Otitis Media in the Age of Antimicrobial Resistance
Margaretha L. Casselbrant
Ellen M. Mandel
Otitis media (OM), inflammation of the middle ear, is, next to the common cold, the most common diagnosis made in children. Prior to the antibiotic era, it was a very serious disease with high morbidity and mortality due to intratemporal and intracranial complications. With the introduction of antibiotics, the frequency of sequelae and complications were reduced. However, overuse of antibiotics in the treatment of acute otitis media (AOM) and otitis media with effusion (OME) has led to the development of resistant bacteria. Therefore, judicious use of antibiotics is recommended, and today, watchful waiting without antibiotics may be considered as an option in mild disease, especially in older children.
DIAGNOSIS
Definition/Symptoms and Signs
Although considered to be a continuum, OM can be subclassified into AOM and OME based on signs and symptoms. As the treatment of AOM and OME differs, it is important to accurately diagnose the two conditions. AOM is generally characterized by rapid onset of signs and symptoms of inflammation in the middle ear accompanied by middleear effusion (MEE). Signs of inflammation include bulging or fullness of the tympanic membrane (TM), erythema of the TM, and acute perforation of the TM with otorrhea. Symptoms include otalgia, irritability, and fever. OME, on the other hand, is defined as MEE without signs and symptoms of acute inflammation as found in AOM (Fig. 99.1).
Pneumatic Otoscopy
Pneumatic otoscopy is the primary diagnostic tool to evaluate the status of the middle ear as it allows for assessment of the TM and its mobility. The normal TM is translucent, concave, and moves briskly with application of positive and negative pressure. A visible landmark is the handle (manubrium) of the malleus, which is attached to the TM, with the umbo in the center of the TM. To adequately visualize the TM, the external ear canal must be cleared of cerumen and debris. The assessment of the TM should include position, color, degree of translucency, and mobility. To ascertain the mobility of the TM, a good airtight seal must be obtained between the speculum and the ear canal. The largest speculum that fits comfortably should be used. A bulb through which air is puffed should be attached to the otoscope, allowing for visualization of TM mobility. Reduced or no mobility of the TM indicates loss of compliance of the TM either as a result of effusion in the middle ear or increased stiffness due to scarring or increased thickness of the TM. Total absence of mobility of the TM may also be due to an opening in the TM either as a perforation or a patent tympanostomy tube. Other features, such as fluid levels or bubbles, may be more easily discerned with movement of the TM. The position of the TM ranges from severely retracted to bulging. Mild to moderate retraction indicates negative pressure, MEE, or both, while a severely retracted TM is usually associated with effusion. Fullness and bulging of the TM is caused by increased pressure, fluid, or both, in the middle ear. Opacification of the TM may be caused by thickening or scarring or middle-ear effusion. A red but translucent TM is usually caused by crying or sneezing due to engorgement of blood vessels in the TM. On the other hand, a “red” opaque TM that is full or bulging is often a sign of AOM. A pink, gray, yellow, or blue retracted TM with reduced or no mobility is usually seen with OME. Myringitis is inflammation of the TM without fluid in the middle ear. Use of an operating microscope (otomicroscopy) may clarify features seen on otoscopy, and visualization of scarring and atrophy of the TM may be enhanced. Use of a Siegel otoscope with the otomicroscope to provide the pneumatic component is advised.
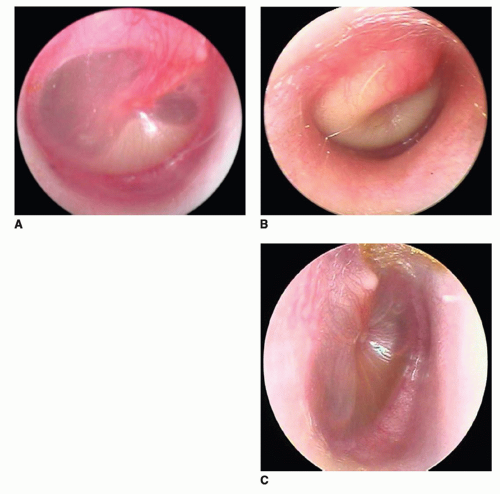 Figure 99.1 Videoendoscopy of the various middle ear states. A: Acute otitis media with fluid level; (B) acute otitis media, bulging TM; (C) Otitis media with effusion, with fluid level. Courtesy of Alejandro Hoberman, MD, Children’s Hospital of Pittsburgh of UPMC. |
Immittance Testing (Tympanometry)
Immittance testing (tympanometry) is an excellent adjunct to the assessment of middle-ear status and the management of OM. When otoscopic evaluation is uncertain or difficult to perform, tympanometry can be very useful in evaluating ear disease in children. It is easy to perform and most often well accepted by the patient. It has been used for school screening as well as in pediatricians’ offices. It is also valuable for documentation of middle-ear status over time with repeat testing. The most commonly used frequency for tympanometric testing is 226 Hz; however, for children less than 6 months of age, a frequency of 1,000 Hz is recommended. A small probe that emits a tone is placed in the ear canal with an airtight seal. The tympanogram is obtained by plotting the immittance (acoustic energy of the reflected tone) of the middle ear as a function of the pressure in the external ear canal, which is varied from −400 to +200 daPa. The instrument provides measures such as peak compensated (static) admittance, tympanometric peak pressure, acoustic reflex, and tympanometric width (TW), a measure of gradient. Algorithms have been developed to determine the presence or absence of MEE, some combining pneumatic otoscopy and tympanometry. The following set of criteria using TW to categorize middle-ear status is used: TW < 150 daPa = no OME, TW > 350 daPa = OME, and TW between 150 and 350 daPa = presence or absence of OME is determined by otoscopy (1). A flat or rounded pattern (TW > 350 daPa) with a small ear canal volume indicates MEE, while a flat pattern with a large ear canal volume suggests a perforation or a patent tympanostomy tube. In a normal air-filled middle ear with equal pressure on both sides of the TM, the peak pressure of the tympanogram is 0 daPa. Other methods of ascertaining middle-ear status have been investigated including spectral gradient acoustic reflectometry (2,3) and ultrasound (4), but they have been found to have limitations, although they may be useful for screening.
