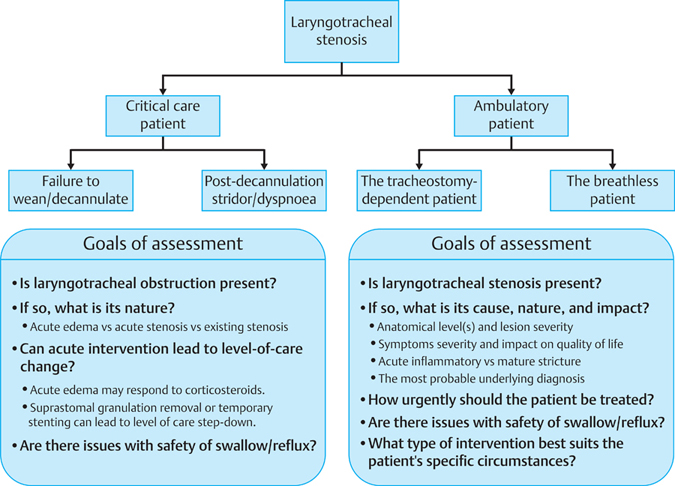
29 Outcome Assessment in Laryngotracheal Stenosis Laryngotracheal stenosis refers to abnormal narrowing of the central air passages from the supraglottic larynx to the carina and proximal main bronchi.1 It is caused by a heterogeneous group of diseases that have in common between them the ability to impair airflow and mucociliary clearance and in a smaller number of cases, swallowing and phonation also. The most common benign cause of this condition is intubation-related airway injury, followed by Wegener granulomatosis and idiopathic subglottic stenosis.1 Although most cases of laryngotracheal stenosis clinically present in a similar way with exertional dyspnea and chronic stridor, the disease entities that cause these symptoms are very different. The ability to restore a prosthesis-free airway capable of meeting the ventilatory demands of the patient is therefore more determined in the long term by the natural history of the underlying disease process being treated than by the ability of an intervention to acutely improve breathing by restoring lumen dimensions. In patients with supraglottic and laryngeal stenosis, restoration of the ventilatory conduit needs also to be balanced against the risk of damaging phonatory and/or swallowing mechanisms. These factors need to be carefully considered when assessing and treating patients with this condition. Outcome assessment is essential in determining safety and success of different treatment strategies used within and between centers. This chapter begins by discussing initial patient assessment and treatment goal setting and goes on to highlight a multidimensional paradigm for assessing outcome in laryngotracheal stenosis. The aims of initial assessment are to establish or confirm the diagnosis, to identify disease-specific risk factors and prognostic variables, to set realistic treatment goals in partnership with the patient, and to establish an initial management plan (Fig. 29.1). Assessment begins by eliciting general and disease-specific symptoms (Table 29.1). Many patients with laryngotracheal stenosis will have been initially misdiagnosed and treated for presumed “resistant” bronchopulmonary diagnoses. It is important therefore to try and obtain a clear time line of when symptoms were first noted as well as dates when initial diagnoses were made and treatments given. Figure 29.1 Overall approach for assessing a patient with laryngotracheal stenosis. Table 29.1 Initial Assessment of a Patient with Suspected Laryngotracheal Stenosis
Initial Patient Assessment and Treatment Goal Setting
Medical History
• Most common symptoms of laryngotracheal stenosis ○Breathlessness ○Stridor (inspiratory/expiratory/biphasic) ○Reduced effort tolerance ○Recurrent chest infections ○Dysphonia ○Dysphagia ○Hemoptysis ○Cough ○Throat or chest pains ○Difficult intubation ○Chronic tracheostomy dependency ○Failed extubation ○Prolonged weaning • Prediagnosis treatments ○Date symptoms first noted ○Initial diagnoses established and treatments given • Is there a history of endotracheal intubation or tracheostomy? ○No history of intubation ○Only minor history of intubation for short (< 1 h) surgery) ○Significant history of intubation (long surgery/mechanical ventilation) • If there is a history of significant intubation, then the following additional information needs to be ascertained | |
Indication for intubation: | [General medical/surgical/trauma/neurological] |
Date of intubation: |
|
Intubation setting: | [Surgery/intensive care] |
Duration of intubation: | [h/d] |
Agitation in ICU: | [Yes/No] |
Use of vasopressors in ICU: | [Yes/No] |
Multiple re-intubations: | [Yes/No] |
Endotracheal tube size: | [Size] |
Tracheostomy in ICU: | [No/Yes: percutaneous/Yes: surgical] |
Tracheostomy tube size: | [Size and type] |
Decannulation: | [Yes/No] |
Decannulation date: | [Date] |
d, day; h, hours.
