Fig. 3.1
A normal tympanic membrane and normal tympanic membrane with labels. (a) Lateral process of malleus (b) tympanic annulus (c) chorda tympani (d) incudostapedial joint (e) handle of malleus (f) shadow of Eustachian tube (g) shadow of round window niche (h) promontory (floor of middle ear) (i) umbo (j) bulge of anterior external auditory canal wall (k) hypotympanic air cells
Table 3.1
Findings on pneumatic otoscopy
Color | Position | Translucency | Mobility |
|---|---|---|---|
Gray | Normal | Translucent | Normal |
Yellow | Bulging | Semi opaque | Increased |
Amber | Retracted | Opaque (dull) | Decreased |
White | No movement | ||
Red | |||
Blue |
In contrast to a normal tympanic membrane, the exam findings in otitis media are quite different. Otitis media with effusion (Fig. 3.2a) will often present with complaints of fullness and possibly decreased hearing. It may also be asymptomatic. Exam findings in serous OME are usually a yellow or amber tympanic membrane with normal or retracted position. Mobility is usually impaired and air bubbles may be seen in the fluid in the middle ear space. Mucoid OME has a yellow to white or creamy color with a bulging, normal or retracted position. Mobility is usually decreased (Fig. 3.3). The findings in OME contrast with the findings in AOM. Here the patient may or may not complain or ear pain. The tympanic membrane will show prominent vessels on exam. There will be purulent effusion in the middle ear space and the tympanic membrane will appear in a normal or bulging position. Mobility will be decreased (Fig. 3.4).
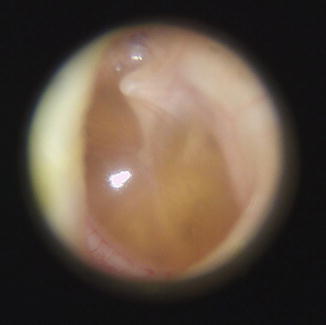

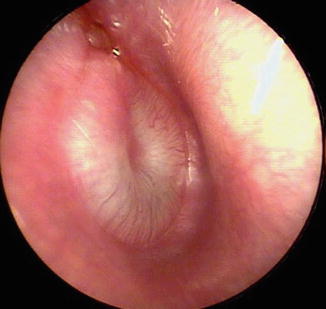
Fig. 3.2
Serous otitis media in left middle ear
Fig. 3.3
Mucoid effusion with bubbles in right middle ear
Fig. 3.4
AOM of right ear
Of paramount importance is making the correct diagnosis for a patient with otitis media as the diagnosis will determine the treatment. The 2013 clinical practice guideline on the diagnosis and management of AOM from the AAP [10] built upon and further clarified diagnostic criteria set forth in the 2004 AAP guideline [38]. The earlier guideline used a 3 part definition of AOM with 1. Acute onset of symptoms, 2. Presence of MEE, and 3. Signs of middle ear inflammation. Criticisms of these criteria were that they lacked precision to exclude OME and permitted the diagnosis of AOM in cases of acute onset of symptoms with otalgia and MEE but without other signs of inflammation on otoscopy. Additionally, the 2004 guideline included a category for “uncertain diagnosis” which may have permitted diagnosis of AOM without clear visualization of the tympanic membrane. The 2013 guidelines qualify these criteria and states that the diagnosis of AOM :
1.
Should be made in children who present with moderate to severe bulging of the TM or new onset otorrhea not due to acute otitis externa.
2.
Should be made in children who present with mild bulging of the TM AND recent onset (less than 48 h) of ear pain (holding, tugging, rubbing of the ear in a nonverbal child) or intense erythema of the TM.
3.
Should NOT be made in children who do not have MEE (based on pneumatic otoscopy and/or tympanometry)
The new guidelines place great importance on the otoscopic exam of the patient to make the correct diagnosis. A study by Karma et al [39] looked at over 2900 children over the course of 2 years at 2 separate sites—totaling over 11,000 visits. Physical exam findings, the color, position and the mobility of the TM were recorded. AOM was diagnosed if the child had MEE and fever, earache, irritability, ear rubbing or tugging simultaneous other upper respiratory symptoms, vomiting or diarrhea. Tympanocentesis was performed but no culture was obtained. Of the acute visits in the study, MEE was found in 84.9 and 81.8 % at the two sites. Of the exam findings, a cloudy, bulging TM with impaired mobility was the best predictor of AOM. Impaired mobility had the highest sensitivity (95 %) and specificity (85 %). Individually, cloudiness was 74 % sensitive and 93 % specific. Bulging TM was only 51 % sensitive, but 97 % specific. Several other studies support the value of the bulging TM on physical exam [40, 41] moderate to severe bulging of the TM is the most important characteristic in the diagnosis of AOM [10].