Audiometry
MEE usually results in a mild to moderate conductive hearing loss. The assessment of hearing is essential to management, as hearing impairment can predispose to delay in speech and language development and may later affect school performance. Audiometry should be used to help
determine management of the child, with more aggressive management considered if there is significant hearing impairment.
determine management of the child, with more aggressive management considered if there is significant hearing impairment.
Behavioral audiometry requires cooperation of the child with the examination, and the test is adapted to the age of the child. Visual reinforcement audiometry is used for children 6 months to 2 years of age and involves presentation of a sound stimulus in the sound field with observation of the child’s conditioned head turn response. This is rewarded with a visual reinforcement such as an animated toy. Play audiometry, for children older than 2 years, is similar to conventional audiometry (for children over 5 years of age), but the child places toys in a bucket rather than raising a hand to acknowledge they heard the sound. Conventional hearing thresholds in the sound field or ear-specific are determined at 0.25, 0.5, 1, 2, 4, and 8 kHz, depending on the age of the child. High frequency testing, from 12 to 20 kHz, can also be obtained in children (see Chapter 100).
Auditory brainstem audiometry (ABR) and transitory otoacoustic emission (TOAE) are excellent methods for testing children who do not cooperate with behavioral hearing evaluation because of very young age or developmental delay. Except for infants, sedation or general anesthesia is usually necessary for ABR testing in younger children. Three electrodes are placed (forehead and each mastoid process) to record the response to clicks of 2,000 to 4,000 Hz or pure-tone burst. The ABR consists of five to seven vertex positive waves. Waves I to III presumably reflect activity of the auditory centers in the eighth nerve fibers and pons; waves IV and V presumably reflect activity of the auditory centers in mid- to rostral pons and caudal midbrain, respectively; and activity from waves VI and VII is less certain. The ABR reflects auditory neural electrical responses that are adequately correlated to behavioral hearing thresholds. However, a normal response on the ABR suggests only that the auditory system up to the mid-brain level is responsive to the stimulus employed. Thus, it does not guarantee normal hearing.
Transitory otoacoustic emissions measure cochlear function (outer hair cells) and is an objective test of auditory function. It is commonly used for newborn hearing screening as it is fast and easy to perform. It is excellent for testing children who do not cooperate with behavioral testing. MEE may confound the results. Therefore, if the OAEs are absent, immittance testing should be performed to assess the middle ear. For children who fail TOAE testing, follow-up audiologic testing must be done to assess type and degree of hearing loss.
EPIDEMIOLOGY
Incidence and Prevalence
OM is considered a worldwide pediatric health care problem. The Early Childhood Longitudinal Study-Birth Cohort (ECLS-B), a nationally representative longitudinal study of more than 8,000 children born in 2001, showed that OM was diagnosed in 39% of children by 9 months and 62% of children by 2 years of age (5). Although the highest incidence of OM is in young children, it occurs in older children, adolescents, and adults. The Oslo Birth Cohort, enrolling infants born in 1992 to 1993, found that among 10-year-olds 13% had at least one episode of OM in the previous 12 months (6). Approximately 3% to 15% of patients with OM referred to otolaryngology clinics are adults (7). While recent studies from the United States (8), Norway (9), the Netherlands (10), and the United Kingdom (11) have indicated that there is a general decline in OM incidence, studies from developing countries and indigenous populations continue to demonstrate a heavy burden of OM (12,13).
Acute Otitis Media
Most children experience at least one episode of AOM during their childhood. The cumulative incidence of the first episode of AOM based on studies from various countries ranges from 19% to 62% by age 1 year and 50% to 84% by 3 years of age (Fig. 99.2) (14,15,16,17,18,19,20). In the majority of these studies, the peak incidence of AOM occurred during 6 to 12 months of life (20). The incidence decreases with age, and by 7 years of age, few children experience episodes of AOM. Recurrent episodes of AOM are common in young children. By 6 months of age, 20% have had two or more episodes (21). Three or more episodes of AOM by ages 1, 3, 5, and 7 years have been documented in 10% to 19%, 50%, 65%, and 75% of children, respectively (20). Six or more episodes of AOM were documented in 39% of children by age of 7 years. It should be noted that these data were obtained prior to the use of pneumococcal vaccine in infants and young children.
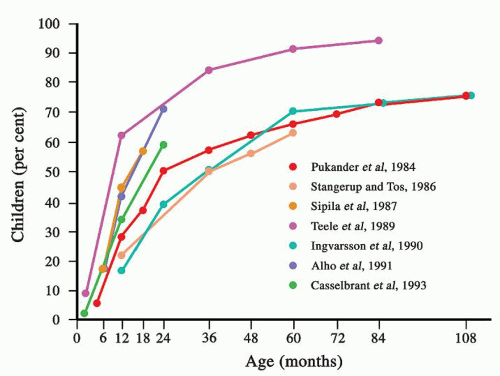 Figure 99.2 Cumulative incidence of first episode of AOM. (Reproduced from Casselbrant ML, Mandel EM. Epidemiology. In: Rosenfeld RM, Bluestone CD, eds. Evidence-based otitis media, 2nd ed. Hamilton, ON: BC Decker, 2003:147.) |
Otitis Media with Effusion
It may be difficult to determine the “true” incidence of OME as by definition OME is asymptomatic. Therefore, a short time between observations is needed to precisely assess the onset and time to resolution of each new episode of OME as approximately 65% of OME episodes in children 2 to 7 years resolve within 1 month (22). Monthly examinations with otoscopy and tympanometry in 2- to 6-year-old children in a day care center in Pittsburgh revealed MEE at least once in 53% to 61% of the children and a Danish study found an incidence of MEE of 26% in 7-year-old children followed monthly for 1 year using tympanometry (23).
The point prevalence of MEE from different countries shows a wide variation depending on the age of the child, season of the year, as well as type of assessment. Thus, it must be emphasized that when comparing the outcome between studies, there is a need to evaluate study methodology and exercise caution when drawing conclusions. However, nearly all children experience at least one episode by 3 years of age (24).
