14 Otological Nerve Surgery Otorhinolaryngology deals with all twelve cranial nerves. Clinical and electrophysiological examinations for the diagnosis of related nerve diseases—ranging from the diagnosis of olfactory nerve impairment and decompression of the ophthalmic and oculomotor nerves, to diagnosis and management of the caudal nerve group—have become routine in larger ear, nose, and throat departments. Otological nerve surgery has also come into favor in connection with otological surgery of the temporal bone (Table 14.1), focusing on cranial nerves VII to XII (the facial, vestibulocochlear, glossopharyngeal, vagus, accessory, and hypoglossal nerves). Otosurgeons therefore need to have a precise knowledge of the physical and electrophysiological diagnosis of motor nerve dysfunction. In addition, there are four important procedures that need to be learned and carried out for several indications: nerve decompression and transposition; neurectomy; end-to-end nerve suturing; and interposition of free nerve grafts.
| Nerve decompression and transposition Nerve section Nerve suture and grafting Neuroma surgery on nerves VII-XII |
 Diagnosis of Motor Nerve Dysfunction
Diagnosis of Motor Nerve Dysfunction
The otorhinolaryngologist is mainly concerned with peripheral palsies of the facial and recurrent laryngeal nerves, and less often with lesions of the glossopharyngeal, vagus, and hypoglossal nerves. In ear and temporal bone surgery, the focus is on diagnosing facial nerve lesions, since these may involve emergency otosurgical indications.
A physical examination of the facial nerve can easily distinguish between central palsies (with persistent innervation of the frontal muscle) and peripheral (nuclear or infranuclear) lesions. However, differentiation between complete (paralysis) and incomplete (palsy) dysfunctions is often made difficult when there is apparently voluntary lid closure, which can even be observed after transection of the nerve trunk. This phenomenon is explained by an automatic silent period (relaxation) of the antagonistic levator palpebrae muscle, innervated by the oculomotor nerve.
Electrophysiological methods alone are appropriate for distinguishing between the three main classes of peripheral nerve dysfunction (Seddon 1972), for which Sunderland (1982) described the morphological basis:
- Neurapraxia. This is a functional block of nerve conductivity, caused by transitory alterations in the myelin sheath, but with preservation of the axon cylinder.
- Axonotmesis. This is a local necrosis of the neurite, with subsequent descending Wallerian degeneration, but with preservation of the nerve cord, and it is usually followed by regeneration, with sprouting of the axon cylinders along the Büngener’s bands (Ledbänder). Axonotmesis can be combined with neurapraxia, limited to a percentage of the thousands of nerve fibers, or it can be total. The proportion of fibers affected will determine the extent and time period of recovery: days or weeks for neurapraxia, months for axonotmesis.
- Neurotmesis is the term for a discontinuation of the nerve cord. Spontaneous regeneration without nerve suturing cannot be expected.
Carrying out the simple nerve excitability test (electrical, inadequate stimulation of the facial nerve at the stylomastoid foramen, with observation of any visible reaction in the facial muscles), is not reliable for the above task. Nor can electroneuronography (using surface electrodes to record a cumulative muscle action potential during electrical stimulation of the facial nerve trunk) provide reliable information. Fisch’s hypothesis that the amplitude reduction in voltage is more or less equivalent to the percentage of facial nerve degeneration is not acceptable, due to the non-linearity of amplitudes relative to the number of nerve fibers. Our own experience with electroneuronography was disappointing, due to frequent unresponsiveness to testing in spite of fast recovery of nerve function.
Only electromyography (EMG) with needle electrodes is able to trace rare action potentials and is therefore capable of identifying whether there is a persistent and untransected nerve cord (Fig. 14.1). EMG can also demonstrate both incipient degeneration, with the occurrence of fibrillation potentials or positive sharp waves, and the onset of regeneration of necrotic nerve axons within a preserved nerve cord or through an interposed nerve autograft (Fig. 14.2). EMG can provide representative information about the status of the actual spontaneous or stimulated electric activity of the facial muscles, but if there is complete electrical silence it is of no assistance in deciding between the alternative diagnoses of neurapraxia (transitory functional block) or axonotmesis (degeneration), nor can it provide information distinguishing between axonotmesis and neurotmesis. Despite these limitations, electromyography has become an indispensable tool in otological nerve surgery. Along with modern imaging modalities, it provides the basis today for all the indications mentioned, and allows clear documentation of nerve recovery or functional nerve repair.
