Purpose
To report the initial experience, clinical outcomes, and safety profile of 27 gauge pars plana vitrectomy (PPV) in eyes with posterior segment disease.
Design
Multicenter, retrospective, interventional case series.
Methods
setting : Private practice and tertiary care settings. study population : Eyes undergoing 27 gauge PPV for a vitreoretinal surgery indication. intervention : Three-port, transconjunctival 27 gauge PPV. main outcome measures : Change in visual acuity and occurrence of intraoperative and postoperative complications with minimum follow-up of 90 days.
Results
Ninety-five eyes met the inclusion criteria. Surgical indications included epiretinal membrane (n = 26), diabetic tractional retinal detachment (n = 14), full-thickness macular hole (n = 11), rhegmatogenous retinal detachment with (n = 7) or without (n = 9) proliferative vitreoretinopathy (PVR), vitreous hemorrhage (n = 10), vitreous opacities (n = 8), endophthalmitis (n = 4), sub–silicone oil retinal detachment (n = 3), retained lens material (n = 1), submacular hemorrhage (n = 1), and aqueous misdirection (n = 1). Mean logMAR visual acuity improved from 1.08 ± 0.71 (20/240 Snellen equivalent) preoperatively to 0.53 ± 0.65 (20/67 Snellen equivalent) postoperatively ( P < .001). Mean follow-up was 144 days (median 127 days, range 90–254 days). There were no intraoperative complications and no case required conversion to 20, 23, or 25 gauge instrumentation. A total of 3 sclerotomy sites (1.1%) were sutured at the conclusion of surgery. Postoperative complications included transient ocular hypertension in 8 eyes (8.4%), transient hypotony in 5 eyes (5.3%), and vitreous hemorrhage in 5 eyes (5.3%). No cases of postoperative endophthalmitis, sclerotomy-related retinal tears, or choroidal detachments were encountered in the follow-up period.
Conclusion
The 27 gauge PPV was well tolerated with low rates of intraoperative and postoperative complications across varied surgical indications.
Microincision vitrectomy surgery (MIVS) with 23 gauge and 25 gauge instrumentation has largely replaced traditional, 20 gauge pars plana vitrectomy (PPV). As initially suggested by Lakhanpal and associates, use of smaller-diameter instruments with self-sealing, transconjunctival scleral wounds offers several advantages that have now been well documented in the literature, including decreased postoperative pain and inflammation, decreased astigmatism, and faster visual recovery. In a 2010 Ophthalmic Technology Assessment report by the American Academy of Ophthalmology, visual outcomes and complication rates of MIVS were found commensurate to 20 gauge vitrectomy benchmarks.
In 2010, Oshima and associates described the initial feasibility and safety of a novel 27 gauge MIVS system, reporting excellent visual and anatomic outcomes in a series of 31 patients. As with prior reports describing initial experience with 23 gauge and 25 gauge MIVS, the series focused primarily on macular cases of lower complexity. With use of 1-stage, straight incisions, no postoperative wound-related complications were encountered in any patient. The authors suggested that smaller 27 gauge instrumentation may reduce wound integrity concerns encountered with 23 gauge or 25 gauge systems.
No larger, multicenter case series from the United States regarding outcomes of 27 gauge vitrectomy surgery have been published since the commercial introduction of this technology by several different manufacturers. The purpose of this study is to review the initial experience, clinical outcomes, and safety profile of a 27 gauge MIVS system for a variety of vitreoretinal indications.