In looking at the presenting symptoms of AOM, ear pain had the highest combined positive likelihood ratio (3.0–7.3) in a 2003 review by Rothman et al. [42]. In three studies cited, Niemela et al reported 54 % sensitivity and 82 % specificity of ear pain [43]. Heikkinen reported 60 % sensitivity and 92 % [44] and Ingvarsson reported 100 % sensitivity, though did not report specificity [45].
Despite its usefulness as a symptom to be used in the diagnosis of AOM, ear pain is only present in 50–60 % of children with AOM [42]. Other signs, restless, ear rubbing, fever, non-specific respiratory complaints, diarrhea were not helpful in diagnosis AOM.
Takata et al reviewed the accuracy of eight methods of diagnosing OME [46]. Pneumatic otoscopy was found to have the best performance with a sensitivity of 94 % (95 % CI 92–96 %) and a specificity of 80 % (95 % CI 75–86 %). Pneumatic otoscopy was compared to acoustic reflectometer, portable tympanometry and several variations of professional tympanometry. All included studies used myringotomy as internal diagnostic comparison. Only one of the included studies on pneumatic otoscopy was performed by validated otoscopists [47]. Additionally, the author noted that audiometry, binocular microscopy and non-pneumatic otoscopy could not be included in the analysis because of inadequate evidence. In a small study, Rogers et al looked at 201 ears in 102 patients and found that binocular microscopy by a staff pediatric otolaryngologist was the most sensitive in diagnosing OME with 88.0 % sensitivity (95 % CI 81.4–94.7) and 89 % specific (95 % CI 83.1–94.9). Resident binocular microscopy was the next most sensitive, followed by staff pneumatic otoscopy and resident pneumatic otoscopy. Thus, as would be expected, there is improved performance garnered from additional years of training and experience. Of note, however, even the resident exam was more specific that the tympanometer 78.4 % (95 % CI 70.4–86.4) to 47.7 % (95 % CI 38.3–57.1).
Tympanometry
Tympanograms are widely used as an adjunct to the pneumatic otoscope in the clinical evaluation of children with otitis media. Most primary care clinics today use a low frequency probe tones (220–226 Hz) [48] and classify results as Jerger A, B or C [49]. Type A represents normal compliance of the tympanic membrane, Type B no compliance and Type C negative pressure in the middle ear space. Tympanometry with low frequency probe is reliable for infants greater than 4 months and has good inter-observer agreement of the curve patterns in routine clinical practice [50]. Despite the relatively low specificity for predicting MEE with a type B tympanogram, 47.7 % in the Rogers study and 74.5 % in the Takata study, tympanometry can guide the clinician in clinical decision making. If the definition of abnormal results on tympanogram are expanded to include both type B as well as type C2 (tympanic peak pressures between −200 and −400 daPa) the sensitivity and specificity, according to data from Takata, improve to 93.8 % (95 % CI 91.1–96.4) and 61.8 (95 % CI 41.5–82.1) respectively. Although not as precise as pneumatic otoscopy, this definition of abnormal result may be the most useful for ruling out OME [51].
Other modalities that have been used to assess the status of the middle ear and aid in diagnosis of otitis media are 1000 Hz tympanometry, multifrequency tympanometry and wideband acoustic transfer functions specifically wideband reflectance (WBR). Data suggest that these methods are useful in specific situations to determine the presence or absence of MEE, especially 1000 Hz tympanometry and WBR as applied to screening in infants. Continued research is needed to define their exact role as diagnostic tools [51]. Acoustic reflectometry (AR) is another tool that can be used in the diagnosis of MEE. Modern acoustic reflectometers analyze the frequency spectrum of reflected sound. They have been shown to be nearly equivalent to pneumatic otoscopy and tympanometry in terms of sensitivity and specificity [52]. AR offers a potential advantage over tympanometry and pneumatic otoscopy in that it does not require an airtight seal.