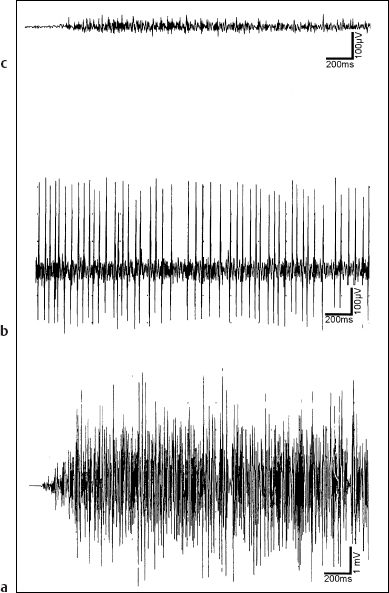
Fig. 14.1 Electromyography with needle electrodes for peripheral facial nerve palsy. a The interference pattern seen in normal voluntary motor activity. b The rare finding of voluntary action potentials, indicating moderate paresis, but showing continuity of the nerve cord. c Remote voluntary activity (“endplate noise”).
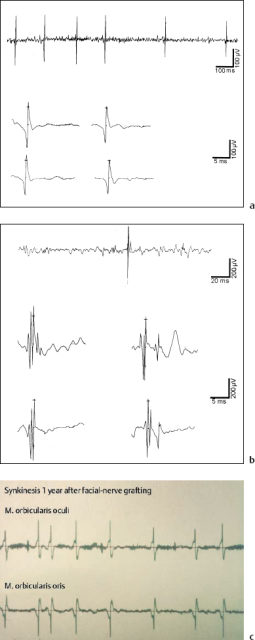
Fig. 14.2 Electromyography for degenerative facial nerve paralysis. a The involuntary sequences of low-voltage spikes (fibrillation potentials) indicate progressive degeneration of axons (axonotmesis). b The high-amplitude multipolar spikes (giant potentials) document new, irregular connections between motor muscle fibers and new motor units after axonal regeneration. c Synchronous discharge of motor units in distant ipsilateral facial muscles verifies synkinesis after regeneration.
 Nerve Decompression and Transposition
Nerve Decompression and Transposition
The benefits of nerve decompression have been well known for many years. A distinction needs to be made between external and internal compression syndromes. The median nerve compression syndrome and trigeminal nerve root compression by the cerebellar arteries in trigeminal neuralgia are good examples of the damaging effect of external compression forces on a nerve or on its root entry zone. Temporal bone trauma with blunt compression of the facial nerve, or with impalement of bone fragments (see Chapter 5) also belongs to this category. Increased intraneural tissue pressure was attributed to the facial nerve in Bell’s palsy and to inflammatory reactions such as herpes zoster oticus (Ramsay Hunt’s syndrome). These are examples of internal compression. Modern neuro-otosurgery has revived the relevant decompression operations for functional rehabilitation of cranial nerves II, V, VII, and VIII. Some of the classic indications for these operations are described in the following sections.
Facial Nerve Paralysis (Bell’s Palsy)
There is an extensive literature on the indication for, technique of, and results of facial nerve decompression in severe Bell’s palsy. This clinical entity was first described by Friedreich (1797) and later by Bell (1821), and it is characterized by functional palsies without nerve axon degeneration (neurapraxia) or with such degeneration (axonotmesis), of unknown origin. Electromyography has demonstrated that mixed forms, with proportional degeneration of the approximately 11 000 axons (Lang 1997), are frequent. It is assumed that interaxonal edema occurs due to neuritic inflammation or circulatory disturbance, or both, leading to a vicious circle of nerve swelling under the epineurium within the fallopian canal, leading to blockage of the axon sheaths with subsequent cessation of axonal flow and occurrence of axonal damage. Massive avulsion of the nerve is in fact observed after opening the fibrous outer nerve sheath (Fig. 14.3). This phenomenon is prominent near the geniculate ganglion, but it can also be seen in the mastoid portion of the nerve. Although Wullstein (1958) originally recommended decompression of this vertical portion caudal to the labyrinth, Fisch (1981) has repeatedly emphasized that the most important site to decompress is the supralabyrinthine portion.