Risk Factors
Risk factors can be host related (age, gender, race, prematurity, allergy, immunocompetence, cleft palate and craniofacial abnormalities, genetic predisposition) as well as environmental (upper respiratory infections [URIs], seasonality, day care, siblings, tobacco smoke exposure, breast-feeding, socioeconomic status, pacifier use, and obesity) and are considered important in the occurrence, recurrence, and persistence of middle-ear disease.
Host-Related Factors
Age
The highest incidence of AOM occurs between 6 and 11 months of age (20), and onset of the first episode of AOM before 6 months (20) or 12 months of age is a powerful predictor of recurrence (25). The risk of persistent MEE after an episode of AOM is inversely correlated with age (20), and children who experience their first episode of MEE before 2 months of age are at a higher risk for persistent fluid during their first year of life than are children having their first episode later (26).
Sex
Most investigators have reported no apparent sex-based difference in the incidence of OME. Some studies have found a significantly higher incidence of AOM in males as well as more recurrent episodes than in females, but others have not found this (24).
Race
Previous studies have suggested a lower incidence of OM in black children compared to white children. However, more recent studies in which the children were followed prospectively with examinations of the ears every 6 weeks showed no difference between the black and white children in their experience with OM (27,28). One study, part of an American population-based sample survey evaluating school children ages 6 to 10 years with tympanometry, also reported no difference between black and white children. However, the prevalence of OME was significantly higher in Hispanic children compared to white children (29).
Allergy/Immunocompetence
Controversy remains regarding the role of allergy in the pathogenesis of OM as allergy is a common problem in children, occurring at a time when respiratory infections and OM are common. Most, but not all, of the epidemiologic studies have supported an association. Pukander and Karma (30) found, in 707 children with AOM, that in children with atopic manifestations, the persistence of MEE for 2 months or longer was greater than in children without allergy. However, in another study, atopic diathesis was not found to predispose a child to the development of AOM (31). Tomonaga et al. (32) determined that allergic rhinitis was present in 50% of 259 patients (mean age of 6 years) in whom OME had been diagnosed while OME was present in 21% of 605 patients (mean age of 9 years) in whom allergic rhinitis had been diagnosed. Among 108 children (ages 5 to 8 years, mean age of 6 years) in whom neither condition had been diagnosed, the incidences of allergic rhinitis, OME, and both of these conditions were 17%, 6%, and 2%, respectively. Another investigative group (33) compared 76 children with MEE admitted for bilateral myringotomy with tube insertion (M&T) to 76 controls matched by age, gender, and season of admission for a general surgical procedure. Results showed a nearly fourfold increase in the risk of persistent MEE in children who had atopic symptoms for more than 15 days per month. In another study, Bernstein and Reisman (34) determined the allergy status of a group of 200 children who had undergone one or more M&T procedures. They diagnosed allergy in 23% of the entire group but found that the frequency was 35% among the 88 children with multiple myringotomies with tube insertions. The frequency of allergy in these patients was higher than that reported for children of similar age in the general population. The above studies generally found a higher frequency of OME in allergic children compared with age-matched nonallergic children, as well as higher frequencies of allergy in children with OME compared with children without OME. Skoner et al. (35) suggested that if significant allergic rhinitis is diagnosed in a patient with OME, it should be treated aggressively. More studies are needed to evaluate the relationship between these two conditions.
Children with recurrent OM as well as other recurrent infections may have a defect in the immune system such as a defect in phagocyte function, humoral immunity, local
immunity, or other immune defects (36). Immunologic screening is indicated to exclude an immunodeficiency in children with frequent episodes of OM or an abnormal course of disease (37). While agammaglobulinemia and hypogammaglobulinemia are rare, deficient or lowered immunoglobulin (Ig)A or decreased levels of one or more IgG subclasses, in particular IgG2, are more common. The specific antibody response to bacterial capsular polysaccharides is often low. Kaur et al. (38) reported finding that, after an episode of AOM due to Streptococcus pneumoniae, otitis-prone children and children who failed treatment for AOM had less of an IgG serum antibody response compared to non-otitis-prone children to proteins of S. pneumoniae. Children infected with the human immunodeficiency virus have a significantly higher recurrence rate than normal children or children who have seroconverted (39).
immunity, or other immune defects (36). Immunologic screening is indicated to exclude an immunodeficiency in children with frequent episodes of OM or an abnormal course of disease (37). While agammaglobulinemia and hypogammaglobulinemia are rare, deficient or lowered immunoglobulin (Ig)A or decreased levels of one or more IgG subclasses, in particular IgG2, are more common. The specific antibody response to bacterial capsular polysaccharides is often low. Kaur et al. (38) reported finding that, after an episode of AOM due to Streptococcus pneumoniae, otitis-prone children and children who failed treatment for AOM had less of an IgG serum antibody response compared to non-otitis-prone children to proteins of S. pneumoniae. Children infected with the human immunodeficiency virus have a significantly higher recurrence rate than normal children or children who have seroconverted (39).
Cleft Palate/Craniofacial Abnormality
To date, no evidence suggests an effect of cleft palate/cleft lip type or laterality on OME prevalence (40), and an equally high OME prevalence was reported in patients with diagnosed submucosal cleft palate (41) but not in patients with bifid uvula (42,43). OM is considered “universal” in infants less than 2 years of age with unrepaired cleft palate (44). After surgical repair of the palate, the occurrence of OM is reduced, which is most likely due to improvement of eustachian tube function. In a prospective study of 150 children with cleft lip and palate, enrolled between 2 and 18 months of age, Robinson et al. (45) reported a 92% prevalence of OME before palate repair, no short-term change after palate repair, but a reduced prevalence to 70% at 4 years of age. Many children continue to have problems up into the teens. A reduction of middle-ear disease by newer palatoplasty procedures has been suggested (46). OM is also common in children with other craniofacial abnormalities also due to anatomical or functional eustachian tube dysfunction (47). Down syndrome children have, in addition to poor active eustachian tube function, low resistance of the eustachian tube, which predisposes to reflux of nasal secretions into the middle ear (48).
Genetic Predisposition
The frequency of the occurrence of one episode of OM is so high that a genetic predisposition cannot be expected. However, a predisposition to recurrent episodes of OM and chronic MEE may have a significant genetic component. The etiology of OM is multifactorial, involving environmental as well as genetic factors. A large number of genes may be involved, each contributing to a particular increase in disease risk.
