Fig. 9.1
Donor keratocytes as a proportion of total keratocytes counted in each of 52 corneal grafts, plotted against graft age. Subset of eight transparent grafts removed due to reasons other than endothelial decompensation. Donor keratocyte survival did not correlate with graft age (Reproduced from Lagali et al. [25]. doi:10.1167/iovs.08-2923. Epub 2009 Jan 17)
Fig. 9.2
Fluorescence microscope images used for FISH analysis of corneal sections. (a) Epithelial (bottom) and stromal (top) cells in a female donor corneal button removed from a male recipient. All epithelial cells with two distinct signals had one red and one green signal per cell. Keratocytes had either one red and one green signal (arrow) or two red signals (arrowhead) per cell. (b) Endothelial cells at the posterior surface of a male donor corneal button removed from a female recipient. Endothelial cells with one red and one green signal (arrow) or two red signals (arrowhead) per cell were observed bar: (a) 50 m, 20 objective; (b) 10 m; 100 objective. frequently observed adjacent to one another in the central cornea. Bar, 50 m (Reproduced from Lagali et al. [25]. doi:10.1167/iovs.08-2923. Epub 2009 Jan 17)
Interestingly, the mix of donor and recipient cells may be responsible for an altered phenotype of the recurrence of corneal dystrophies [27].
Recurrence Following Corneal Grafting for Corneal Dystrophies
In a classic review (1978), Waring 3rd et al. [28, 29] describe the corneal dystrophies and their tendency to recur after PKP. Due to advances in molecular genetics, the focus here has been placed on the more recent literature.
The Bowman layer dystrophies, the Reis-Bücklers and the Thiel-Behnke and the stromal dystrophies, the granular types, and the lattice types of dystrophies are subjected to PKP (penetrating keratoplasty) or DALK (deep anterior lamellar keratoplasty). The more superficial dystrophies, the epithelial, are generally treated with phototherapeutic keratectomy or by other means.
Modern molecular genetics have enabled the subdivision of the dystrophies based on gene location and mutation analysis. Several dystrophies emanate from different mutations in the same gene. Therefore, a more precise prognosis can be decided only on the basis of type of mutation in the individual [30].
In the literature, a recurrence of the inherited disease is either classified as signs of the original disease in the graft or as an actual reoperation caused by the recurrence.
With few exceptions, Bowman layer corneal dystrophies are the most anterior changes that are subjected to corneal grafting. Both Reis-Bücklers’ (CDB1) and Thiel-Behnke (CDB ll) dystrophies are mutations in the BIGH 3 gene, and there are indications that the epithelium may be responsible for the pathologic changes. Both (there may be several subtypes) can recur in the graft.
In a study of 73 patients (110 eyes) grafted for corneal dystrophies originating in the BIGH 3 gene, 17 patients (27 eyes) were grafted for Reis-Bücklers’ (R 124 L) and 8 patients (13 eyes) from Thiel-Behnke dystrophy (R555Q). Of the Reis-Bücklers’ cases, significant recurrence was found in 24 of the 27 operated eyes within a mean time of 5.9 years. In the Thiel-Behnke eyes, dystrophic changes recurred in the graft in 5 of the 13 operated eyes within a mean time of 15 years.
Three other BIGH 3-derived corneal dystrophies showed significant recurrences:
In classic granular dystrophy (C6CD1RSSSW), 13 out of 28 eyes showed significant recurrence after 10 years. Twenty eyes were grafted for lattice type l dystrophy (LCDI/R124C). Ten of these showed significant recurrence within 11.3 years. Diagnosis using mutation analysis creates small subgroups that can show more frequent and rapid recurrences compared to the main dystrophy type [30].
Of 61 PKPs in 39 patients with lattice type l dystrophy, 48 % of the grafts showed clinical signs of recurrence within 3–26 years. Subepithelial opacities and anterior stromal haze were the most common findings. Only 1 eye presented with lattice figures. Fifteen percent of the eyes needed regrafting [31] (Fig. 9.3).

Fig. 9.3
Classic lattice dystrophy (a). Recurrence of lattice changes in the form of superficial opacifications without lattice lines (b). The superficial changes can successfully be removed with phototherapeutic keratectomy (c)
In 54 PKP-operated eyes (37 patients) due to stromal dystrophies with a long follow-up (lattice dystrophy 21 eyes, granular dystrophy 19 eyes, and macular dystrophy 14 eyes), recurrences appeared earlier in younger patients. Macular dystrophy has a better prognosis than granular and lattice type I dystrophy in terms of recurrences. Seven out of the 21 eyes with lattice had recurrences, and fourteen out 19 eyes with granular had recurrences [32].
