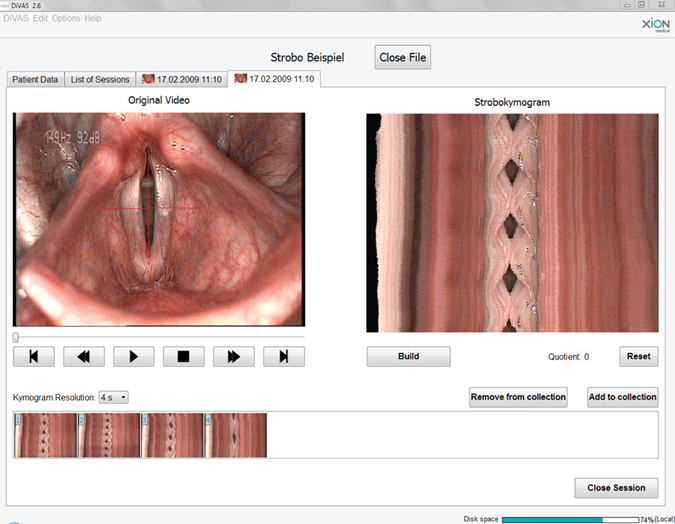
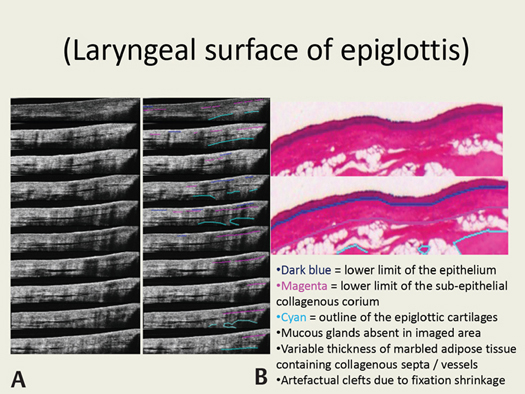
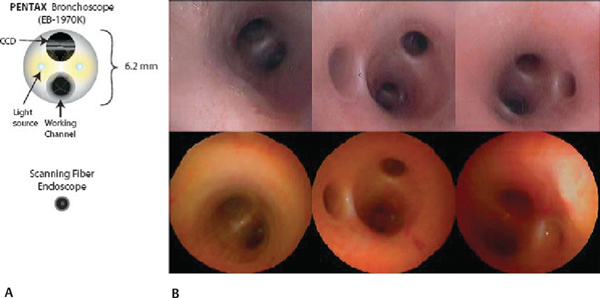
39 Recent Advances in Laryngology and Laryngology Research The technological revolution witnessed toward the end of the last millennium has exploded into a new evolutionary era for the 21st century, which holds great promise for global health care delivery and patient care. Our everyday lives are being transformed through developments in fiberoptics technology allowing faster broadband, multimedia telecommunications, as well as more powerful computers facilitating advanced software processing and extraordinarily large digital data management. Medical research has sought to harvest new technological tools in this fertile climate providing promise for innovative, newer methods for disease diagnosis and management. In good tradition, laryngological research has kept abreast of developments and indeed, on many fronts, continues to pioneer and lead the way providing direct and obvious health care improvements. Multidisciplinary research collaborations, crossing geographical as well as disciplinary boundaries, linking public health care providers, academic institutions, and industrial partners, are allowing fusion of ideas and visions with realization of new technological applications in both laryngeal disease diagnostics and therapeutics. Recent advances have been particularly significant in digital endoscopic imaging of the larynx; adjunctive endoscopic imaging modalities; molecular biomarkers in the context of understanding laryngeal disease processes, diagnosis, and treatment; laser technology in laryngeal surgery; and transoral robotic surgery extending to the larynx. All areas are poised for significant further research and adoption of innovative applications, which may be accelerated still further by emerging nanotechnology applications. Observations from examination of the human larynx with dental mirrors were first published over 150 years ago1 and there has been an enormous development in laryngeal imaging since then. Multiple fiber bundle imaging was first described by Hopkins and Kapany2 from work done at Imperial College London, United Kingdom. Use of the “Hopkins” rigid glass rod with side illumination has since revolutionized minimal access surgery applications across the surgical spectrum, not least in laryngology. Flexible fiberoptic imaging has developed along the same principles of coherent light bundles transmitting image information from a distal illuminated object and image clarity has progressively improved with technological developments including the arrival of analogue charge-coupled device (CCD) and more recent complementary metal-oxide-semiconductor (CMOS) camera image sensors, which have been incorporated into the distal tip of endoscopes to allow high definition, high resolution, still and video digital imaging. Camera stack systems are produced by several manufacturers, with a variety of advanced imaging techniques for more detailed examination of the larynx, providing the potential for objective measurements of voice quality and vocal cord function, as well as adjunctive diagnostic information of tissue structure and nature.3–5 Video-stroboscopic evaluation has gained popularity over the past 25 years among laryngologists and speech pathologists, providing qualitative and quantitative data on vocal cord function, both in the presence and absence of vocal cord pathology.6 Subtle diagnostic information missed by the unaided, naked eye, provides extra information to assist in further management and response to treatment. Video strobokymography has emerged7 to build upon the limitations of simple video stroboscopy, providing quantitative measures of motion and geometry of vocal folds, allowing objective information for planning treatment and monitoring progress over time. Video strobokymograms illustrate a temporal image log of cord appearance and behavior, composed of multiple lines of interest from successive recorded frames of stroboscopic digital video images. To create a kymogram, one (and always the same) line perpendicular to the glottis axis is taken from each image and together combined into a new image showing the time course of fold vibrations (Fig. 39.1). The wave of the mucous membrane and a clear open–close phase is recognizable allowing quantitative calculations in the context of observing cord function in health and disease.8 With the new generation video kymographic and high-speed larynx imaging systems, two CCD sensors are used to provide simultaneously a high-definition color laryngoscopic image and a high-speed kymographic image for clinical vocal fold examination.9 