OVERVIEW
- Pain in the ear arises from ear disease, but also from non-aural disorders
- Diagnosis and management depend on skilled, experienced examination
- Other causes are only by exclusion of ear abnormalities, with reliable recognition of normality
- Referral for specialist opinion is essential whenever:
- there is difficulty in seeing the entire meatus and tympanic membrane, or any doubt about significance of findings
- there is suspicion of complications
- there is difficulty in seeing the entire meatus and tympanic membrane, or any doubt about significance of findings
- Operative intervention may be needed to confirm a diagnosis, or for treatment
- Possible complications must be suspected and treated urgently
Pain (otalgia, earache) is one of six symptoms that suggest ear disease (Box 2.1), these are: pain, discharge, hearing loss, tinnitus, facial weakness and vertigo.
- Pain (otalgia)
- Discharge
- Hearing loss
- Tinnitus
- Vertigo
- Facial palsy
The possible causes of otalgia are: (1) acute inflammatory processes (acute otitis externa, acute suppurative otitis media, acute coalescent mastoiditis, otitis media with effusion (OME), bullous myringitis, ‘malignant’ necrotising otitis externa (and some rarities); (2) referred pain; (3) neurological; (4) psychogenic (Box 2.2).
- acute inflammatory disease of the external ear or middle ear cleft
- diseases not primarily in the ear
- referral from other sites
- neurological disease
- psychogenic
- referral from other sites
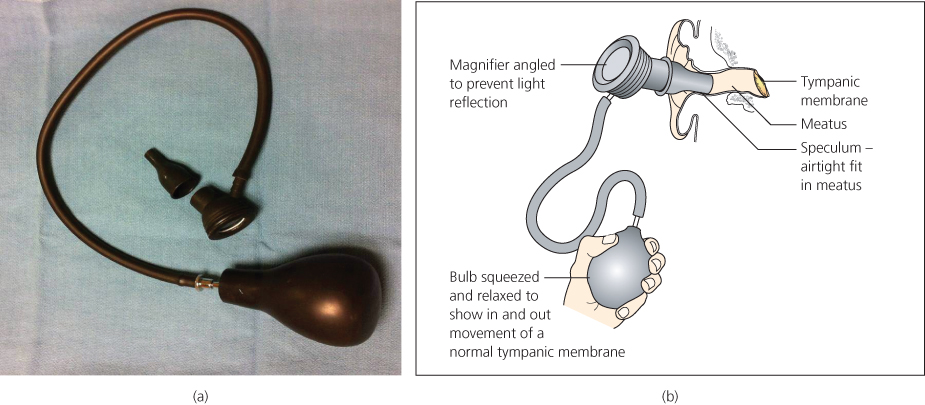
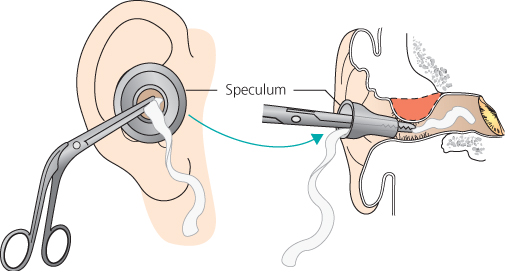
Inflammatory causes are recognized by skilled inspection of the external ear and tympanic membrane. As described in Chapter 1, examination of and around the pinna, precedes that of the ear canal (external acoustic meatus) and tympanic membrane (drumhead). An otoscope is the commonest tool available in general practice (Chapter 1), but otologists always prefer the use of a headlight or head mirror with a light source to cast light in the direction of vision down the meatus, and to allow instruments to be used with both hands for the removal of wax or debris; for the assessment of drum mobility using a pneumatic speculum (which also provides low power magnification) (Figure 2.1); and to show fluid sucked through any perforation. Then the tympanic membrane is examined with a binocular microscope).
The binocular microscope (functionally similar to microscopes used in otological surgery) is essential for the fine use of microinstruments and suction apparatus, providing stereoscopic magnification of 6× or more (Figure 2.2).