Since the introduction of intravenous high-dose corticosteroid therapy for severe Bell’s palsy by Stennert (1979), the number of decompression operations has dramatically decreased.
Fisch based the indication for intervention on the electroneuronographic findings. He attributed linear proportionality in degeneration percentages to the amplitude of the electrically elicited cumulative action potential, recorded by a surface electrode over the facial muscles. The linearity between amplitude and percentage is questionable, and we were also disappointed with the practical results of the test. Too often there was no response in patients who experienced a fast recovery, while in others signs of degeneration became visible despite high amplitudes in the neuronographic examinations. For many years now, we have based our indication on an electromyographic examination of the facial musculature, using at least three unipolar needle electrodes to record voluntary and spontaneous muscle action potentials from the frontal, periocular, and perioral muscles (Wigand 1967). As long as voluntary activity can be observed, a decompression operation is not indicated, even with complete clinical paralysis lasting several weeks. As soon as zero voluntary activity is combined with marked signs of degeneration (fibrillation potentials—which may occur after the second week of paralysis—), in the absence of regeneration potentials surgical decompression must be considered reasonable. Since there have been no controlled clinical studies based on EMG analysis, the controversy over the value of the operation will continue; options discussed range from doing nothing, through corticosteroid monotherapy, to early decompression. In a prospective study, Gantz et al. (1999) showed that over 90% degeneration in electroneuronography (ENOG) with electrical silence in the EMG predicts a 58% chance of poor outcome (House–Brackmann grade III or IV), while middle fossa nerve decompression provides a good outcome (House–Brackmann I and II) in 91% of patients with the same combination of findings. From the pathophysiological viewpoint, one can agree with Bumm’s law that surgery facilitates regeneration while at the same time promoting synkinesis due to incorrect spread (Bumm et al. 1982). From the statistical point of view, early surgery will also help reduce the percentage of nerve fibers that move from neurapraxia to axonotmesis as time goes on.
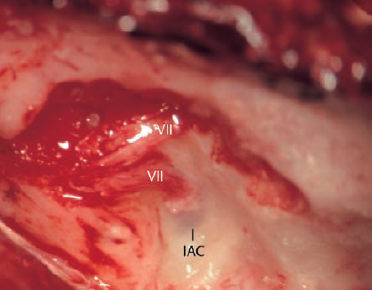
Fig. 14.3 Decompression of the geniculate ganglion and facial nerve via the middle fossa approach for Ramsay Hunt’s syndrome (right ear). After an incision in the epineural nerve sheath, the nerve fibers with edema emerge from the fallopian canal—a very different appearance in comparison with nerve exposures in acoustic neuroma surgery.
VII Facial nerve
IAC Internal auditory canal
In patients with severe facial nerve paralysis and herpes zoster oticus (Ramsay Hunt’s syndrome) we use the same treatment approach as in Bell’s palsy. The only difference is that aciclovir is administered immediately in addition to corticosteroid therapy. It has been alleged that cortisone treatment increases the incidence of herpetic meningitis, but in more than 30 years I have never observed a single patient who developed meningitis after corticosteroid therapy, which Wullstein (1958) was already using at high doses of 80–250 mg prednisolone (Solu-Decortin). On the other hand, since the introduction of aciclovir not a single patient with herpes zoster oticus with facial nerve paralysis has had to undergo a decompression procedure in my department during the last five years.
Apart from Bell’s palsy, trauma to the petrous bone may also represent an indication for nerve decompression.
Surgical Technique of Facial Nerve Decompression
Since, in principle, significant internal compression can be expected in the supralabyrinthine part of the facial nerve, a middle cranial fossa approach is the method of choice. This provides excellent exposure of the fallopian canal from its meatal ostium (the meatal foramen) to the geniculate ganglion and down to its epitympanic portion over the oval niche. The segment between the internal auditory canal and the geniculate ganglion is the narrowest part of the canal. Its curved course lies very near to (1–2 mm from) the basal turn of the cochlea, but it can be precisely identified from above. No other approach provides comparably good exposure of this segment and of the geniculate ganglion, while preserving the integrity of the ossicular chain and of the superior semicircular canal. The nerve should be followed from the meatal foramen beyond the geniculate ganglion into its tympanic portion. If microscopic inspection shows that there are still suspicious changes here, transmastoid decompression of the vertical segment into the stylomastoid foramen can be added.