Twin and triplet studies have been used to assess the heritability of OM. Two retrospective studies using questionnaires have been published. The first study, using 2,750 Norwegian twin pairs, estimated the heritability at 0.74 in females and 0.45 in males (49). In the second study, the estimated heritability was, on average, 0.57 at ages 2, 3, and 4 years (50). In a prospective twin/triplet study from Pittsburgh with monthly assessments of middle-ear status, the heritability estimate for OM at age 2 years was 0.79 in females and 0.64 in males (51). Heritability is a population statistic to ascertain if a trait is heritable, while link-age and association studies may identify genetic regions or specific genes influencing the particular trait or disease. Daly et al. (52), using genome-wide linkage analysis, have suggested that regions of chromosomes 19q and 10q contain genes contributing to the susceptibility to chronic OME/recurrent AOM. Subsequent fine mapping of both regions further strengthened the evidence for this link-age (53). A second genome-wide linkage analysis demonstrated linkage regions with plausible candidate genes in 17q12 (AP2B1, CCL5, and a cluster of other CCL genes) and in 10q22.3 (SFTPA2) (54). Polymorphisms in mannose binding proteins (55), surfactant protein (56), mucin expression (57), and cytokines (58,59) have been associated with mucosal immunity and development of disease. In addition, polymorphisms in three genes (FBXIIO, TLR4, and PAII) originally identified in mouse models of OM have shown evidence of susceptibility to childhood OM in cohort studies (60,61,62).
Environmental Factors
The main risk factors for OM are day care, number of siblings, tobacco smoke exposure, breast-feeding, birth weight, socioeconomic status, and air pollution. Environmental risk factors for OM across Western countries, including European countries, the United States, Canada, and Australia, have shown large variations in rates across the various countries: day care at ages 1 to 3 years (Sweden 75% vs. Italy 6%), breast-fed at 6 months (Norway 80% vs. Poland 6%), and women smoking (Germany, France, and Norway 30% to 40% vs. Portugal less than 10%) (63).
Upper Respiratory Infection/Seasonality
Both epidemiologic evidence and clinical experience strongly suggest that OM is frequently a complication of an URI. The incidence of AOM is highest during the fall and winter months and lowest during spring and summer months, which parallels the incidence of URI (22). This supports the hypothesis that an episode of URI plays an important role in the etiology of OM. Rhinovirus, RSV, adenovirus, and coronavirus have been detected in MEE during episodes of AOM (64,65). Winther et al. (66) reported that the OM complication rate of a cold-like illness was 33%. The predominant virus in this population was the rhinovirus.
Day Care/Home Care/Siblings
Almost universally, day care center attendance remains a very important risk factor for development of OM. For example, prevalence of high negative middle-ear pressure
and flat tympanograms (type B), indicative of MEE, have been shown to be highest in children cared for in day care centers with many children, intermediate in children in family day care with fewer children, and lowest in children cared for at home (67). Data from the United States ECLS-B, including more than 8,000 children studied at 9 months and 2 years of age, showed a significant increased risk for recurrent AOM and tube insertion for children attending day care (5).
and flat tympanograms (type B), indicative of MEE, have been shown to be highest in children cared for in day care centers with many children, intermediate in children in family day care with fewer children, and lowest in children cared for at home (67). Data from the United States ECLS-B, including more than 8,000 children studied at 9 months and 2 years of age, showed a significant increased risk for recurrent AOM and tube insertion for children attending day care (5).
Birth order has been shown to be associated with episodes of OM and percentage of time with MEE (22). Firstborn children had a lower rate of episodes of AOM and less time with MEE during the first two years of life than children with older siblings. Also, having more than one sibling was significantly related to early onset of OM (30), and the presence of more children in the household was related to more time with MEE (28).
The reason for the higher morbidity in children in day care centers and in children with older siblings may be related to the greater opportunity for exposure to viral URI, which may cause eustachian tube dysfunction leading to the development of OM.
Tobacco Smoke Exposure
An association between OM and passive exposure to smoking has been reported by many investigators, while others have not been able to demonstrate such an association. In most studies, the information regarding smoke exposure has been obtained from the parents. A few studies have measured cotinine, a metabolite of nicotine, in blood, urine, or saliva of the child and have been able to more accurately determine the association between OM and smoke exposure (21,68). More information about the pathogenesis, duration, and intensity of exposure is needed to clarify this association. Two studies have shown an association between middle-ear status and parental smoking. In children exposed to parental smoking, tympanostomy tubes stayed in place for 59 weeks compared to 86 weeks in children who were not exposed to smoking (69). Also, myringosclerosis was more prevalent in children with two smoking parents compared to those with no smoking parents (64% vs. 20%), and maternal smoking was associated with a highly increased risk of recurrent OM after insertion of tympanostomy tubes (70).
Breast-/Bottle Feeding
Breast-feeding for 6 months exclusively is recommended by most national and international authorities, including the American Academy of Pediatrics and the American Academy of Family Physicians, the World Health Organization (WHO), and the United Nations Children’s Fund. In 2002, Kramer and Kakuma (71) published a comprehensive review of the world literature to determine health benefits of exclusive breast-feeding for 6 months compared to 3 to 4 months. They reported a decrease in the risk for gastrointestinal infection even in developed areas. It had not been shown previously that exclusive breast-feeding for 6 months or longer compared to 4 to less than 6 months in the United States provided greater protections against respiratory infections. Therefore, a secondary analysis of data from the National Health and Nutrition Examination Survey III, a population-based cross-sectional home survey conducted from 1988 to 1994, was undertaken (72). After adjusting for demographic variables, child care and smoke exposure, the data revealed statistically significant increased risk for both pneumonia (OR: 4.27; 95% CI: 1.27 to 14.35) and three or more episodes of OM (OR: 1.95; 95% CI: 1.06 to 3.59) in those children breast-fed 4 to less than 6 months. These findings further support the current recommendations that infants receive breast milk exclusively during the first 6 months of life.