In a large material from England, the frequency of diagnosis (dystrophies) out of all together 3555 grafts, 1452 had to be reoperated. One hundred and one of the repeat surgeries or 7.2 % were due to recurrence of corneal dystrophies [33].
DALK has been evaluated as an alternative to PKP in lattice dystrophy l, and the outcome was compared to DALK in macular dystrophy [34]. Sixty eyes with lattice dystrophy and 24 eyes with macular dystrophy were operated on with a DALK technique. It was concluded that DALK was a favorable technique for lattice dystrophy, whereas for macular dystrophy, the DALK was not as good [34]. Endothelial density deteriorated faster in macular dystrophy. DALK has also been evaluated for granular dystrophy. Recurrences were common. Simple recurrence occurred in 5 out of 7 eyes (mean time to recurrence was 15.6 months). Clinical significant recurrence occurred 34 month after surgery in 3 out of 7 eyes. Two eyes showed no recurrence [35].
In another more recent material where DALK was performed in 9 eyes with granular dystrophy, 2 eyes showed a recurrence (22 %), one of which as early as after 14 months. The mean follow-up time was 43.5 months.
In the same material 1 out of 43 grafts with macular dystrophy (2.3 %) and 6 eyes with lattice dystrophy (35.3 %) recurred [36].
Macular Dystrophy
Opacities from macular corneal dystrophy recur less commonly than in lattice and granular dystrophies [28]. There is however a considerable variation in the literature.
In a cohort of patients operated on in Saudi Arabia with PKP for macular dystrophy (229 eyes in 141 patients) followed for a mean of 5.9 years, clinical significant recurrence was observed in 5.2 % of the grafts [37] (Fig. 9.4).
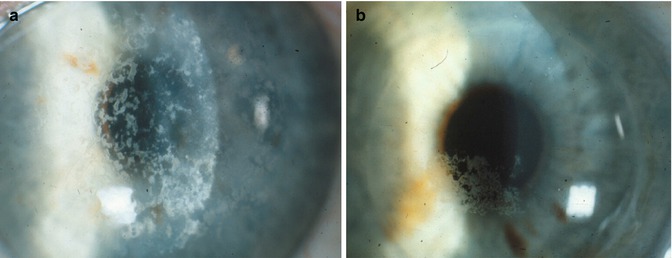
Fig. 9.4
A 56-year-old male with macular dystrophy in the right eye (a) and recurrence of the changes 6 years following a penetrating corneal graft (b)
In two recent reports, a comparison of PKP and DALK for macular corneal dystrophy was analyzed.
The highest recurrence figures were reported in a retrospective study where PKP was performed in 57 eyes and DALK in 21 eyes. Mean follow-up time was 5.1 years. Seventeen percent of PKP-treated eyes showed recurrences and so did 42.9 % of the DALK eyes. The younger the onset of the disease and the younger at surgery, the higher the risk of recurrences [38].
In a randomized trial [31] (54 patients an 82 eyes), recurrence of disease (follow-up 30.5 months) was 4.8 % in the PKP group and 5.7 % in the DALK group. There was less endothelial damage in the DALK group [39].
In a British material, 16 patients who underwent 41 transplants in 31 eyes were followed between 25 and 408 months from the initial diagnosis. Six eyes of four patients were regrafted after recurrence of the disease. Clinical recurrence was observed in two more eyes. It was furthermore assessed that a larger graft showed less recurrence [40].
In a report from Iran 2009, 62 eyes of 39 patients underwent PKP for macular dystrophy and were followed for a mean of 52 months. Only one eye showed a minor recurrence [41].
Schnyder Dystrophy
In a retrospective case series of 115 individuals from 34 families with Schnyder dystrophy, it was found that the crystal component of the corneal changes was observed only in 54 % of the affected individuals.
PKP had been performed in 54 % of patients when older than 50 years and in 77% when older than 70 years. In 8 of 39 eyes that underwent PKP for Schnyder dystrophy, the disease recurred in the graft. There was no repeat surgery for dystrophy recurrence [44, 45].
