Otoplasty
- Prominauris (prominent ears) occurs in approximately 5% of the population.
- Conchal prominence and the absence of an antihelical fold represent the most common causes of prominence of the ears.
- Although there are hundreds of techniques to correct auricular prominence, the most common are suture techniques for conchal setback (technique of Furnas) and for creation of an antihelical fold (technique of Mustarde).
- Otoplasty refinement techniques exist for deformities such as large earlobes and excessive helical prominences.
- Complication rates from otoplasty range from 7% to 12% and may be subdivided into early, late, and aesthetic/anatomic in etiology.
- Auricular hematoma occurs in 1% of otoplasties. Complaints of unilateral pain or tightness within the first 48 hours postoperatively require prompt removal of dressings to examine the wound site for hematoma collection.
The incidence of excessively prominent ears is about 5%. It is inherited as an autosomal dominant trait with 25% partial penetrance; it most commonly results from two anatomic irregularities, specifically the absence of an antihelical fold and excessive depth or projection of the conchal bowl.
Precise analysis of auricular deformities is paramount to achieving successful outcomes. Surgeons must identify the specific cause of auricular prominence in the formulation of an appropriate surgical plan. Although frequently bilateral, asymmetries in ear protrusion should be noted. As such, standard preoperative photography should be performed, including frontal, full right and left oblique, full right and left lateral, and close-up right and left lateral views.
Although there exist proponents of earlier surgical correction, most authors agree that the ideal age for otoplasty is between 5 and 6 years. Physiologically, the auricle is roughly 90% of adult height by 6 years of age. Psychosocially, correction is undertaken before or soon after a child’s entrance to grammar school, where children are subject to peer ridicule. Moreover, by 5 or 6 years, children are able to participate in their own postoperative care (ie, not pulling off bandages or disturbing the wound).
Over 200 techniques have been described for correction of the prominent ear. Conceptually, they can be subdivided into procedures that address an absent antihelical fold, procedures that reduce excess in the conchal bowl, and those that reduce prominent or enlarged lobules. Most of the latter techniques involve reshaping auricular cartilage, which can be accomplished through a number of cartilage-manipulating techniques such as suturing, scoring, and excision/repositioning, to name a few. Herein, the most commonly used technique for correction of an absent antihelical fold, originally described by Mustarde, is discussed in greater detail. In addition, the Furnas technique for reduction of an excessive conchal bowl is described.
In 1963, Mustarde first described a technique for creating an antihelical fold by using permanent conchoscaphal mattress sutures. Since that time, many subtle refinements of this technique have been described, but the fundamentals of the procedure remain unchanged.
Pediatric patients most commonly undergo general anesthesia for this procedure, and perioperative broad-spectrum antibiotics are administered. The face is prepped into a sterile field such that both ears can be visualized simultaneously. After infiltration with lidocaine 1% with epinephrine 1/100,000, an eccentric fusiform incision is made into the postauricular surface. Typically, more skin is excised from the postauricular surface than from the mastoid, in an effort to camouflage the resultant scar into the postauricular sulcus following setback.
Once the fusiform of skin is excised, the remaining skin of the posterior aspect of the helix, antihelix, and concha is undermined with scissors, leaving perichondrium attached to the auricular cartilage. The extent of antihelical fold creation is determined by pinching the anterior auricle with a thumb and index finger. Alternatively, some surgeons mark cartilaginous landmarks with several ink-dipped fine needles. Permanent horizontal mattress sutures (eg, 4–0 Mersilene [Ethicon, Inc., Somerville, NJ]) are placed into the helical cartilage, parallel with the helical rim at the lateral extent of the desired antihelical fold (Figure 79–1). It is critical that sutures are placed through the cartilage and lateral perichondrium but not the lateral helical skin. The first helical suture is placed at the level of the helical root to create the superior crus. The second suture is typically placed just inferior to the junction of the superior and inferior crura. Third and fourth sutures are placed as needed. Some overcorrection is necessary during placement of the most superior suture, because it has been demonstrated that as much as 40% loss of correction at this site may occur within the first postoperative year.