Socioeconomic Status
Socioeconomic status and access to health care are factors that may affect the incidence of OM. It has been generally thought that OM is more common among the lower socioeconomic strata due to poor sanitary conditions and crowding. Paradise et al. (28) followed 2,253 infants for 2 years in the United States and found an inverse relationship between the cumulative proportion of days with MEE and socioeconomic status. However, many studies have not revealed any correlation between socioeconomic status of the child’s family and the incidence of MEE.
Pacifier Use
Niemelä et al. (73) reported that pacifier use increased the annual incidence of AOM and calculated that pacifier use was responsible for 25% of AOM episodes in children younger than 3 years. They reported the results of an intervention trial in which parents in various well-baby clinics were taught that pacifier use was harmful and should be limited, while parents in other clinics were not provided with this information. This led to a 29% decrease in AOM in the group provided with pacifier information. Pacifier use has been theorized to contribute to the development of OM, possibly due to the sucking action of the child propelling nasopharyngeal secretions into the middle ear or by the pacifier acting as a fomite. However, Brook and Gober (74) cultured the surface of pacifiers from children with AOM but found no pathogens typical of AOM. The role of pacifier use in AOM remains unclear.
Obesity
Recent studies have indicated that there may be an association between OM and body mass index (BMI). Tympanostomy tube insertion and overweight were studied in a predominantly white cohort of children (97%) followed from birth to 2 years of age (75). Weight for length and BMI
for age were calculated using well-child visit data. A history of tympanostomy tube insertion significantly predicted risk of BMI index at both greater than 95th percentile and greater than 85th percentile at 2 years of age after controlling for risk factors and confounders. However, early weight status was not related to later OM, recurrent OM, or tympanostomy tube insertion. In another cohort of American Indian children, a history of recurrent AOM increased the likelihood of weight-for-length index greater than 95th percentile (76). The mechanisms are not clear, but it was suggested that inflammatory changes in the middle ear can result in objective gustatory changes.
for age were calculated using well-child visit data. A history of tympanostomy tube insertion significantly predicted risk of BMI index at both greater than 95th percentile and greater than 85th percentile at 2 years of age after controlling for risk factors and confounders. However, early weight status was not related to later OM, recurrent OM, or tympanostomy tube insertion. In another cohort of American Indian children, a history of recurrent AOM increased the likelihood of weight-for-length index greater than 95th percentile (76). The mechanisms are not clear, but it was suggested that inflammatory changes in the middle ear can result in objective gustatory changes.
PATHOPHYSIOLOGY AND PATHOGENESIS
The pathophysiology of OM is multifactorial with various overlapping factors (Fig. 99.3).
Eustachian Tube Function
The eustachian tube in the infant is shorter, wider, and more horizontal than in the adult, which leads to the high rate of OM in infants and children. By 7 years of age, when the tube has a more adult configuration, the prevalence of OM is low (77). The three physiologic functions of the eustachian tube are (a) pressure regulation (ventilation), (b) protection, and (c) clearance (drainage). Of these three functions, pressure regulation is the most important (36) (Fig. 99.4). Middle-ear pressure is equilibrated to atmospheric pressure through active intermittent openings of the eustachian tube caused by contraction of the tensor veli palatini muscle during swallowing, jaw movements, or yawning. If active function is impaired, negative pressure will develop in the middle ear. Pressure regulation can be impaired by failure of the opening mechanism (functional obstruction) or anatomical (mechanical) obstruction. In ears with normal eustachian tube function, the eustachian tube is collapsed when at rest. This protects the middle ear from nasopharyngeal sound pressure and reflux of secretions from the nasopharynx. The clearance of secretions produced within the middle ear into the nasopharynx is provided via the mucociliary system and through the “pumping action” of the eustachian tube during closing. The passive closing of the tube is initiated at the middle-ear end of the eustachian tube and progresses toward the nasopharyngeal end, which results in removal of the secretion.
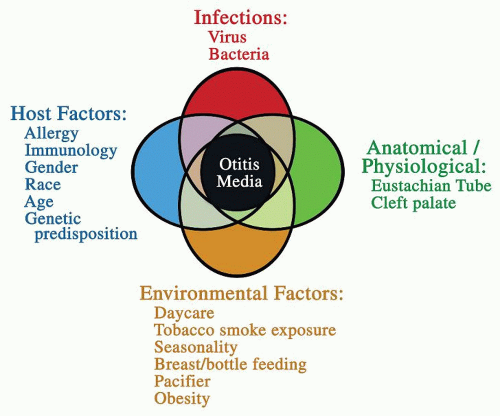 Figure 99.3 Various factors interact in the pathogenesis of OM. (Adapted from Casselbrant ML, Mandel EM. Acute otitis media and otitis media with effusion. In: Flint W, et al, eds. Cummings otolaryngology—head and neck surgery, 5th ed. Philadelphia, PA: Mosby Elsevier, 2010.) |
Using a pressure chamber, Bylander et al. (78) evaluated eustachian tube function in children and adults who were considered otologically normal with intact TMs. While only 5% of the adults were not able to equilibrate negative middle-ear pressure, as many as 35.8% of the children
could not equilibrate negative pressure. Children ages 3 to 6 years performed worse than children ages 7 to 12 years. These studies indicate that in even apparently otologically normal children, eustachian tube function is worse than in adults, but it does improve with age. The improvement in the eustachian tube function parallels the decrease in the incidence of OM. Stenström et al. (79) tested eustachian tube function in 50 otitis-prone children and 49 children with no history of AOM (controls) using a pressure chamber. The otitis-prone children had significantly poorer active tubal function than the normal controls, suggesting that recurrent AOM is the result of functional obstruction of the eustachian tube.
could not equilibrate negative pressure. Children ages 3 to 6 years performed worse than children ages 7 to 12 years. These studies indicate that in even apparently otologically normal children, eustachian tube function is worse than in adults, but it does improve with age. The improvement in the eustachian tube function parallels the decrease in the incidence of OM. Stenström et al. (79) tested eustachian tube function in 50 otitis-prone children and 49 children with no history of AOM (controls) using a pressure chamber. The otitis-prone children had significantly poorer active tubal function than the normal controls, suggesting that recurrent AOM is the result of functional obstruction of the eustachian tube.