In 77 eyes (48 patients) with stromal dystrophies, recurrence was most common in Bowman layer corneal dystrophy, Reis-Bücklers, and followed by granular and lattice dystrophies. Both macular dystrophy and Schnyder dystrophy were infrequent, and within the comparatively short follow-up (2–3 years), none had recurrences [46].
Avellino Dystrophy
Granular corneal dystrophy type 2 or Avellino dystrophy is caused by a mutation in the T6FB T I. Several reports exist on a reactive recurrence following PTK, LASIK, and LASEK. Early recurrence was noted after PTK and LASEK in a homozygous individual [47–49].
Holland et al. examined 27 family members with the disease. Of these, 3 had been grafted previously and two of those showed granular deposits in the grafts. The earliest changes were 9 year post-op. The granular deposits also precede lattice lines in the natural development of the disease [50].
Repeat Grafts
In one material, between 1990 and 1999, 1096 procedures were performed; 784 patient records were available for evaluation. Regrafting was the most common indication, accounting for 40.9 % of all cases [1].
Between 1989 and 1995, 16 % (271 of 1689) of transplants performed in Wills Eye Hospital were regrafts compared with 9 % (165 of 1860) in the period from 1983 to 1988 (P < 0.01) [51].
Of 243 repeat PKP performed in 210 eyes of 208 patients were included in the study. 5.7 % of the repeats were stromal dystrophies (constituting 4.9 % of the cases to begin with). Follow-up was 43 months. The best graft survival was in eyes with an original diagnosis of keratoconus (93.8 %), and the worst was in eyes with Fuchs’ dystrophy (23.1 %). Overall, 29.6 % of eyes achieved a final visual acuity greater than 20/200, while only 4.8 % were 20/40 or better. The best visual prognosis was in eyes with an original diagnosis of stromal dystrophy and keratoconus [52].
150 repeat grafts at the Wills Eye Hospital in 1985–1995 were reviewed. Fuchs’ dystrophy constituted 21 out of the 150 (14 %). Corneal dystrophies constituted 1.7 % of the original indications [53].
Fuchs’ Dystrophy
Damage to the corneal endothelium or disease in the endothelium results in stromal edema and subsequently epithelial edema and then bullous keratopathy.
By definition, a corneal dystrophy is inherited. Spontaneous cornea guttata, followed by stromal edema and bullous keratopathy, is common, whereas true hereditary bullous keratopathy, or Fuchs’ dystrophy, is fairly uncommon. In one US study 13.6 % had a documented family history [54]. If the many spontaneous cases are caused by gene defects remains to be shown. The present knowledge on the basics of “Fuchs’” dystrophy has recently been reviewed [55].
In most materials corneal edema is subdivided into two groups, postsurgical pseudophakic or aphakic bullous keratopathy and Fuchs’ dystrophy. The latter group contains both hereditary and nonhereditary corneal edema. “Fuchs’ dystrophy” constitutes a substantial part of the indications for corneal transplantation. The figures range between 0.5 and 23.8 %.
In two German materials and one US material, the indication for Fuchs’ dystrophy increases [9, 10, 17] and diminishes in one over time [5].
Fuchs’ dystrophy including what is known about the complicated heredity when present has been recently reviewed. There are at least two subforms, one with early onset starting around 30 years of age and one form with a late onset manifesting at about 60 years. Further genetic analysis is needed to clarify the varying aspects of disease [56]. It is an open question whether “Fuchs’ dystrophy” recurs in the graft in the form of cornea guttata. New knowledge of the dynamics of the endothelium in the graft and host makes genuine recurrence possible [26]. The indication for regraft is generally corneal decompensation.
In a large material of PKP in 3993 eyes, Fuchs’ dystrophy constituted 25 % of the primary surgeries. Graft survival after 5 years was 97 and 90 % after 10 years compared to keratoconus, 97 to 92 % [57].
Repeat penetrating grafts in Fuchs’ patients constituted about 15 % of all repeat grafts. Fuchs’ constituted 15 % of the indication for the first graft. The average time to the repeat grafts was 6.3 years. 7.7 % of the repeat grafts failed. The two main reasons were endothelial failure in eight out of the 21 failed regrafts and rejection in another eight 8 [53].
Fuchs’ dystrophy constituted 3.9 % of indications in a large English material of 3555 cases. The group Fuchs’ dystrophy constitutes 140 of the 329 corneal dystrophies undergoing PKP in 1971–1990 [33]. Repeat PKP for Fuchs’ dystrophy showed a survival rate of 23.1 % after 43 months which is very low compared with eyes with the original diagnosis of keratoconus, 93.8 % [52].