Methods
Institutional Review Board approval from Wills Eye Hospital was obtained for the retrospective review of clinical records for all patients who underwent 3-port, transconjunctival PPV using a 27 gauge system (Constellation Vitrectomy 27+ Total Plus Pak; Alcon Laboratories, Fort Worth, Texas, USA) from May 1, 2014 to January 31, 2015. This research adhered to the tenets of the Declaration of Helsinki and was conducted in accordance with regulations set forth by the Health Insurance Portability and Accountability Act. The clinical sites participating in this multicenter, consecutive, interventional case series included Wills Eye Hospital, Philadelphia, Pennsylvania; Eye Consultants of Maryland, Owings Mills, Maryland; Retinal Consultants of Arizona, Phoenix, Arizona; Berrocal & Associates, San Juan, Puerto Rico; and Cincinnati Eye Institute, Cincinnati, Ohio. All patients were identified from surgical operative reports and were included if they underwent 3-port, 27 gauge PPV for a vitreoretinal surgery indication. Eyes undergoing concurrent cataract extraction were included in the analysis. However, eyes undergoing concurrent glaucoma filtering surgery and/or corneal transplantation surgery were excluded. All surgeries were performed and managed postoperatively by the authors (M.H.B., P.U.D., A.C.H., J.H., M.A.K., R.R.L., Ca.D.R., Ch.D.R., Ar.S., B.T.).
Patient records were reviewed and the following data were collected: age, sex, preoperative and postoperative Snellen visual acuity (VA), preoperative and postoperative intraocular pressure (IOP), indication for vitreoretinal surgery, past ocular and surgical history, and lens status. Intraoperative surgical details including use of air, gas, or silicone oil tamponade; characteristics of wound construction; presence of retinal tears near sclerotomy sites; presence of sclerotomy site leakage; use of intraoperative sclerotomy suture; and total surgical time were recorded.
In each case, retrobulbar, peribulbar, or subconjunctival anesthesia was administered. Surgical eyes were prepared using 5% providone-iodone (Betadine; Purdue Fredrick Co, Norwalk, Connecticut, USA). All surgeries were performed using the Constellation Vitrectomy 27+ Total Plus Pak vitrectomy system (Alcon Laboratories). Cannulas were inserted in the inferotemporal, superotemporal, and superonasal quadrants 3.0–4 mm posterior to the limbus. The conjunctiva and Tenon capsule were displaced over the sclera to avoid communication between conjunctival and scleral entry sites. Trocar cannulas were inserted with a “straight in” (perpendicular to the sclera) or angled (less than 90 degrees to the sclera) approach according to surgeon preference.
Details of the surgical procedure varied based on posterior segment indication. A core vitrectomy was performed in all cases using a cut rate of 7500 cuts per minute (cpm) and linear aspiration of 0–650 mm Hg. Port bias was initially set to open. Machine settings were then modulated according to surgeon preference, as required by the surgical maneuver being performed. Triamcinolone acetonide, indocyanine green, and tissue plasminogen factor were used as surgical adjuncts based on surgical indication and surgeon preference. Fluid-air and fluid-gas exchange (16%–18% sulfur hexafluoride [SF6] or 12%–16% perfluoropropane [C3F8]) were performed as appropriate and according to surgeon preference. Membrane and/or internal limiting membrane peeling was performed for epiretinal membrane (ERM) or macular hole indications. Endophotocoagulation was used in cases of diabetic retinopathy and retinal detachment. Silicone oil (1000 centistokes) was used as tamponade in cases of proliferative vitreoretinopathy (PVR) or tractional retinal detachments as determined by the operating surgeon. At the conclusion of each case, a peripheral retinal examination was performed with scleral depression and wide-field viewing to evaluate for retinal breaks. All sclerotomy sites were inspected after removal of cannulas, and if required per surgeon discretion, a suture was placed to prevent leakage. A chandelier light source was not used in any case.
Ocular examination with Snellen visual acuity, applanation tonometry, and slit-lamp biomicroscopy was performed on all patients at the 1-day, 1-week, 1-month, and all subsequent postoperative visits for a minimum follow-up of 90 days. Postoperative complications, including hypotony, ocular hypertension, retinal detachment, endophthalmitis, and choroidal detachment, were also detailed if present. Hypotony was defined as a new-onset IOP of 6 mm Hg or less at any postoperative visit and ocular hypertension was defined as an IOP of 25 mm Hg or more at any visit. Snellen visual acuities were converted to logMAR equivalents for statistical analyses, with counting fingers (CF) and hand motions (HM) vision corresponding to 1.98 and 2.28, respectively. Using a paired Student t test analysis or Fisher exact test (GraphPad Software Inc, La Jolla, California, USA), a P value < .05 was considered statistically significant. The primary outcome measures were change in VA and occurrence of intraoperative and postoperative complications.