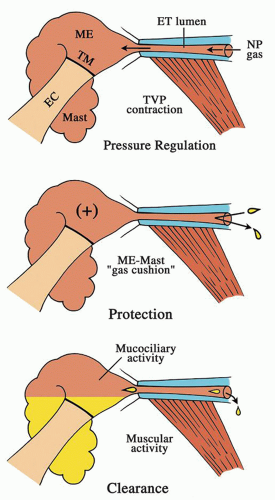 Figure 99.4 Functions of the eustachian tube (ET)-middle ear (ME)-mastoid (mast) gas cell system. Pressure regulation function is related to active dilation of the tube by contraction of the tensor veli palatini muscle (TVP) (upper figure). Protective function is dependent, in part, on an intact middle ear and mastoid gas cells to maintain a gas cushion (middle figure). Clearance function is enhanced by mucociliary activity and muscular activity during tubal closing (lower figure). EC, external canal; NP, nasopharynx; TM, tympanic membrane. In: Bluestone CD. Eustachian tube: structure, function, role in otitis media. Hamilton, ON: BC Decker, 2005:51. |
The forced response test (FRT) is designed to measure the passive and active function of the eustachian tube. In a recent pilot study, the FRT was used to test 3-year-old children 3 months after tympanostomy tube insertion with chronic OME (17 children, 24 ears) or recurrent AOM (15 children, 22 ears). The passive resistance and one measure of active function were significantly higher in the recurrent AOM group. The frequency of tubal dilation was not significantly different between the groups (80). However, based on the high variability in all the test parameters, the authors dismiss the possibility that an individual can be assigned to a particular disease expression based on the FRT test.
Infection
Bacteriology
Prior to the year 2000, studies in the United States reported that S. pneumoniae was the single most common bacterial pathogen in AOM, followed by Haemophilus influenzae and Moraxella catarrhalis, Streptococcus pyogenes, and other miscellaneous bacteria accounted for just a few cases. From ears with chronic OME, H. influenzae was the single most common pathogen, followed by S. pneumoniae, M. catarrhalis, and other bacteria accounting for a small percentage of cases each. Prevnar, a heptavalent conjugated pneumococcal vaccine (PCV7) for infants and young children, was licensed in the United States in 2000. Casey and Pichichero (81) examined the experience of children in a suburban Rochester, NY, practice in the years 2001 to 2003 (after the introduction of PCV7) compared to the years 1995 to 2000 and reported a 24% decrease in persistent AOM and AOM treatment failures. They also reported a decrease in recovery of S. pneumoniae from the ears of such children and an increase in H. influenzae. McEllistrem et al. (82) looked at middle-ear cultures obtained between 1999 and 2002 at five institutions. They reported that the percentage of AOM episodes due to non-PCV7 serogroups increased after 2000 from 12% in 1999 to 32% in 2002, and the nonvaccine serotypes were more frequent in those who received more than one dose of vaccine.
Nasopharyngeal carriage was also examined. Pelton et al. (83) enrolled 275 infants and children 2 to 24 months of age in a surveillance study in which nasopharyngeal swabs or nasal washes were obtained at all well-child visits and at visits for AOM. From 2000 to 2003, they noted a decrease in vaccine serotypes with an increase in nonvaccine serotypes. Tracking antimicrobial susceptibility, they found that the MIC50 and MIC90 for amoxicillin were stable until the last 6-month period when they both increased significantly. Jacobs et al. (84) examined the nasopharyngeal flora in children undergoing tympanostomy tube placement in March 2004 to March 2005 and also found a decrease in vaccine serotypes with a concomitant increase in nonvaccine serotypes, many of which were antibiotic-resistant strains.
Casey et al. (85) looked at the bacteriology of the nasopharynx and middle-ear fluid from children with no or infrequent episodes of AOM and from children with recurrent AOM during the years 2007 to 2009. Compared to their findings in 2001 to 2003, they found that, unlike shortly after the introduction of the conjugate pneumococcal vaccine, the frequency of non-PCV7 strains was nearly equal that of H. influenzae, with the nonvaccine serotypes, particularly 19A, replacing the vaccine serotypes. The frequencies of S. pneumoniae and H. influenzae were nearly equal, and the bacteria recovered from otitis-prone children were not different from that recovered from children with their first or second AOM episode.
Recently, a new vaccine with 13 serotypes of S. pneumoniae (PCV13) has replaced the 7-valent vaccine. In addition to the PCV7 strains, it includes serotypes 1, 3, 5, 6A, 7F, and 19A, which should add significant protection. As previously, there is a need for continued surveillance of the bacteriology of AOM with the use of this new vaccine.
Biofilms
Bacterial biofilms are sessile communities of interacting bacteria attached to a surface and encased in a protective matrix of exopolysaccharides rather than living in a motile “planktonic” or free-floating state. The matrix allows for protection from phagocytosis and other host defense mechanisms due to lack of accessibility by Igs and complement. The reduced metabolic rate of bacteria in the biofilm renders them resistant to antimicrobial treatment. The bacterial community relies on a complex intracellular communication system that provides for organized growth characteristics known as “quorum sensing.” Biofilms have been known for a long time to exist on hard surfaces such as metal pipes, or teeth. Post et al. (86), using polymerase chain reaction methodology (PCR), found evidence of bacteria in 48% of culture-negative MEEs from children undergoing tympanostomy tube insertion for chronic OME. Hall-Stoodley et al. (87) obtained confocal laser scanning microscopy images from the middle-ear mucosa of 26 children scheduled for tympanostomy
tube insertion for recurrent/persistent OM and 8 controls (3 children and 5 adults) who underwent cochlear implants. Generic stains and species-specific probes for H. influenzae, S. pneumoniae, and M. catarrhalis were used to evaluate biofilm morphology. Mucosal biofilms were visualized in 92% of the mucosa from children with chronic and recurrent OM, but were not observed in any of the eight controls. The authors suggested that the findings supported the hypothesis that chronic middle-ear disease is biofilm-related. Biofilms have also been identified in the nasopharynx of children with OM, and it was suggested that the biofilm may act as a reservoir for bacterial pathogens resistant to antibiotics. The mechanical debridement of the nasopharyngeal biofilms may explain the observed clinical benefit associated with adenoidectomy in subsets of pediatric patients (88).
tube insertion for recurrent/persistent OM and 8 controls (3 children and 5 adults) who underwent cochlear implants. Generic stains and species-specific probes for H. influenzae, S. pneumoniae, and M. catarrhalis were used to evaluate biofilm morphology. Mucosal biofilms were visualized in 92% of the mucosa from children with chronic and recurrent OM, but were not observed in any of the eight controls. The authors suggested that the findings supported the hypothesis that chronic middle-ear disease is biofilm-related. Biofilms have also been identified in the nasopharynx of children with OM, and it was suggested that the biofilm may act as a reservoir for bacterial pathogens resistant to antibiotics. The mechanical debridement of the nasopharyngeal biofilms may explain the observed clinical benefit associated with adenoidectomy in subsets of pediatric patients (88).