The transtemporal, extradural approach to the facial nerve and geniculate ganglion is described in Chapter 13. For exploration and decompression of the facial nerve, juxtalabyrinthine bone removal can be confined to the internal auditory canal at its fundus. From here, the fallopian canal is followed to the geniculate ganglion. This is uncovered, and the greater petrosal nerve is identified. Thereafter, the tegmen epitympani is unroofed, and the malleoincudal joint is exposed. Medial to the malleoincudal joint, the bone is carefully removed without causing any injury to the ossicular chain, uncovering the fallopian canal as far as possible. Small diamond burrs are used for all the bone removal.
When the facial nerve has been exposed, its epineurium is slit with a small, curved, and sharp sickle knife. The fibrous sheath of the geniculate ganglion is also opened. After this maneuver, an impression of the extent of the intraneural tissue pressure is obtained if the nerve fibers pour out, with edema from the bony canal. Where they look normal, as is most often the case in the visible part of the tympanum, decompression may end there. Gelfoam soaked in an aqueous solution of corticosteroid is placed over the opened nerve, and wound closure starts.
In patients with longitudinal or transverse temporal bone fractures, with immediate complete paralysis and zero EMG signals, and with CT evidence of a fracture cleft crossing the nerve, microsurgical exploration of the area via the middle fossa approach is indicated. By contrast, a delayed onset of the palsy has a good prognosis without intervention. Fisch (1974) showed that both types of petrous bone fracture cause the maximum of facial nerve injury around the geniculate ganglion. Disruption of the nerve (neurotmesis) is more of an exception. A more frequent finding is impalement by wedged bone chips (Fig. 5.23c) or simply compression by the dislocated bone. Severe degeneration without visible changes in the nerve cord can also be due to sudden stretching. We have always opened the fibrous nerve sheath, with the aim of improving the local circulation.
Wound closure follows the technique used in the middle fossa approach described earlier (pp. 240–241). To avoid broad fibrous scar formation directly on the opened facial nerve cord, a piece of silicone foil with the appropriate shape and size is placed over the nerve and geniculate ganglion, helping at the same time to reinforce the epitympanic tegmen and thereby protecting the ossicular chain from massive cranial adhesions. Postoperative conductive hearing loss must be avoided. If this occurs, a second-stage endaural posterior atticotomy with removal of adhesions is appropriate in order to restore normal hearing. It is important to carry out preoperative audiogram examinations to avoid incorrectly linking post-operative hearing loss to the facial nerve decompression operation.
Neurovascular Decompression for Hemifacial Spasm
Clinical entity. Hemifacial spasm is characterized by spasmodic contractions of the mimic muscles of one side of the face. The contractions can be triggered or facilitated by exposure of the ipsilateral eye to bright light, and by warming the facial skin. At the start of the syndrome, brief twitching of the eyelids occurs, which does not cause the patient any difficulty. Soon, however, sequences of weak contractions develop that become irritating to the patient. Within a few months, the spasms become stronger and more frequent, extend, and involve other groups of facial muscles. In the end phases, almost continuous waves of contractions disfigure the face down to the platysma, and the patients suffer severely during these episodes.
Hemifacial spasm should not be confused with:
- Blepharospasm, a bilateral syndrome of unknown origin with involuntary contractions of the orbicularis oculi muscles. This is also intensified by light and by focusing the gaze.
- Facial tic, which involves automatic bilateral expressive facial movements, due to extrapyramidal disturbances.
- Postparalytic mass movements (synkinesis), which are the result of peripheral nerve regeneration.