XION Medical (Xion GmbH, Berlin, Germany) has developed an innovative digital video archiving and evaluation system, which is user-friendly, facilitating ready digital data archiving for modern electronic record keeping. Images and video from different patient episodes can be compared on adjacent windows on the same screen allowing more objective comparison of changes in laryngeal appearance temporally. With increasing and larger number patient datasets being established, in the context of accepted high-speed laryngeal imaging clinical protocols and the regular clinical use of this tool, the characterization and discrimination power of the parameters can be explored by applying powerful data analysis techniques to see if automated discrimination between various laryngeal disorders (and stages of disorders) can be established. Data continue to build demonstrating advantages and limitations with increasing use of these laryngeal imaging methods.8 Figure 39.1 A video strobokymogram example taken from the EndoSTROB device from XION Medical. Printed with permission from SheffMed, United Kingdom. Other developments in endoscopic laryngeal imaging relate to emerging adjunctive optical imaging techniques attempting to exploit various properties of light, utilizing broad and narrow-band light spectra. Research has been proliferative in several related areas of this technology, with the door slowly opening to a new era of high resolution, high accuracy (sensitivity and specificity) endoscopic imaging, which shall transform clinical diagnostics and therapeutics in laryngology, as well as a whole host of other medical disciplines and organ systems. On the back of developments in fiberoptics, optoelectronics, applied medical optics, and photonics research, with much more powerful laser and other light sources and increasingly cheaper and miniaturized components, several potential endoscopic technologies have emerged, providing adjunctive endoscopic tools to aid the clinician in laryngeal diagnostics and therapeutics. Optical coherence tomography (OCT)10 is an emerging technology first reported for cross-sectional retinal imaging in 1991. To date, its regular use has been adopted mainly in the ophthalmology community, although with technological developments in the past 10 years, its potential for endoscopic application has been explored and adjunctive benefit slowly realized for other organ systems such as the larynx.11 It offers a noninvasive way to visualize laryngeal tissue architecture (optical biopsy), using low-power infrared light with interferometry in an analogous way to ultrasound, with collection of back-scatter reflections at tissue layer interfaces. Up to micrometer level, resolution of morphological detail is possible, allowing a penetration depth of 2 to 3 mm into tissue. Its potential benefit as a diagnostic or therapeutic adjunct for office and theater-based clinical application in laryngology is slowly being realized as more and more preclinical and clinical studies are being reported.12–16 Even minimal scarring from traditional glottic lesion biopsies may result in functional voice problems that do not resolve; an “optical biopsy” method would be an appropriate development for the larynx. Wong et al13 reports on in vivo experience using a handheld OCT probe in near or gentle contact with mucosa, for adjunctive examination of patients’ larynges while under general anesthesia (normal and benign laryngeal pathology), demonstrating and confirming the findings of ex vivo laryngeal studies12 that OCT images compare favorably with conventional histopathology. The thickness of laryngeal mucosa in various subsites is demonstrated in detail with tissue architecture clearly displaying epithelial from subepithelial layers, integrity of basement membrane, as well as microstructural features such as submucosal glands, ducts, blood vessels, and cartilage. Benign true vocal cord pathology imaged included Reinke edema, polyps, nodules, papillomatosis, mucous cysts, and granulation tissue. Others have added to this work demonstrating the ability for fiberoptic OCT to demonstrate basement membrane violation in invasive laryngeal carcinoma, as well as identify tissue transition zones at premalignant margins of cancer. These findings were limited to superficial lesions as opposed to bulky exophytic growths where tissue penetration would be inadequate to allow the basement membrane to be seen. Just et al17 reported favorably on their unit’s experience applying intraoperative OCT adjunctively to the operating microscope to define biopsy site location and resection planes precisely. Its potential for office-based application as an