In the Swedish National Cornea Register, the failure rate of the first operation was 15 % within 2 years, compared to 34 % for the regrafts. There was a higher rate of postoperative complications (suture related, glaucoma, etc.) following the regraft, 58 % compared to 34 % following the first graft [58].
The prevalence of Fuchs varies in different countries. Fuchs is rare in countries like Japan, Saudi Arabia, China, and Singapore. In the United States the prevalence is about 4 % [55].
Posterior Polymorphous Cornea Dystrophy
There are very few reports of corneal grafts performed for posterior polymorphous dystrophy. Two cases underwent PKP because of posterior polymorphous dystrophy at the age of 25 and 33 years, respectively. Six months and 18 months post-op, signs of recurrence, faint haze, or a dull appearance at the level of the endothelium were noted. Both eyes had to be regrafted 7 and 9 years after the first surgery [51]. Waring III in his review from 1978 states that no recurrences had been documented in grafts from posterior polymorphous dystrophy [29] (Fig. 9.5). The largest material described consisted of 120 patients. 13 of those were grafted in altogether 22 eyes. 9 of the grafted eyes opacified during the follow up period [59].

Fig. 9.5
Posterior polymorphous dystrophy in a 27-year-old female. Best spectacle corrected visual acuity was 0.3, and topography showed an concomitant keratoconus
DSEK and SMEK
DSEK and DMEK are becoming the major grafting techniques for treating endothelial disease or “Fuchs’ dystrophy.” The shift from PKP has been fairly rapid. Prospective randomized studies comparing the old and the new technique have not been published.
Result from the Australian Corneal Graft Registry published in 2014 with a large number of corneal grafts (13,920) makes it possible to compare 858 DALK, 2287 endokeratoplasties with PKPs. The main outcome measure was graft survival. It was concluded that graft survival was worse in both DALKs and endokeratoplasties compared to PKPs over the same time frame. They also state that an evidence for a learning curve is unconvincing [60].
In 2011, in a Cochrane Review [61], the authors concluded that there was no high-quality evidence that endokeratoplasty was superior to PKP. Further randomized controlled trials of visual and refractive outcome need to be performed. A similar conclusion, although stressing the force of numerous published case series, was drawn 2013 in a German review. The authors conclude that Descemet’s membrane endothelial keratoplasty (DMEK) is advantageous over Descemet stripping endothelial keratoplasty (DSEK) which in turn has better results than PKP [62]. The value of data in larger numbers in national registers was discussed in detail in a recently published editorial. These data also reflect the level of quality of care that is reached in the medical community in general [63]. Of 396 DSEK procedures, 20 failed, 40 % due to primary endothelial failure, 40 % due to progressive endothelial failure, and 20 % due to endothelial rejection. Repeat DSEK was performed on average 13 months after the first operation. The follow-up from repeat surgery was 27 months. The visual acuity outcome was satisfactory [64].
In 44 eyes with macular corneal dystrophy, 18 eyes with lattice dystrophy, and 12 eyes with granular dystrophy, DALK was completed in 69 cases (94.6 %). The mean follow-up period was 43.5 ± 23.9 months. Postoperative best spectacle-corrected visual acuity of 0.5 or better was present in 52 of 69 eyes (75.4 %). Lattice dystrophy recurred in 6 eyes (35.3 %) [36].
Keratoconus
Three indications for PKP are leading: pseudophakic bullous keratopathy, keratoconus, and regrafts. Regrafts have increased in the last decades, whereas keratoconus has declined in importance somewhat.
The keratoconus proportion of indications for corneal grafting is 2.5 % in Taiwan [11], 13 % China [16], 5.7 % China [19], 15.5 % Canada [14], 25.5 % Germany [9], 45.6 % N Zealand (1991–1999) [13], 26 % Greece [7], 12.1 % France [3], 16 % United States [8], and Great Britain 15 % [1].
In the Australian Corneal Graft Registry, survival rates of penetrating grafts after keratoconus were 89 % after 10 years, 49 % after 20 years, and 17 % after 23 years. After 15 years the survival rate was similar to that of all other penetrating grafts. Recurrent keratoconus caused failure in 4 % of the 4834 keratoconus grafts. In grafts surviving 15 years or more (n = 235), recurrent keratoconus constituted 12 % of the graft failures [65]. In a study of 112 eyes that underwent PKP for keratoconus, the rate of recurrence after 25 years was 11.7 % [66]. In another study, the probability of 20 years after surgery to suffer recurrence of keratoconus was 10 % [67]. The same study concluded that the greatest risk of rejection was during the first two postoperative years.