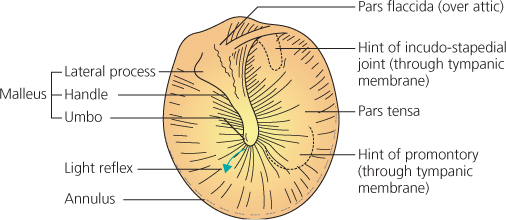
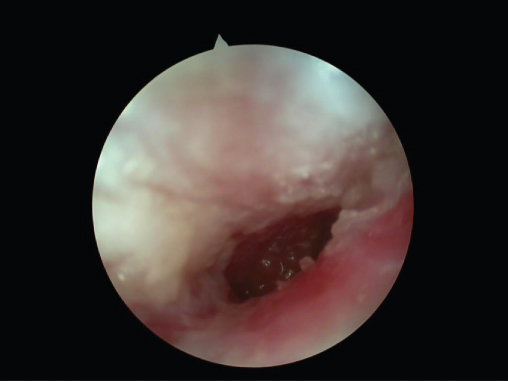
If the external ear canal and the tympanic membrane are definitely normal (Figure 2.3), then pain is not due to ear disease. The reliability of this judgement depends entirely on the skill and experience of the examiner. Many tympanic membranes show apparent abnormalities that are not caused by acute disease. Tympanosclerotic pale yellow or white patches are an example. These are not always confidently recognised, but are irrelevant to any acute inflammatory disease. If there is any doubt, or if parts such as the attic cannot be seen, an expert otological opinion is needed (Figure 2.4).
Figure 2.3 Normal left tympanic membrane: lateral process of malleus, below attic, handle of malleus with umbo at its lower end, and light reflex.

Acute otitis externa
Acute otitis externa may be either diffuse—involving all the skin of the external meatus (Figure 2.5) or localized as a furuncle (Figure 2.6).
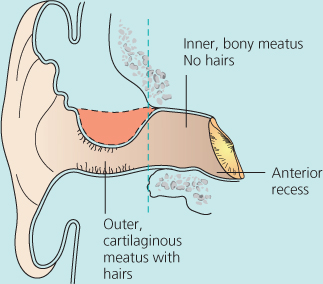
A furuncle is a tender painful swelling (a boil). It is always in the outer ear canal, where hair follicles are found, never in the inner bony meatus. Hearing is impaired only if the meatus becomes blocked by swelling or discharge, and fever occurs only if infection spreads in front of the ear, as cellulitis or erysipelas. Superficially tender enlarged nodes may be palpable in front of or behind the ear. The pinna is tender to movement in acute otitis externa, but this is never the case in acute otitis media. Discharge, if any, is usually thick and scanty, unlike the copious mucoid discharge through a tympanic membrane perforation from acute middle ear infections. Fungal skin infections cause severe pain with wet desquamation of keratin and black or coloured granules of the fruiting heads of conidiophores.
Treatment of acute otitis externa
Systemic antibiotics are only advised in acute otitis externa if there is fever or lymphadenitis. Meatal swelling is reduced by inserting a ribbon gauze wick impregnated with a deliquescent substance such as magnesium sulphate paste, or glycerine and 10% ichthammol (Figure 2.7). Proprietary expandable ‘Pope’ wicks (Xomed), are thin and stiff allowing careful insertion with small forceps. They soften and swell gently against the meatal walls when moistened with liquid medication. Wicks should be replaced daily until the skin swelling subsides.
Ear drops may then be used: aluminium acetate to ‘toughen’ the skin; 2% aceticid otic solution to restore the normal acidic state of the ear canal; or topical aminoglycoside antibiotics such as gentamicin, framycetin or neomycin, combined with corticosteroids. Topical clotrimazole is a useful antifungal agent. Systemic analgesics, together with warmth applied through a hot pad, heat lamp, or warm oil drops, relieve pain. Any discharge should be swabbed for laboratory examination, but treatment is started before awaiting a report.
Recurrent furunculosis is always a reason to exclude diabetes.
Acute suppurative otitis media (ASOM)
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