Results
Ninety-five eyes (51 left eyes and 44 right eyes) of 95 patients were included. Mean age at the time of surgery was 65 years (standard deviation 13 years, range 32–93 years), and 46 patients were female. Mean follow-up was 144 days (median 127 days, range 90–254 days). Forty-five eyes (47%) were phakic, 35 eyes (37%) were pseudophakic, and 15 eyes (15.8%) underwent concurrent cataract extraction and intraocular lens implantation at the time of vitrectomy surgery. Relevant past ocular history included proliferative diabetic retinopathy in 23 eyes (24.2%), prior PPV in 18 eyes (19.0%), and open-angle glaucoma in 11 eyes (11.6%). Of the eyes with a history of glaucoma, 1 eye (9%) had prior filtering surgery.
Surgical indications for vitrectomy included epiretinal membrane (n = 26), diabetic tractional retinal detachment (n = 14), full-thickness macular hole (n = 11), rhegmatogenous retinal detachment with (n = 7) or without (n = 9) PVR, vitreous hemorrhage (n = 10), vitreous opacities (n = 8), endophthalmitis (n = 4), sub–silicone oil retinal detachment (n = 3), retained lens material (n = 1), submacular hemorrhage (n = 1), and aqueous misdirection (n = 1).
No intraoperative complications were encountered, including sclerotomy-related breaks. No cases required conversion to 20, 23, or 25 gauge instrumentation. At the conclusion of surgery, 48 eyes (51%) were left with a fluid-filled vitreous cavity, 16 eyes (17%) with C3F8 gas, and 13 eyes (14%) with SF6 gas, 11 eyes (12%) were infused with air; and 7 eyes (7%) were infused with 1000 centistoke silicone oil. Three eyes (3.2%) required 1 sclerotomy suture for wound closure as determined by the operating surgeon, all of which were silicone oil–filled eyes. The 27 gauge instruments were found to be of sufficient rigidity to perform all surgical maneuvers in all eyes by all surgeons.
Primary outcomes are summarized in Table 1 . Mean logMAR VA improved from 1.08 ± 0.71 (20/240 Snellen equivalent) preoperatively to 0.53 ± 0.65 (20/76 Snellen equivalent) at final postoperative visit ( P < .001). Compared to a mean preoperative IOP of 16.8 ± 6.7 mm Hg (range 5–48), IOP was 16.1 ± 6.1 mm Hg (range 4–34) on postoperative day 1 ( P = .35), 15.7 ± 5.2 mm Hg (range 5–48) on day 7 ( P = .17), 16.1 ± 4.5 mm Hg (range 8–34) on day 30 ( P = .33), and 15.2 ± 3.4 mm Hg (range 8–24) at the final postoperative visit ( P = .021) across all eyes.