Over half of all cases of laryngotracheal stenosis are caused by intubation-related airway injuries. Obtaining a detailed intubation history is therefore mandatory (Table 29.1). The second common cause of benign laryngotracheal stenosis is vasculitis-related airway stenosis, most commonly secondary to Wegener granulomatosis. Vasculitis symptoms need therefore to be specifically sought and if there is known or suspected vasculitis, then disease activity needs to be quantified. We use the Birmingham Vasculitis Activity Score (BVAS) for this purpose.2
Another factor which significantly impacts on treatment success is safety of swallowing, especially in supraglottic and laryngeal cases where laryngotracheal reconstruction may itself impact upon safety of swallowing, and in patients with neurological swallowing impairment where lumen restoration may lead to the development or worsening of chronic aspiration. Symptoms of chronic aspiration need therefore to be specifically sought and documented. A global assessment of patient function and ventilatory demands helps determine the most appropriate extent of reconstructive surgery.
Physical Examination
Physical examination for laryngotracheal stenosis consists of a general medical examination, an ear-nose-throat (ENT) examination, and a directed examination of the supraglottis and larynx with flexible endoscopy. Patient’s weight and height also needs to be noted. A body mass index > 40 significantly reduces the likelihood of treatment success.3
Evaluating the Intensive Care Patient
Within intensive care settings, a patient with obstructive laryngotracheal edema or acute or pre-existing stenosis may manifest with failure to wean or decannulate or post-extubation stridor. Many cases of extubation failure or stridor are due to acute laryngotracheal edema and are successfully managed with systemic corticosteroid therapy.4 ENT assessment is often reserved for refractory or acutely life-threatening cases. The aim of this assessment is to distinguish between laryngeal swelling and obstructive granulation tissue formation (Fig. 29.2) or structural laryngotracheal deformities to determine whether minimally invasive surgery can help with critical care step-down and the degree of urgency of such treatment5 and whether the patient is likely to require post-discharge follow-up.

Figure 29.2 Examples of acute intubation-related obstructive airway injuries.
The newly developed stenosis manifesting following decannulation represents a particularly hazardous clinical scenario in that a newly developed stenosis may acutely compromise an airway that is no longer protected in a patient whose diminished physiological reserve immediately following critical illness predisposes them to rapid decompensation which may readily prove fatal. A standard flexible nasoendoscopy is not an inadequate examination, and detailed visualization of the airways from the supraglottic larynx to the carina either endoscopically or radiologically is mandatory to rule out an acute stenosis or obstructive laryngotracheal edema. A flow-volume loop examination in cooperative patients is also highly desirable in these cases.
Outcome Assessment in Laryngotracheal Stenosis
Under physiological conditions it is the performance of the cardiovascular system and not the respiratory system that limits exercise capacity. The principal objective of laryngotracheal reconstruction is therefore long-term restoration of a prosthesis-free airway whose reconstructed dimensions do not constrain the ventilatory demands of the patient while maintaining good phonation and a safe swallow. The four domains in which treatment efficacy can be assessed are anatomy, physiology, symptoms, and quality of life. Systematic documentation of occurrence and severity of disease or treatment-specific complications is also critical for assessing treatment efficacy (Table 29.2).
Treatment durability can be assessed by measuring the intertreatment interval, but this can only be meaningfully done for individual pathological disease processes. For example, idiopathic subglottic stenosis and Wegener granulomatosis are intrinsically recurrent disease processes. Deciding between what “treatment failure” is and what is treatment for recurrence of an intrinsically recurrent disease can therefore be difficult. By contrast, intubation-related airway stenosis is in most cases a nonrecurrent disease process that can be expected to be “cured” by surgery. Posttreatment recurrence in the intubation-related stenosis can therefore be considered a true treatment failure.