Figure 79–1.
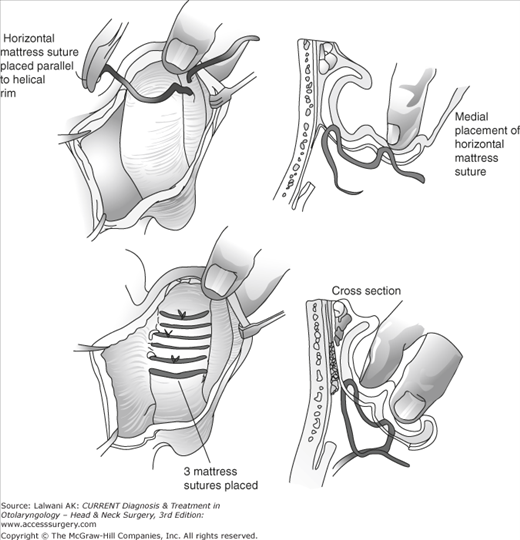
Technique of Mustarde for creation of the antihelical fold—three permanent horizontal mattress sutures are placed parallel with the helical rim. Care is taken to place sutures through the anterior perichondrium without violating the anterior skin. (Reproduced, with permission, from Adamson PA, Constantinides MS. Otoplasty. In: Bailey BJ, Calhoun KH, Coffey AR, Neely JG, eds. Atlas of Head & Neck Surgery—Otolaryngology. Philadelphia: Lippincott-Raven, 1996:429.)
The wound is irrigated with antibiotic solution and closed with resorbable sutures. Antibiotic ointment, along with cotton impregnated in mineral oil, is applied to the new antihelix and postauricular sulcus, and a mastoid dressing is applied.
The dressing is removed on the first postoperative day to check for hematomas, and replaced for 3–4 more days. Subsequently, a head band is worn continuously for 2 weeks and at night for an additional 4–6 weeks.
In 1968, Furnas popularized a technique of conchal setback using permanent conchomastoidal suturing. This procedure is often undertaken in conjunction with techniques to correct an absent antihelical fold, as described above.
The patient is prepped and draped in a manner similar to that described for correction of the antihelical fold. After infiltration of lidocaine 1% with epinephrine 1/100,000, a fusiform incision is made in the postauricular region. The width of the incision is estimated by manually pushing the concha toward the mastoid. Care is taken to avoid excessive skin excision, since tension on the wound predisposes to hypertrophic scar formation. Little to no skin excision is required inferior to the level of the antitragus. After excision of skin, soft tissue and postauricular muscle are excised from the postauricular sulcus. Sufficient soft tissue is excised to produce a pocket that will receive the concha during suture placement.
The skin over the helix, antihelix, and concha is undermined with scissors, and permanent horizontal mattress sutures (eg, 4–0 Mersilene [Ethicon, Inc., Somerville, NJ) are placed at the lateral third of the concha cavum and concha cymba parallel with the natural curve of the auricular cartilage (Figure 79–2). The sutures are thrown through cartilage and lateral perichondrium, but not lateral auricular skin. At least three sutures are placed for adequate setback. The sutures are placed on what was the ascending wall of the concha and, when tightened, convert the wall into a longer floor of the concha. For long-term successful conchal reduction, suture bites of mastoid periosteum must be taken. With extremely thick cartilage, as frequently seen in older persons, the cartilage may be weakened by excising small vertical ellipses of cartilage. It is important for the conchomastoidal sutures to allow the concha to be set not only medially but posteriorly. If not, external auditory canal stenosis can result.
Figure 79–2.