| Diagnosis (n) | Mean Age (Years ± SD) | Mean Preoperative IOP (mm Hg) | Mean IOP Day 1 (mm Hg) | Mean IOP Day 7 (mm Hg) | Mean IOP Day 30 (mm Hg) | Mean Preoperative LogMAR VA (± SD) | Mean Postoperative LogMAR VA (± SD) | P Value, VA | Mean Operative Time (Minutes ± SD) | Mean Follow-up (Days ± SD) |
|---|---|---|---|---|---|---|---|---|---|---|
| Overall (95) | 65 ± 13 | 16.8 | 16.1 | 15.7 | 16.1 | 1.01 ± 0.7 | 0.53 ± 0.65 | <.001 | 32 ± 28 | 144 ± 55 |
| ERM (26) | 69 ± 12 | 15.7 | 14.6 | 15.6 | 16.5 | 0.60 ± 0.48 | 0.29 ± 0.14 | <.001 | 27.7 ± 10 | 151 ± 55 |
| TRD (14) | 55 ± 7 | 14.4 | 18.2 | 14.3 | 14.9 | 1.48 ± 0.59 | 1.07 ± 0.79 | .11 | 47.9 ± 17 | 130 ± 62 |
| FTMH (11) | 71 ± 8 | 17.5 | 15.7 | 15.1 | 16.2 | 0.78 ± 0.32 | 0.30 ± 0.31 | <.001 | 23.3 ± 10 | 170 ± 58 |
| VH (10) | 56 ± 14 | 21.1 | 17.0 | 15.5 | 16.8 | 1.45 ± 0.70 | 0.29 ± 0.28 | <.001 | 30 ± 14 | 113 ± 47 |
| RRD (9) | 73 ± 11 | 17.3 | 19.8 | 17.2 | 16.6 | 1.10 ± 0.44 | 0.44 ± 0.34 | .02 | 36.5 ± 29 | 193 ± 53 |
| Vitreous opacities (8) | 65 ± 11 | 14.8 | 10.1 | 13.6 | 13.9 | 0.06 ± 0.1 | 0.02 ± 0.04 | .43 | 22.6 ± 8 | 117 ± 24 |
| PVR RRD (7) | 63 ± 16 | 13.6 | 17.7 | 20.3 | 18.1 | 1.56 ± 0.72 | 1.55 ± 0.90 | .98 | 45.3 ± 47 | 144 ± 53 |
| Endophthalmitis (4) | 70 ± 15 | 23 | 20 | 17.5 | 16.5 | 1.79 ± 0.43 | 0.64 ± 0.90 | .03 | 27.8 ± 18 | 155 ± 37 |
| Other a (6) | 66 ± 20 | 19.7 | 14 | 14.5 | 15.2 | 1.41 ± 0.64 | 0.65 ± 0.40 | .01 | 30.2 ± 11 | 108 ± 19 |
a Other = submacular hemorrhage (n = 1), sub–silicone oil retinal detachment (n = 3), retained lens material (n = 1), and aqueous misdirection (n = 1).
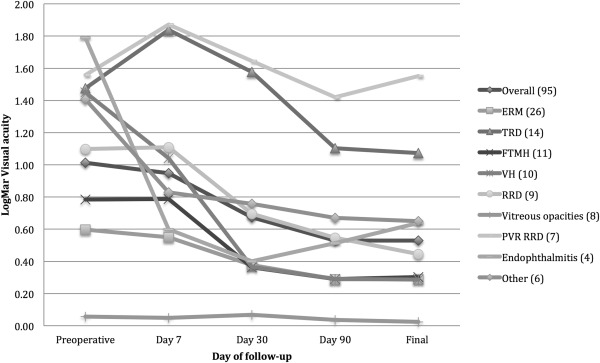
VA outcomes were assessed by surgical indication ( Figure 1 ). Statistically significant improvement in logMAR VA at final postoperative visit was noted for ERM (n = 26 eyes, P < .001), full-thickness macular hole (n = 11 eyes, P < .001), vitreous hemorrhage (n = 10 eyes, P < .001), rhegmatogenous retinal detachment without PVR (n = 9, P = .02), and endophthalmitis (n = 4, P = .03) indications. Improvement was noted for patients with vitreous opacities (n = 9 eyes, P = .43) and diabetic tractional retinal detachment (n = 14, P = .11) but did not reach statistical significance. No significant change in VA was noted for PVR-related retinal detachments (n = 7, P = .98). Anatomic success, including closure of macular hole, removal of ERM, clearing of clouded media, and repair of detached retina, was achieved in all eyes. VA improved in phakic eyes (n = 50, P < .001), pseudophakic eyes (n = 30, P = .006), and eyes that underwent concurrent cataract extraction (n = 15, P = .54).