Nistico et al. (89), using a culture-independent molecular diagnostic methodology and confocal scanning, demonstrated that H. influenzae, S. pneumoniae, M. catarrhalis, and S. aureus were present in adenoids from children with “chronic otitis media” (rAOM and/or cOME) as well as in children with obstructive sleep apnea (OSA) in biofilm clusters on the mucosal surface and within adenoid crypts as well as intracellularly. The distribution of pathogens in the two groups was similar except that H. influenzae was significantly more common in children with chronic OM than in OSA (66.7% vs. 10%, P = 0.005).
Viruses
Until the introduction of PCR, viruses were not considered a major factor in the etiology of OM, probably due to technical difficulties in isolating the viruses. However, using the PCR technique, it has been possible to identify respiratory syncytial virus (RSV), influenza, adenovirus, parainfluenza, and rhinoviruses in MEE (65,90). There is strong evidence that viruses have a crucial role in the development of AOM (90). In the majority of children, viral infection of the upper respiratory tract mucosa initiates the whole cascade of events that finally leads to the development of AOM, and AOM may be regarded as a complication of a preceding or concomitant viral infection. In a study of 60 children (24 families) with at least 2 children between the ages of 1 and 5 years who were followed from October 2003 through April 2004 by daily parental recording of illness signs, weekly pneumatic otoscopy and viral PCR of nasal secretions collected during “colds” or when MEE was noted or from enrolled sibs without these conditions, one or more viruses were identified from 73% of secretions collected during a “cold” but from only 18% collected at a time without a “cold” (66). Of 93 episodes of OM (includes AOM and OME), 70% occurred during a “cold,” and nasal secretions from 77% of children at the time of these episodes were positive for virus. For OM episodes, both with a “cold” and without, rhinovirus was the virus found most frequently; influenza and RSV were not found in episodes not associated with a “cold.” When a virus was isolated from the nasopharynx with a cold or not, an associated episode of OM was classified as AOM in 8% of rhinovirus detections but in 33% and 38% of detections of RSV and influenza A virus, respectively (91). In a cohort of children 6 months to 3 years of age whose parents were instructed to present to the study when the child had a URI or AOM, Chonmaitree et al. (92) found AOM in 37% of URI episodes and OME in 24%. They found rhinovirus and adenovirus most commonly detected during URI, but the rate of OM associated with rhinovirus was lower than for other viruses.
Allergy and Immunology
Even though allergy is considered in the pathogenesis of OM, the causal mechanism is not understood, and well-controlled studies to prove the efficacy of antiallergic medication in the treatment of OM are lacking. Several mechanisms by which allergy may cause OM have been suggested: (a) the middle ear as a “shock organ” (target), (b) allergy-induced inflammatory swelling of the eustachian tube mucosa, (c) inflammatory obstruction of the nose, and (d) aspiration of bacteria-laden allergic nasopharyngeal secretions into the middle ear. The last three mechanisms involve an association between allergy and abnormal eustachian tube function. Prospective studies have reported a relationship between upper respiratory tract allergy and eustachian tube obstruction in a series of provocative, intranasal, allergen-inhalation challenge studies (93).
Recent studies focus on the analysis of the inflammatory markers in MEE to determine the role of allergy. Both Th (T-helper) 1 and Th2 inflammatory patterns have been found in OME. Th1 cytokines antagonize allergic inflammation and play a key part in the defense against viruses and intracellular pathogens, while Th2 cytokines promote IgE production, eosinophil growth, and mucus production (94). The chemoattractant cytokine RANTES (regulated upon activation, normal T cell expressed and secreted) and eosinophilic cationic protein (ECP), signs of a Th2 process, were assessed in MEE samples from 25 children with allergy and 20 nonallergic children, aged 5 to 11 years at the time of tympanostomy tube insertion (95). RANTES as well as ECP were significantly higher in the MEE samples from children with allergy than children without allergy (P < 0.01; P < 0.05, respectively). There was also a positive correlation between RANTES and ECP in MEE (P < 0.01) in children with allergy, which suggests that allergy is a contributing factor in the pathogenesis of OM.
Children with major immune deficiencies may have recurrent OM as part of their overall clinical picture, but most otitis-prone children may have only a subtle immunologic abnormality that predisposes them to recurrent infections (96). The three major OM pathogens—S.
pneumoniae, H. influenzae, and M. catarrhalis—frequently colonize the nasopharynx. There are many different strains of these organisms, and among the different strains, there are heterologous surface (strain-specific) antigens and conserved antigens. Conserved antigens induce broadly protective antibodies while strain-specific antigens induce limited protection. Otitis-prone children may display strain-specific immunity but fail to develop a broadly protective antibody response, which makes them susceptible to recurrent and persistent OM (97).
pneumoniae, H. influenzae, and M. catarrhalis—frequently colonize the nasopharynx. There are many different strains of these organisms, and among the different strains, there are heterologous surface (strain-specific) antigens and conserved antigens. Conserved antigens induce broadly protective antibodies while strain-specific antigens induce limited protection. Otitis-prone children may display strain-specific immunity but fail to develop a broadly protective antibody response, which makes them susceptible to recurrent and persistent OM (97).
Recurrence of bilateral OME after tympanostomy tube insertion was more likely in children with poor eustachian tube function and low IgA or low IgG2 and decreased levels of mannose-binding lectin than in children with poor tubal function and high IgA and IgG2 measured at time of tube insertion (98). This suggests that an interaction between various immune factors may increase the risk for the development of OM.