Recurrence of keratoconus is usually a late complication [68–71], in the majority of cases due to a progressive disease in the host cornea, being more accentuated if the original graft is small. Progressive, late development of astigmatism is a probable forerunner of recurrent keratoconus in the graft [71, 72].
The morphology of ectatic grafts is similar to that of keratoconic corneas [68–71, 73]. There is also a risk, although minimal, of grafting corneas from donors with keratoconus [74, 75].
Dalk has been used as an alternative to PKP in grafting for keratoconus. The experience of postoperative complications is not long, but the time to recurrent ectasia may be shorter [76, 77].
In corneal grafts (PKP) for keratoconus, the age of primary surgery was 33 years. Ectasia developed 22 years later on average. Two out 15 regrafts developed ectasia again [78].
Keratoconus can be associated with other corneal dystrophies as macula dystrophy [79–81], granular dystrophy [82], posterior polymorph dystrophy (Fagerholm P 2002), and lattice dystrophy (Fagerholm P 2005). If corrected visual acuity is worse than expected, concomitant keratoconus can be an explanation.
Salzmann’s Nodular Degeneration
Salzmann’s nodular degeneration is bilateral in 63 % of the affected and affects foremost women (89 %). The progression of the disease is accompanied by hyperopization and increasing astigmatism [83]. Decreased visual acuity is the most common symptom [84]. The disease is accompanied by meibomian gland dysfunction in 33 % of the cases, peripheral vascularization in 31 %, associated contact lens wear in 33 %, pterygium in 16 %, keratoconjunctivitis sicca in 10 %, and exposure keratitis in 4 % (Fig. 9.6).

Fig. 9.6
Salzmann’s nodular degeneration in a 47-year-old female. Iron lines are typical bordering the keloidlike changes
These data spring from a cohort of 93 cases with the disease [83]. Recurrent erosions are not uncommon [85]. Impaired vision necessitated surgery in 85.5 %. In 79 % vision improved [83]. Most patients are operated on with manual keratectomy [86]. PTK has been evaluated [87–89]. Mitomycin has been added to both the manual and laser procedures with the motivation to minimize recurrences [86, 87, 89]. PKP is sometime employed, more so before the advent to mitomycin C and PTK. None the less, Salzmann’s nodular degeneration can recur after PKP [90] but often after a longer time span and after lamellar keratoplasty [91].
Herpes Simplex Keratitis
Herpes simplex keratitis has been a constant but limited indication for corneal grafting in most materials. Opacities due to herpes simplex keratitis (HSK) have been more common as an indication in developing countries [22, 92, 93]. In statistics spanning over a longer period, the indication for PKP for herpes keratitis is diminishing [7, 21, 94]. In several materials the proportion of HSK cases that has been grafted constitute somewhere between 1 and 7.3 % [1, 3, 7, 18, 21, 84, 95].
It was shown that an increased virus load in the excised corneas made the prognosis worse for the graft. So did preoperative steroid treatment, severity at the time of surgery, and corneal neovascularization [96, 97]. The increased risk of allograft failure was also determined retrospectively from the histopathologic presence of corneal vessels [98]. The authors also found that vessel in the cornea increased the risk of recurrences. The latter conclusion contradicts the findings from a previous study [99] where no increased risk of recurrences from vessels present in the stroma was found.
In a Danish material from 1995 with 72 penetrating grafts for HSK without antiviral therapy, the recurrence rate after 2 years was 44 %. The 2-year survival rate of the grafts was 67 % [100].
In a retrospective study published the same year, the recurrence-free survival rate after 4 years was 51 %. Recurrence of HSV infection occurred in 18 of the 49 eyes. In 50 % of grafts with recurrences, the result was an opacified graft [101].
In a study from Germany (1993), the survival rate for 11 years after PKP for HSK was 68 %. Corneal inflammation at the time of surgery was found to be a negative prognostic factor [99] (Fig. 9.7).
Fig. 9.7
Herpes simplex keratitis grafted á chaud in the era before antiviral therapy. Postoperative inflammation was intensive and the scaring produced a prominent keloid
In two other series, rejection was the principal cause of graft failure in 64 % and 46 %, respectively, whereas viral recurrence caused failure in 15 and 16 %, respectively [102, 103]. Graft survival after 2 years was 67 and 66 % [100, 102]. In the Australian Corneal Graft Registry, if recurrence-free, the grafts survive in 83 %. The report concludes that viral recurrence has a major impact on graft survival [104].