IOP outcomes were compared among wound construction techniques and tamponade agents ( Table 2 ). Sixty-eight eyes underwent angled incisions and 27 eyes underwent straight (perpendicular) incisions. Compared to a mean preoperative IOP of 16.4 ± 7.7 mm Hg, IOP was 15.8 ± 6.8 mm Hg on postoperative day 1 ( P = .61), 15.3 ± 6.0 mm Hg on day 7 ( P = .60), and 15.9 ± 5.0 mm Hg on day 30 ( P = .60) for eyes with angled incisions. Compared to a mean preoperative IOP of 17.8 ± 2.7 mm Hg, IOP was 16.6 ± 3.8 mm Hg on postoperative day 1 ( P = .15), 16.6 ± 2.5 mm Hg on day 7 ( P = .06), and 16.7 ± 2.4 mm Hg on day 30 ( P = .05) in eyes with straight incisions. Comparing groups, there was no statistically significant difference in IOP between wound construction techniques at any time point, including day 1 ( P = .34), day 7 ( P = .28), day 30 ( P = .29), or final follow-up ( P = .19). Regarding the 3 total sclerotomy sites requiring suture at the close of surgery, 2 were constructed with an angled incision and 1 from a straight incision. Compared to preoperative values, mean IOP was 15.9 ± 16 mm Hg in eyes with silicone oil ( P = .06), 15.8 ± 3.6 mm Hg in patients with SF6 gas ( P = .50), 17.6 ± 5.22 mm Hg in eyes with C3F8 gas ( P = .74), 13.8 ± 3.2 mm Hg in eyes with air ( P = .11), and 16.2 ± 4.70 mm Hg in fluid-filled eyes ( P = .45) at postoperative day 30.
| Preoperative IOP (mm Hg) | IOP Day 1 (mm Hg) | IOP Day 7 (mm Hg) | IOP Day 30 (mm Hg) | P Value, IOP Day 30 | |
|---|---|---|---|---|---|
| Overall (95) | 16.8 ± 6.7 | 16.1 ± 6.1 | 15.7 ± 5.2 | 16.1 ± 4.5 | .33 |
| Tamponade (n) | |||||
| Fluid filled (48) | 16.9 ± 7.0 | 14.5 ± 6.2 | 15.3 ± 4.0 | 16.2 ± 4.7 | .45 |
| C3F8 gas (16) | 17.1 ± 3.5 | 19.9 ± 7.7 | 15.9 ± 3.4 | 17.6 ± 5.2 | .74 |
| SF6 gas (13) | 16.4 ± 3.2 | 16.2 ± 2.8 | 14.8 ± 3.2 | 15.8 ± 3.6 | .50 |
| Air (11) | 19.8 ± 10.8 | 15.9 ± 4.4 | 14.7 ± 4.8 | 13.8 ± 3.2 | .11 |
| Silicone oil (7) | 11.3 ± 4.1 | 18 ± 4.7 | 21 ± 13.5 | 15.9 ± 2.5 | .06 |
| Wound construction (n) | |||||
| Angled (68) | 16.4 ± 7.7 | 15.8 ± 6.8 | 15.3 ± 6.0 | 15.9 ± 5.0 | .60 |
| Straight (27) | 17.8 ± 2.7 | 16.6 ± 3.8 | 16.6 ± 2.5 | 16.7 ± 2.4 | .05 |
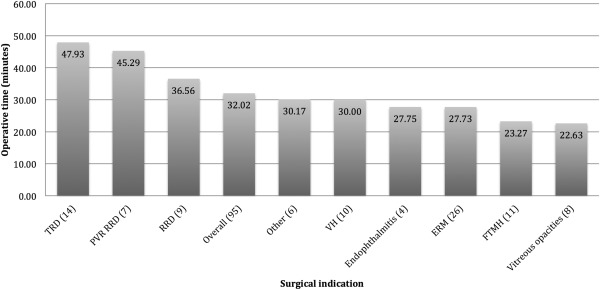
Total operative time was assessed for each diagnosis ( Figure 2 ). Across all cases, mean operative time was 32 minutes (median 15, range 11–87 minutes). If excluding eyes with concurrent cataract extraction (n = 15 eyes), mean operative time was 30.5 minutes (median 25.5, range 11–87). If excluding eyes with prior history of vitrectomy (n = 19 eyes), mean operative time was 32.2 minutes (median 28, range 11–87 minutes). Per indication, the mean operative time was shortest for vitreous opacities at 22.6 minutes (median 22, range 11–34 minutes) and longest for diabetic tractional retinal detachment at 48 minutes (median 47.5, range 15–74 minutes).