Electromyographic recording of voluntary activity and of the spasmodic episodes can clarify this differential diagnosis unequivocally (Wigand et al. 1968, 1972). While blepharospasm and facial tics showanormal interference pattern in the motor neuron potentials, synkinesis is characterized by normal or reduced interference patterns, which are synchronous in their onset at remote recording sites. For example, when the patient is asked to close the eyes, approximately normal potentials will start not only in the ocular musculature, but in the oral musculature as well. Typical of hemifacial spasm is the involuntary appearance of sharply synchronized sequences of bursts in different muscle groups (Fig. 14.4). These do not have interference patterns, but show identical, reproducible patterns within one lead over long periods.
The pathogenesis of hemifacial spasm is a matter of controversy. Esslen (1957) found disturbances of the isolating properties of the nerve fibers, leading to a flash-over of neural discharges from one fiber to another (ephapse), but Jannetta (1985) has favored the earlier view of Dandy (1934) that the cranial nerves are subject to biomechanical irritation from pulsating cerebellar arteries that cross the nerve or its root exit zone. It seems plausible that mechanical influences may cause a motor nerve to become pathologically irritable, and the repeated experience that the spasms resolve after the pressure-exerting vessels have been disengaged from the nerve during decompression surgery has provided support for this interpretation. The surgical procedure is similar to that for decompression of the trigeminal root in trigeminal neuralgia. Appropriate techniques include suboccipital approaches via the posterior cranial fossa, and the enlarged middle cranial fossa approach. Partial excisions of facial nerve branches (Fisch 1972, Miehlke 1973, 1981) appear obsolete.
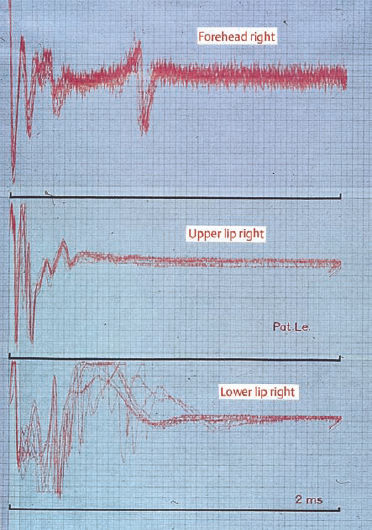
Fig. 14.4 Electromyography in hemifacial spasm (superimposed recording technique). The synchronized bursts of repeated patterns of spikes between different leads are very characteristic.
Conservative Treatment of Hemifacial Spasm
Although neurovascular decompression of the facial nerve can be regarded as treating the cause of hemifacial spasm, the procedure is not indicated for all patients, and some refuse surgery. Primary conservative treatment is reasonable. During the initial stages of the syndrome, advising the patient to avoid bright light and to wear sunglasses can provide some relief. Antispasmodic antineuralgic drugs such as carbamazepine may also help reduce the frequency and severity of attacks.
Inducing mild peripheral myoparesis by subcutaneous injection of botulinum toxin (Botox), a method introduced by Scott (1981) and Laskawi et al. (1994), is a very effective treatment that eliminates the attacks for a period of six to eight weeks. The injection can be repeated, and it is a valuable adjuvant treatment if nerve decompression is not sufficiently successful, or if there are mild recurrences after surgery.
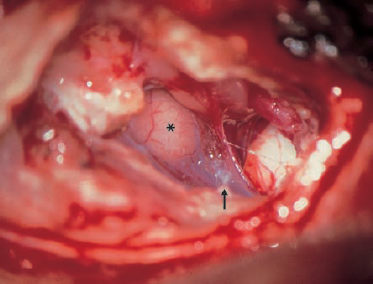
Fig. 14.5 Enlarged middle fossa approach exposure of the internal auditory canal and cerebellopontine angle in a patient with hemifacial spasm (left ear). The facial and vestibulocochlear nerve bundle is attached by fibrous arachnoid adhesions (arrow) to a protruding flocculus (*). The facial nerve is encircled by a thick artery (anteriorly) and there is a thinner artery penetrating between the facial and vestibular nerves.
VII Facial nerve
VIII Vestibulocochlear nerve
SSC Superior semicircular canal
Surgical Treatment by Neurovascular Decompression
Three approaches are appropriate for exposure of the facial nerve and vestibulocochlear nerve within the cerebellopontine angle: the retrolabyrinthine presigmoid approach, the microscopic or endoscopic retrosigmoid approach, and the enlarged middle fossa approach.