adjunct to flexible fiberoptic nasendoscopy for the awake patient under topical local anesthesia has recently been demonstrated utilizing a miniaturized endoscopic OCT probe passed in tandem to a flexible nasendoscope to view the larynx.15 Rubinstein et al16 have recently presented their experience of intraoperative OCT imaging of benign and malignant disease conditions using the first commercially available OCT imaging system for upper aerodigestive tract imaging that confirm earlier findings and provide further reliable intraoperative information to guide surgical biopsies, intraoperative decision making, and therapeutic options for various pathologies and premalignant laryngeal disease. Figure 39.2 Detailed ex vivo optical coherence tomography (OCT) images versus hematoxylin and eosin (H&E) correlation: (A) A series of OCT images, which are vertical slices (B-scans) into the epiglottis at different lateral positions. (B) H&E images from the same specimen processed after OCT imaging. Printed with permission from Tadrous P, Tatla T, Cernat R, Podoleanu A. Histopathological correlation of optical coherence tomography (OCT) images of the human larynx ex vivo. J Pathol 2012;226(S1):S.20. Endoscopic OCT has been realized for laryngeal application, a result of imaging systems becoming cheaper and more portable, opening up potential in vivo application in the laryngologist’s clinic and operation theater. Further validation work continues in this context for more accurate histological validation of ex vivo and in vivo laryngeal OCT image data, as well as development and in vivo testing of miniaturized endoscopic and handheld OCT probes with higher resolution and faster axial scan acquisition rates (Fig. 39.2).18,19 Increased data acquisition rates shall generate very large OCT datasets that will require parallel improvements in digital data storage and analysis capabilities. Further improvements in instrument design and endoscopic OCT technology are on the horizon and the future holds strong promise for office-based cancer disease screening and real-time “smart surgery” be it endoscopic, microsurgical or transoral robotic application in the larynx. Various adjunctive imaging modalities have been researched, adopted, and promoted in recent years by some of the major manufacturers of endoscopic imaging systems5,20,21 in attempt to improve upon the diagnostic accuracy of high resolution, “white-light” imaging alone. Various organ systems have been studied extensively with several studies reporting individual unit’s local experience in using these systems for laryngeal diagnostics. Natural cellular fluorophores, such as flavin mononucleotide (FMN), exist as metabolic coenzymes in normal cells for aerobic glycolysis, but not in the anaerobic glycolysis pathways utilized by neoplastic cells.22 Tissue autofluorescence is the natural capacity for tissue to fluoresce when exposed to light of a certain wavelength. Typically, filtered blue light excitation of oxidized FMN and other natural cellular fluorophores in normal cells emits a green fluorescence which can be imaged and amplified by sensitive camera systems in real time. Normal tissue appears green, whereas precancerous (dysplastic) or cancerous tissue does not autofluoresce and appear as darker fields (reddish/violet).23 Indirect autofluorescence laryngoscopy21,23 and flexible autofluorescence endoscopy20 have shown increased sensitivity for diagnosis of premalignant and malignant laryngeal lesions when used as an endoscopic adjunct to “white-light” illumination, improving sensitivity levels to around 90% (a statistically significant increase of 12%).23 Zargi et al24 showed specificity to be lower at 71%, the findings of which were mirrored by others23 due to some benign lesions displaying a loss of green fluorescence. Various groups have reported their findings exploring the potential additional benefits to autofluorescence in applying aminolevulinic acid (ALA) topically to the laryngeal mucosa, to preferentially induce fluorescence within neoplastic cells. Conflicting results have been noted as to whether ALA-induced fluorescence spectroscopy adds any further diagnostic accuracy to autofluorescence alone in the larynx, particularly in the context of laryngeal dysplasia and carcinoma.25 Narrow band imaging (NBI) is a novel, high-resolution endoscopic technique used widely to aid diagnosis of intestinal lesions, which has recently been investigated in vivo for suspected laryngeal lesions to differentiate precancerous and malignant laryngeal lesions.5,26 The modality is based on the fact that the depth of light penetration depends on the light wavelength; the longer the wavelength, the