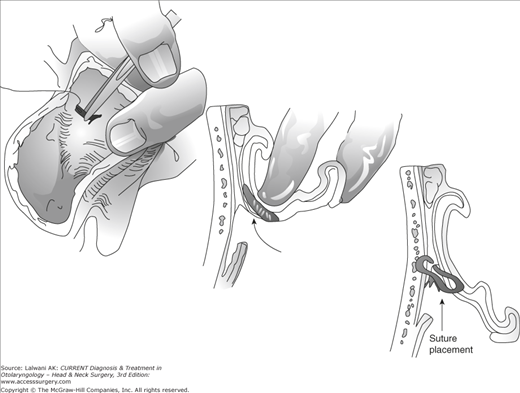
Technique of Furnas for correction of conchal excess. Permanent conchomastoid horizontal mattress sutures are placed at the lateral third of the concha. A full-thickness bite of cartilage and perichondrium is performed, with care taken to avoid suture placement through the anterior skin. In addition, the sutures must pull the ear posteriorly as well as medially to prevent stenosis of the external auditory canal. (Reproduced, with permission, from Adamson PA, Constantinides MS. Otoplasty. In: Bailey BJ, Calhoun KH, Coffey AR, Neely JG, eds. Atlas of Head & Neck Surgery—Otolaryngology. Philadelphia: Lippincott-Raven, 1996:429.)
The wound is irrigated and closed as after the Mustarde technique. A mastoid dressing is placed, and subsequent postoperative management is the same as that of antihelical fold surgery.
Frequently, small deformities of the auricle are present that can be corrected by subtle surgical refinements. These techniques are applicable to both congenital irregularities and deformities that are detected after more substantial otoplasty correction (ie, conchal setback and correction of absent antihelical fold). Such refinements include correction of the prominent lobule and reduction of helical prominences.
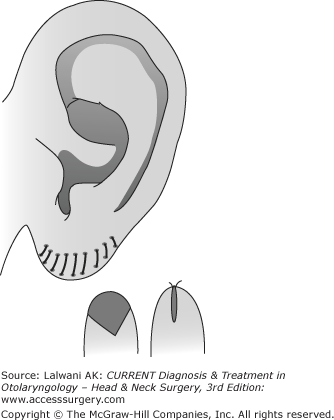
Reduction of a large ear lobule rarely requires general anesthesia in the adult population. A new earlobe size is designed with a marking pen. After infiltration with local anesthesia, a fusiform incision is made anteriorly and posteriorly in a curvilinear fashion, and a V-shaped, wedge excision of lobule excess is performed (Figure 79–3). The skin is closed with permanent suture (eg, 6-0 nylon), with suture removal occurring on the sixth postoperative day.
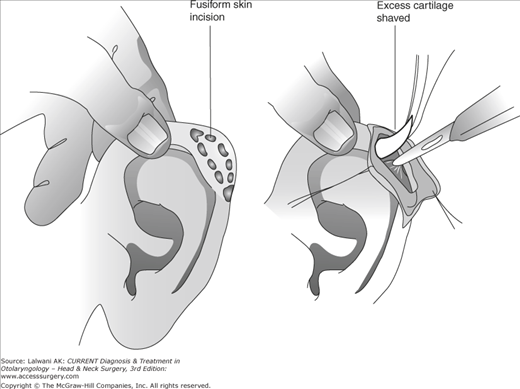
Helical prominences, such as superior outer helical rim cartilage excess (ie, elf ears, Spock ears) and superior helical fold cartilage excess (ie, lop ear), may be corrected by a variety of helical reduction techniques. After the infiltration of local anesthesia, a fusiform incision is made on the outer helical rim in the case of helical rim excess and under the helical fold in the case of superior helical fold excess (Figure 79–4). After skin elevation, excess cartilage is shaved using a blade. Skin is trimmed as necessary to ensure appropriate draping over the cartilaginous rim. The incision is closed with permanent suture (eg, 6-0 nylon), with suture removal occurring on the sixth postoperative day. No pressure dressing is required.
Overall, there is a high satisfaction rate among patients who undergo otoplasty surgery (85%). Complication rates range from 7% to 12%, with unsatisfactory aesthetic outcomes accounting for the majority of complications. Complications arising from otoplasty may be subdivided into early, late, and aesthetic/anatomic in etiology (Table 79–1).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