Assessment of Airway Anatomy
The most commonly used system for assessing stenosis anatomy is the Myer-Cotton grading system.6 This system is based on the degree of cross-sectional lumen encroachment. Grade I lesions encroach in between 0 and 50% of the lumen, grade II lesions obstruct between 51 and 70% of the lumen, grade III lesions obstruct between 71 and 99%, and grade IV lesions cause total lumen obliteration. This system was initially developed for assessing the subglottis in children, but has since been expanded to encompass tracheal lesions in both children and adults. More recently, Freitag et al proposed a more detailed descriptive system for assessing the nature and extent of tracheobronchial stenoses (Fig. 29.3).7
Table 29.2 Disease-Specific Complications in Laryngotracheal Stenosis
• Nature of complication ○Wound/stent-suture infection ○Deep neck sepsis ○Aspiration pneumonia ○Chest infection ○Major vessel injury ○Pressure sore ○Pneumothorax ○Hemothorax ○Respiratory arrest/acutely life-threatening event ○Stent fracture or migration ○Significant sudden worsening of symptoms requiring admission ○Bleeding ○Severe pain ○Unplanned admission for medical therapy (steroids, mucolytics, etc.) ○Sedation withdrawal ○Other • Severity grading for complications ○0: No adverse event ○1: Mild adverse event (minor no specific intervention) ○2: Moderate adverse event (minimal intervention) ○3: Severe and undesirable adverse event (significant symptoms) ○4: Life-threatening or disabling adverse event (need for intensive care or invasive procedures) ○5: Death related to adverse event |
In 1992, McCaffrey proposed a different system which was based on the site of involvement.8 McCaffrey divided stenoses into four groups based on the length of the lesion and on whether or not the glottis was involved (Fig. 29.4). The classification was validated against actuarial time to decannulation.
In our experience the four key prognostic factors are the nature of the underlying disease process, presence of acute fibroinflammatory stenoses as opposed to mature fibrotic strictures (Fig. 29.5), site of the stenosis, and in particular whether the glottis is involved, and vertical height of the lesion (Fig. 29.6).3,9 Details of our approach to anatomical airway assessment are provided in Table 29.3.
Some years ago we developed a system for quantitative endoscopy to determine the precise degree of luminal obstruction as an assessment method and an outcome measure.10 There had been previous and subsequent efforts by other workers to achieve the same objective and in particular, the computed tomography-based “laryngotracheal profile” by Kiesler et al provides a most eloquent approach to assess airway dimensions (Fig. 29.7).11–13
We have, however, subsequently found detailed assessment of cross-sectional airway anatomy to be unnecessary and have reverted to using the Myer-Cotton system (Table 29.3). The reason for this is the nonlinear relationship between the degree of cross-sectional stenosis and symptoms. It has long been known that most patients are asymptomatic or minimally symptomatic for prolonged period but suddenly develop severe clinical symptoms and need to be operated on urgently.
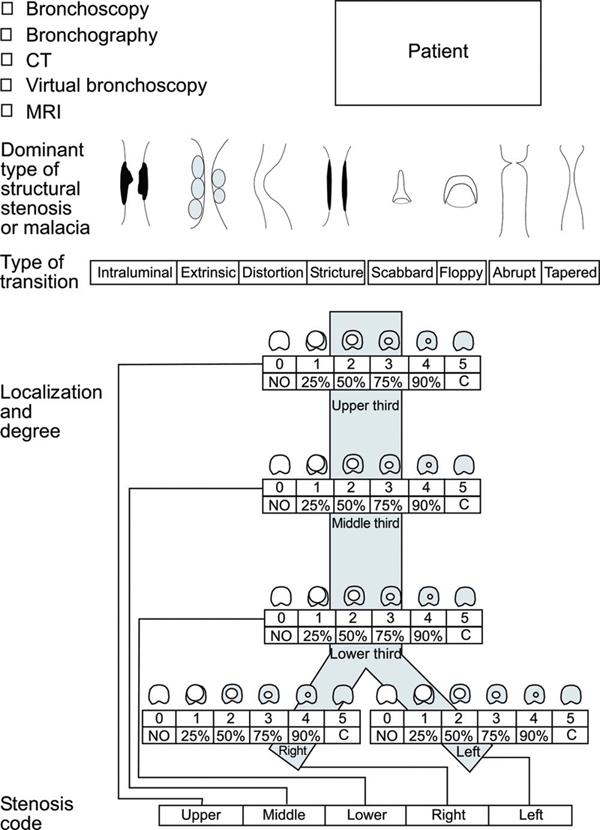
Figure 29.3 Freitag system for documentation of stenosis severity.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