Graft survival following PKP has improved since prophylactic treatment with acyclovir was introduced.
In a study from 1994, the use of topical antivirals to reduce the risk of viral recurrence and graft rejection was compared to a group of patients given no prophylactic treatment [105]. Sixty-six (52 %) of the grafts received prophylactic postoperative topical antiviral treatment, and 59 (46 %) received no antiviral therapy. Postoperative prophylactic antiviral treatment was associated with decreased rates of herpes simplex keratitis recurrence and allograft rejection. In a prospective trial with oral acyclovir, the advantage of prophylaxis was evident [106]. In the small material, there were no recurrences of herpes simplex keratitis in any patient receiving acyclovir (mean follow-up of 16.5 months) compared with a 44 % (four of nine) recurrence rate in patients without acyclovir (mean follow-up of 20.6 months). Graft failure occurred in 14 % (2 of 14) of acyclovir treatment eyes compared with 56 % (five of nine) without.
Deep anterior lamellar keratoplasty has been compared with PKP when grafting for HSK opacities [107]. Fifty-eight eyes in 58 patients were operated on with DALK and 63 eyes in 63 patients with PKP. The follow-up time was about 46 months in both groups. There were no rejections in the DALK group, whereas 26 eyes (41.3 %) suffered rejection in the PKP group. There were 21 episodes of recurrence in the PKP group compared to 7 in the DALK group. Fourteen eyes failed in the PKP group compared to 1 in the DALK group [107]. The patient’s received oral acyclovir for 12–18 months post-op.
A low graft rejection rate, 2.3 %, was reported after DALK in 44 patients given intravenous acyclovir and amniotic membrane prior to DALK. The follow-up time was 29.1 months (range 1–4 years). Fourteen percent developed recurrent HSK [108].
In another series of 52 eyes in 52 patients, DALK was performed and the patients were followed for a mean of 31 months. Both acyclovir and topical steroids were given for 1 year after surgery. No rejections or recurrences were noted [109].
On the other hand, a high percentage of postoperative complications were observed following DALK in another material of 18 patients. Six patients, or 33 %, experienced recurrence of HSK, 50 % experienced an episode of graft rejection, and 28 % (five cases) suffered graft failure. The patients were given oral acyclovir and topical dexamethasone for 1-year post-op [110]. A good effect of acyclovir prophylaxis was confirmed in a 5-year follow-up, placebo-controlled, randomized trial on acyclovir prophylaxis after keratoplasty [111].
Prophylaxis
In his commentary from 1998, Larkin concludes that oral antiviral prophylaxis for 1 year following PKP for HSK, accompanied by topical steroids, is a reasonable strategy [112].
This is confirmed in subsequent studies [113–117]. Oral antiviral therapy and postoperative steroids, furthermore, help in preventing relapse of neovascularization [118].
Herpes simplex virus keratitis is reported to be more common in patients with atopic disease [119, 120] (Fig. 9.8).
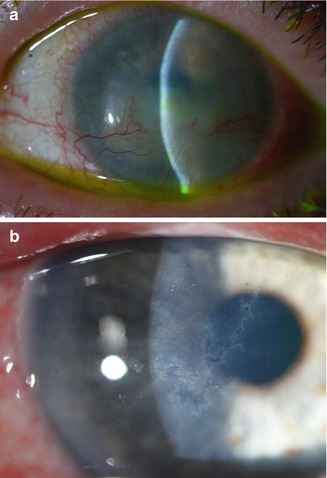
Fig. 9.8
Herpetic keratitis in the right eye of a woman with atopic dermatitis and keratoconjunctivitis (a). The sequel of a previous attack of herpes simplex keratitis is seen in the left eye (b)
When comparing the outcome of PKP for HSK, it was shown that nonatopics had significantly more epithelial recurrences, although in general the incidences of recurrences were low and high graft survival numbers were reported [119]. Antiviral prophylaxis for HSV recurrences was proven more effective in reducing infections in atopics and less effective in reducing inflammatory episodes in atopics versus nonatopics. A recurrence of herpetic disease following PKP for HSK is likely to originate from the host, either via nerves from the trigeminal ganglion or from latency in the remaining host epithelium [121].
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