Retrolabyrinthine approach. The retrolabyrin thine approach is an otological access route through the mastoid (Silverstein and Norell 1982), the principles of which are described in Chapter 13 (pp. 246–247). The advantage of this technique is that it provides an easy entrance route through the middle ear, but it has considerable disadvantages with limited opening of the cerebellar dura, obscuring of the facial nerve by the overlying vestibular nerve branches, and the impossibility of surveying the facial nerve within the internal auditory canal, where neurovascular conflicts may also be present.
Retrosigmoid approach. The retrosigmoid approach (Janetta 1975, Magnan and Chays 1998) is also described in Chapter 13 (pp. 247–250). The exposure of the cerebellopontine angle is adequate, and vascular complications, hemorrhage, and dislocation can be managed under normal neurosurgical conditions. This is the method advocated by Janetta. The complication rates experienced earlier, with conditions including facial paralysis, total deafness, and vestibular disorders, as well as blindness and neurological deficits, were significantly reduced after this method was introduced. The disadvantages of the technique, with masking of the facial nerve by the flocculus and by the vestibular nerve, and with no inspection of the internal auditory canal, make this technique a difficult one that requires considerable experience.
Retrosigmoid endoscopic decompression. Caces et al. (1996) reported good results with facial nerve decompression in the cerebellopontine angle using a rigid endoscope. Exposure of the cerebellopontine angle and brain stem was achieved using a limited retrosigmoid approach. Anyone who has tried to work with an endoscope in the cerebellopontine angle, with the many large vessels and arachnoid adhesions present there, will be aware how challenging this sophisticated method is.
Enlarged middle fossa approach. Our own preferred technique for facial nerve decompression in patients with hemifacial spasm is the enlarged middle cranial fossa approach. This allows exposure and decompression of the facial nerve between its exit from the pons to its entrance into the fallopian canal. The great advantage of the technique is the prominent position of the nerve in the internal auditory canal when this access route from above is used. The nerve is not hidden by the vestibular nerve or by the cerebellar flocculus. In addition, its exit zone can be clearly visualized with a microscope. Since arterial loops may also compress the facial nerve within the internal auditory canal, this approach is the appropriate method for all possible configurations of vascular oppression. The only disadvantage of the enlarged middle fossa approach in comparison with the suboccipital approaches is its higher cost in terms of operating time and precise bone work. The complication rates are extremely low when the technique is used at centers where it is routine.
Exposure of the cerebellopontine angle for dissection of the facial nerve as it leaves the pons, and exposure of the internal auditory canal, follow the pattern described in Chapters 4 and 13 (pp. 37–39 and 230–241). After refolding the dural flaps and opening the arachnoid, dissection of the facial nerve starts slightly lateral to the first visible crossing artery or vein, not automatically at the fundus. We have often found tight arachnoid adhesions jointly encircling nerves VII and VIII and attaching them to a protruding flocculus, with an artery between the facial and the vestibulocochlear nerve (Fig. 14.5). In other cases, the facial nerve was separately fixed to a thick artery at the porus by this type of adhesion. These bands of connective tissue have to be transected. The ball-tipped dissector is first used to mobilize them gently, and the Fisch scissors are then used to transect them sharply. A great deal of skill is required to avoid injury to the vessel, since the pulsating cerebrospinal fluid may shake the target. The nerve and vessel should not be pulled apart with perpendicular movements, and instead one should always try to apply shearing forces parallel to the nerve, so as to avoid applying sudden pressure to it. Thorough separation of all vessels impinging on the nerve is very important; sometimes there are two or three vessels, and it is never clear which of them is the harmful one. In particular, any cross-overs near the brain stem have to be released, as they may be more deleterious than the lateral conflicts.
After this complete decompression, small cushions have to be interposed between the nerve and the offending vessel (Fig. 14.6). I prefer to use a silicone sponge wrapped in a very thin layer of temporalis fascia. Muscle or connective tissue alone will shrink after a few months, and the resulting fibrosis will compress the nerve again. Silicone or Teflon disks alone cannot be positioned with sufficient stability, but may slip away. A small roll of thin fascia around a cushion of Silicone or Teflon sponge, however, gives good fixation and provides adequate insulation against the pulsating arterial pressure.
