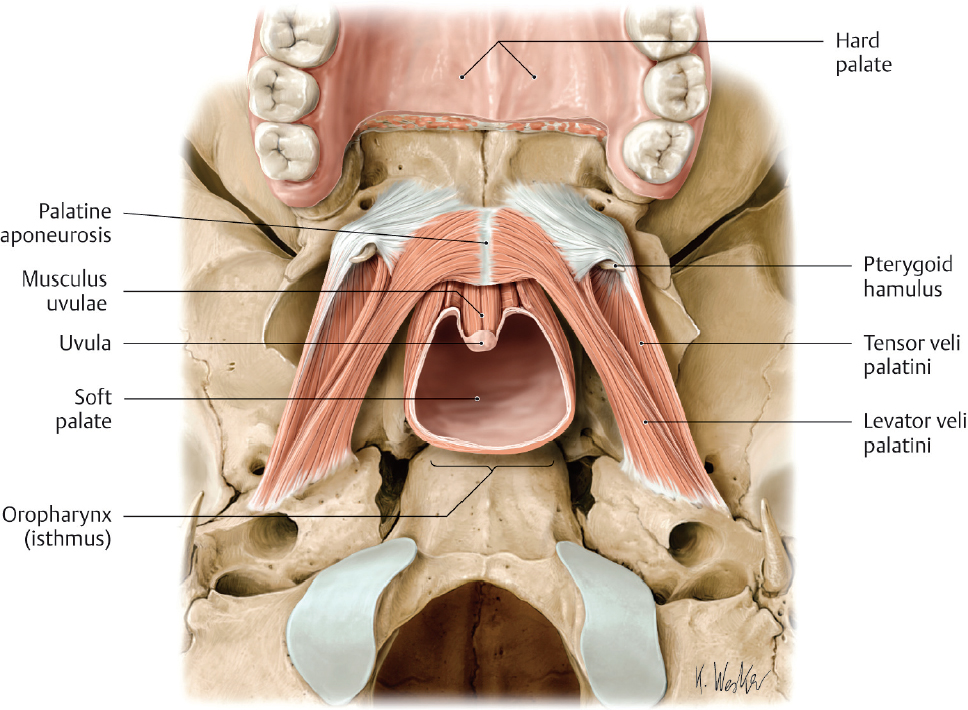
Fig. 11.1 Muscles of the soft palate. (From Atlas of Anatomy, © Thieme 2008, Illustration by Karl Wesker.)
Etiology of SPT may be identified as imaging changes in the inferior olive or dentato-olivary tract. SPT has been associated with numerous systemic metabolic, immunologic, infectious, and traumatic disorders (Table 11.2). There is no clear etiology of EPT, although there are rare reports of imaging abnormalities involving the inferior olive.4
 Treatment
Treatment
Treatment of palatal myoclonus with botulinum neurotoxin (BoNT) is based on the role of the tensor veli palatini as the source of the symptomatic clicking. Thus, despite the underlying subclassification of the palatal tremor, treatment should initially target the tensor when remediating the clicking tinnitus is the goal of therapy. In the United States, onabotulinumtoxinA is the most widely used formulation of BoNT/A. Typical treatment consists of one or two injection sites per side of the soft palate, placing 2.5 units (U) per injection site for an initial dose of 2.5 to 5 U per side. Reported dose ranges can vary from 2.5 to 15 U of BoNT/A per side of the palate.5–8
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