deeper the penetration. NBI modifies the broadband white light of a xenon lamp into two narrow band beams with central wavelengths of 415 (narrow band blue) and 540 nm (narrow band green) (designed primarily to penetrate mucosa and submucosa). When used in combination they provide high surface contrast, displaying morphology of superficial capillary networks and subepithelial vessels for in vivo differentiation of nonmalignant from malignant laryngeal lesions. Ni et al5 demonstrated that utilizing white light modes and NBI modes during office-based flexible nasendoscopy with topical local anesthesia, sensitivity of 88.9% and specificity of 93.2%, respectively, is achieved in detecting malignant lesions; significantly superior to white light illumination alone. Raman spectroscopy provides information about molecular composition and structure and it too has been investigated ex vivo as a potential tool for noninvasive optical tissue diagnosis in the larynx.27,28 Inelastic light scattering following excitation of target tissue using monochromatic laser light can be detected and analyzed to determine Raman spectral data, a unique molecular signature of the material. It was first described by the Nobel Prize winner Raman in 1928.29 Good quality spectra have been obtained with ex vivo laryngeal specimens. Lau et al28 described 5-second acquisition times, showing spectral tissue characterization and predictive sensitivities (89, 69, and 88%, respectively) and specificities (86, 94, and 94%, respectively) for normal tissue, carcinoma, and papilloma. Stone et al27 described prediction sensitivities of 83, 76, and 92%, with specificities of 94, 91, and 90% for normal, dysplastic, and squamous cell carcinoma of the larynx, respectively. These studies support the potential for future in vivo endoscopic studies. Rigid contact endoscopy30,31 and confocal endoscopy25,32 are two associated techniques that allow the surgeon to see magnified optical cellular detail in vivo of superficial tissue surfaces; studies on the normal and diseased larynx have been described in recent years but show various limitations including poor depth penetration and difficulty visualizing the basement membrane. Other “noninvasive” in vivo optical imaging modalities are still very much in early development and presently mostly limited to research and observations on biological processes in preclinical models.33 Of particular note, however, scanning fiber endoscopy is an emerging versatile technology for ultrathin flexible endoscope application which holds great promise.34 It uses a single-mode optical fiber with active laser light scanning of tissue, allowing high resolution and large field of view imaging with much smaller diameter flexible endoscopes (Fig. 39.3). The reduced size increases furthermore the potential for developing “smart” endoscopic tools that have adjunctive optical arrangements coupling high-quality video imaging with subsurface tissue interrogation and high-resolution fluorescence imaging. The clinical application of OCT and other endoscopic imaging modalities can be advanced further by utilizing tissue contrast and spectral data provided by disease-specific biomarkers.11,35 Molecular imaging capabilities are poised for clinical translation in coming years, providing adjunctive disease-specific information to improve further the accuracy of any “optical biopsy” tool. Molecular imaging strategies fall into two categories: (1) endogenous molecular imaging, involving direct imaging of endogenous biomolecules, and (2) molecular contrast-imaging, involving exogenous contrast agents introduced in vivo to bind specifically to biomolecules of interest. Contrast may involve near-infrared activated fluorescently labeled antibody probes, or indeed other labeling reagents coupled to antibody probes such as submicron microspheres or nanoparticles incorporating nontoxic materials such as gold or iron oxide.11 Presently, these are experimental only; once validated ex vivo and in preclinical animal models, they will need to undergo human trials to assess their clinical validity and safety profile. Printed with permission from Wiley-VCH Verlag GmbH & Co. KGaA. Lee CM, Engelbrecht CJ, Soper TD, Helmchen F, Seibel EJ. Scanning fiber endoscopy with highly flexible, 1 mm catheterscopes for wide-field, full-color imaging. Biophotonics 2010;3(5–6):400.
Advances in Endoscopic Imaging Systems for Laryngology
Adjunctive Endoscopic Optical Imaging Techniques
Optical Coherence Tomography in the Larynx
Related Adjunctive Optical Imaging Modalities in the Larynx
Application of Molecular Biomarkers in Laryngology
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