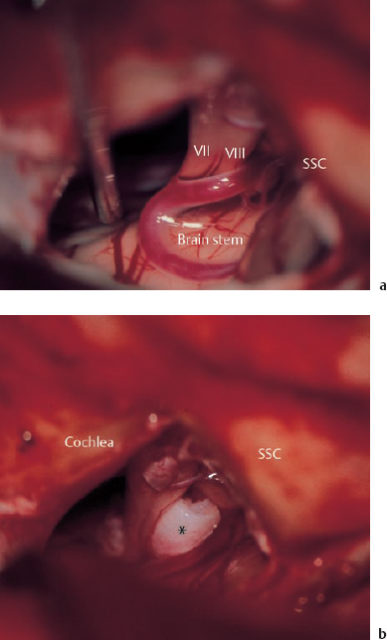
Fig. 14.6 Neurovascular decompression for hemifacial spasm via the enlarged middle fossa approach (right ear). a The facial and vestibulocochlear nerve bundle is encircled by a thick artery (at the rear), and there is an arterial loop in the foreground sending a thinner branch around the anterior face of the facial nerve. b Separation of the arterial loop from the nerve bundle using an interposed Teflon sponge (*). The patient was a 64-year-old woman who was free of symptoms for six years postoperatively, but then required occasional botulinum injections due to mild recurrences of spasm.
SSC Superior semicircular canal
Neurovascular Decompression for Progressive Vestibulocochlear Insufficiency
It is reasonable to assume that biomechanical forces exerted by arteries lying on the vestibulocochlear nerve can irritate the nerve in the same way as they provoke trigeminal neuralgia and hemifacial spasm. In patients with progressive hearing loss, tinnitus, and giddiness of unknown origin, we therefore carry out air cisternography (CT of the internal auditory canal and cerebellopontine angle with air-bubble injection), and more recently magnetic resonance angiography, to detect arterial loops crossing the vestibulocochlear nerve (Fig. 14.7). If there are positive signs of abnormal crossing of an artery or thick vein, and if the patient insists on definitive treatment of the symptoms—usually severe tinnitus or disabling vertigo, but also progressive deafness—we explore the vestibulocochlear nerve and carry out a decompression operation. This type of cryptogenic progressive deafness often used to be attributed to genetic disorders or local circulatory insufficiency. In similar cases, Fisch (1970) tried to improve the vascular supply to the eighth nerve by implanting well-vascularized muscle flaps into the internal auditory canal, an operation he termed “neuromyosynangiosis.” However, a significant correlation with sensorineural symptoms has not yet been confirmed (De Carpentier et al. 1996). Arterial loops are also found without symptoms. Our own series is still too small for any statistical analysis of the results to be meaningful. Despite some very positive findings with vascular decompression surgery (Møller et al. 1993), firm recommendations cannot yet be given. It is clear that marked improvement in hearing cannot be expected, but progressive hearing loss can be stopped, and severe tinnitus can often be relieved.
The surgical technique is analogous to that for decompression of the facial nerve. The enlarged middle fossa approach allows optimal microscopic checking of the full length of the vestibulocochlear nerve bundle between the meatal fundus and the nerve entry zone at the pons (Fig. 14.8). Dissection of the vestibular nerves is comparatively easy, but exposure of the cochlear nerve is obstructed by the overlying facial nerve. Extremely gentle separation and forward mobilization of the latter, however, allows inspection and isolation of the cochlear nerve within the internal auditory canal and at the porus (Fig. 14.9). At the brain stem, the cochlear and vestibular nerves cling tightly together and have to be handled as a single structure. If there is a history of severe permanent unsteadiness and vertigo, and if patient has given informed consent, it may be prudent to combine decompression of the cochlear nerve with vestibular nerve neurectomy (see the section on Menière’s disease, below).