Gastroesophageal Reflux
In 2002 Tasker et al. (99) reported finding pepsin/pepsinogen, using enzyme-linked immunosorbent assays, in 90.8% of 65 MEE samples obtained at the time of myringotomy in children. The pepsin/pepsinogen levels ranged from 0.8 to 213.9 µg/mL, which is 1,000 times higher than serum levels. He et al. (100), using a sensitive and specific pepsin assay, detected pepsin activity in 14.4% of 152 subjects undergoing tympanostomy tube insertion. The levels of pepsin ranged from 13 to 687 ng/mL. O’Reilly et al. (101) found pepsin in the middle-ear cleft of 20% of children (14% of ears) undergoing tympanostomy tube insertion for OM, compared to 1.4% of control children (1.5% of ears) undergoing cochlear implant who did not have a history of OM. Children with purulent effusions were more likely to have pepsin than those with mucoid or serous effusion (47% vs. 20% vs. 27%, respectively).
A prospective, uncontrolled before-and-after intervention study was performed in children with OM and GERD (102). Thirty-seven of the forty-seven entered children were evaluated 8 to 12 weeks following antireflux therapy (lansoprazole in the morning with ranitidine or nizatidine at bedtime) and were found to have improvement in hearing, quality of life scores, reflux questionnaires, fiberoptic laryngoscopy, otoscopy, and tympanometry.
PREVENTION OF DISEASE
Management of Environmental Factors
Promotion of breast-feeding in the first 6 months of life, avoidance of supine bottle feeding and pacifier use, and elimination of passive tobacco smoke may be helpful in reducing the risk of development of OM. Alteration of child care arrangements such that the child is exposed to fewer children may also be of benefit.
Vaccines
The three most common bacteria isolated from the middle ear are S. pneumoniae, H. influenzae, and M. catarrhalis. Presently, the S. pneumoniae vaccines (Pneumovax, Prevnar, and Prevnar 13) are the only bacterial vaccines available in the United States for OM. Although respiratory viruses, such as RSV, influenza, adenovirus, parainfluenza, and rhinovirus, have been isolated in MEE using PCR, influenza vaccine is the only available recommended viral vaccine today that may impact OM.
Bacterial Vaccines
Streptococcus pneumoniae
Pneumovax is a 23-valent polysaccharide vaccine [PPSV23], which is not efficacious in children 2 years or younger due to poor antibody production. Prevnar is a conjugated vaccine in which pneumococcal polysaccharides are conjugated to a nontoxic mutant of diphtheria toxin. The 7-valent vaccine (PCV7, serotypes 4, 6B, 9V, 14, 18C, 19F, 23F) was licensed for use in the United States in 2000 and recommended for use in children less than 6 years of age by the American Academy of Pediatrics (103). Prevnar 13 (PCV13) replaces PCV7. It was licensed for use in 2010 and includes six additional serotypes (1, 3, 5, 6A, 7F, and 19A) that can cause invasive pneumococcal disease, including the increasingly drug-resistant serotype 19A. The PCV 13 vaccine is recommended for all children 2 to 59 months of age and for children 60 to 71 months of age with an underlying condition that makes them more susceptible to pneumococcal disease. Children up to age 59 months who are fully (four doses) vaccinated with PCV7 should receive one dose of PCV13. (For further guidance by the American Academy of Pediatrics on use of PCV13 and PPSV23, see the Policy Statement, www.pediatrics.org/cgi/doi/10.1542/peds.2010-1280.)
There was great hope that the introduction and subsequent use of PCV7 for infants and young children would lead to a substantial decrease in AOM. Data from vaccine trials conducted in California (104) and Finland (105) revealed only a 7% and a 6% relative reduction, respectively, in AOM episodes. However, in the California study, children with recurrent OM benefited from the vaccine with a reduction of OM episodes varying from 9.3% to 22.8%, increasing as the frequency of episodes of AOM increased. In addition, immunized children were 20.1% less likely to require tube placement than controls. The PCV7 vaccine demonstrated a much higher efficacy (greater than 80%) in reducing invasive pneumococcal disease than reducing the burden of OM. Additional follow-up of the study subjects continued to demonstrate a modest amount of protection against episodes of AOM and tympanostomy tube insertion (106). Reduction in need for tympanostomy tubes after introduction of PCV7 was also shown in Tennessee and New York (107) and in Finland (108).
With use of the vaccine, pneumococcal colonization in the nasopharynx has changed as the vaccine has caused a reduction in the carriage rate of vaccine serotypes and replacement with nonvaccine serotypes (84,109). It should be noted that a reduction in nasopharyngeal carriage of vaccine serotypes and an increase in nonvaccine serotypes have also been seen in children younger than 7 months of age (83).
In the United States and Finland, the initial immunization with PCV7 is at age 2 months based on the results from the clinical trials. However, the question of whether or not the results obtained in the Finnish and US trials could be extrapolated to older children who already had a history of recurrent episodes of AOM was addressed by Dutch and Belgian trials (110,111). Seventy-eight and three hundred and eighty-three children with documented histories of recurrent AOM were enrolled in the Belgian and Dutch studies, respectively. In both trials, children between 1 and 7 years were immunized at entry with PCV7 followed by a booster immunization with a 23-valent pneumococcal polysaccharide vaccine 7 months later and followed up for a total of 18 months in the Dutch and 26 months in the Belgian trial. The results from these two studies did not lend any support to the use of pneumococcal conjugate vaccine to prevent AOM in previously unvaccinated toddlers and children with a history of recurrent AOM. In the infant studies, the PCV7 immunization may prevent or delay nasopharyngeal colonization of the most frequent pneumococcal serotypes and consequently delay pneumococcal episodes of AOM until a later age. In older children, who already are carriers of pneumococci, there is rapid replacement of pneumococcal vaccine serotypes with nonvaccine serotypes.
An 11-valent polysaccharide pneumococcal serotype vaccine conjugated to H. influenzae-derived protein D was evaluated in a clinical trial conducted in the Czech Republic enrolling a total of 4,968 children who were followed to the end of the second year of life with middle-ear cultures when episodes of AOM were diagnosed (112




Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