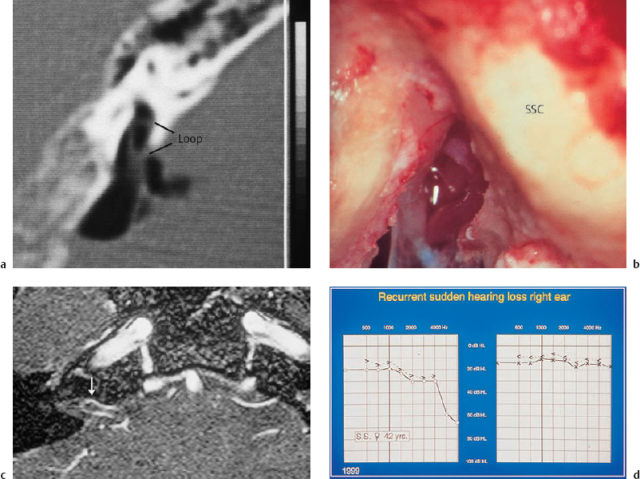
Fig. 14.7 An arterial vessel loop within the internal auditory canal, compromising the eighth cranial nerve in patients with progressive sensorineural hearing loss with severe tinnitus. a Imaging of the vessel loop on air cisternography. b The findings in the same patient (a 45-year-old man) during the decompression operation via an enlarged middle fossa approach. c Imaging of a vessel loop (arrow) on magnetic resonance angiography. d The audiogram in the same patient, who was suffering from recurrent acute hearing losses and persistent tinnitus in the right ear (a 42-year-old woman).
SSC Superior semicircular canal
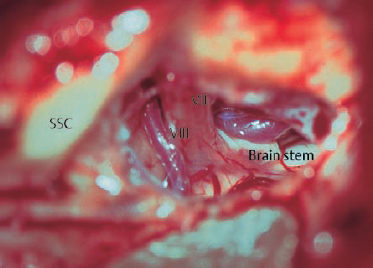
Fig. 14.8 Clear exposure of the full length of the facial and vestibulocochlear nerves from above between the brain stem and the fundus of the internal auditory canal (left ear) in an enlarged middle fossa approach.
VII Facial nerve
VIII Vestibulocochlear nerve
SSC Superior semicircular canal
Nerve Transposition
In some pathological situations, removing a nerve from its natural course and subsequently embedding it in an altered position (rerouting it) is a useful option. For example, the facial nerve can be shortened by correcting its curved parts at the geniculate ganglion or below the lateral semicircular canal, and after a traumatic rupture in this area this can make simple nerve suturing possible, avoiding the risks of interposing a nerve graft. A second, more frequent indication is anterior transposition of the facial nerve from its vertical portion, to facilitate broad exposure of the jugular foramen, or displacement of the chorda tympani in middle ear surgery Hypoglossal–facial nerve anastomosis is another example. These three goals—shortening the nerve’s course for nerve repair, achieving better visualization, and avoiding heterotopic implantation—justify artificial alteration of the normal anatomy. To some extent, this type of manipulation always implies depriving the mobilized nerve of its normal vascular supply, with the associated risk to nerve function. Obviously, transpositions over a longer distance and close to the entrance zone of important blood vessels involve greater risks than shortdistance erouting. In the facial nerve, critical portions include the internal genu at the geniculate ganglion, and the nerve’s exit from the stylomastoid foramen. By contrast, total skeletonization of the branching nerve tree within the parotid gland is usually well tolerated.
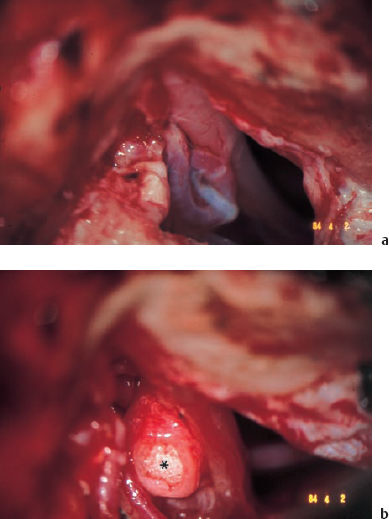
Fig. 14.9 Neurovascular decompression of the vestibulocochlear nerve for progressive sensorineural hearing loss with tinnitus and vertigo. a The arterial contact with the eighth nerve, exposed from above via the enlarged middle fossa approach. b Interposition of a Teflon sponge (*), covered with temporalis fascia and fixed in position with fibrin tissue adhesive.
Surgical Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