Hearing Testing
Audiometry may be used in the assessment of patients with otitis media . It is recommended when MEE has been present for 3 months or greater or when there is concern for speech delay, learning problems or when a significant hearing loss is suspected. Audiometric results with otitis can range from normal to moderate hearing loss (0–55 dB). The average hearing loss is 25 dB hearing level (HL) and approximately 20 % of ears exceed 35 dB HL [50]. The hearing loss is conductive in nature and secondary to the effusion in the middle ear space or the retraction of the TM. It causes an overall stiffening of the middle ear transduction mechanism (TM and ossicles) that generally affect lower frequencies before higher frequencies [7].
Conventional audiometry can be performed for children greater than 4 years of age. Screening conventional audiometry can be performed in the primary care setting. For younger children and for those for whom conventional audiometry is not appropriate, comprehensive audiologic assessment should be obtained. This includes air conduction and bone conduction thresholds for pure tones, speech detection and speech reception thresholds. For children aged 6–24 months visual reinforced audiometry may be used. Play audiometry is typically used for children 24–48 months [53]. Assessment of individual ear thresholds using either headphones or in canal inserts is typically possible with children older than 24 months. If this is not possible, then assessment is done under soundfield conditions and the responses can only comment on the better hearing ear.
Auditory brainstem response (ABR) testing and otoacoustic emission (OAE) testing are not tests of hearing but rather assessments of the integrity of the auditory pathway. They are objective measures used in situations when behavioral testing is not possible (e.g. newborn screening), but they should not be used as a substitute for behavioral audiometry [53].
Treatment
Medical
As it can be seen from the discussion above, the correct diagnosis of otitis media drives all further management of the patient. Risks of treatment need to be weighed against the natural history of otitis media. A recent Cochrane review reported that up to 82 % of children with acute otitis media will improve spontaneously [54]. In terms of treatment for otitis media, it can broadly be broken down into medical and surgical with the mainstays being antibiotics, both oral and oto-topical. The mainstay of surgical therapy is tympanostomy tubes.
The classic study by Howie on the bacterial etiology of otitis media using placebo therapy and serial tympanocenteses revealed that the spontaneous resolution rate of otitis media is, to a large extent, determined by the specific pathogen [55]. AOM caused by S. pneumoniae is less likely to resolve on its own than that caused by H. influenzae. By contrast, the vast majority of M. catarrhalis ear infections resolve with placebo and serial tympanocentesis. The fact that suppurative complications of otitis media such as mastoiditis are almost never caused by M. catarrhalis further underscores the low pathogenic potential of this organism in AOM.
Since 2004 the AAP and the American Academy of Family Practice have emphasized a selective approach to the treatment of otitis media with the publication of clinical practice guideline for the diagnosis and management of AOM [38]. In 2013, the AAP released a comprehensive peer-reviewed revision to this guideline that incorporated recent data on the effect of PCV on the microbiology of AOM, as well as address some of the controversial issues raised by the original guideline [10]. These guidelines provide specific and stringent criteria for the diagnosis of AOM, as well as an option for initial observation vs. therapy in selected patients. They also address appropriate choices on antibiotic agents, pain management and preventive measures.
The AAP guideline provides a number of clinical scenarios to determine whether antibiotics are indicated or observation is an option [10]. These are based on the clinical presentation, severity of symptoms and the age of the child, and include:
(a)
Severe unilateral or bilateral AOM, characterized by moderate/severe otalgia, otalgia for at least 48 h or fever ≥39 C, should be immediately treated, irrespectively of the child’s age.
(b)
Similarly, treatment with antibiotic should be initiated immediately for AOM with otorrhea.
(c)
Non-severe bilateral otitis media in young children (6–23 months) should also be treated with antibiotics.
(d)
Non-severe unilateral AOM in young children (6–23 months) should be either treated with antibiotics or observation with close follow up can be an option based on a joint decision with the caregivers.
(e)
Non-severe AOM (unilateral or bilateral) in children 24 months or older should be either treated with antibiotics or offered observation based on a joint decision with the caregivers.
The guideline also emphasizes that if observation is elected, antibiotic therapy should be started if the child worsens or fails to improve within 48–72 h [10].
Most experts agree that amoxicillin for a full course of 10 days continues to be an effective agent following the introduction of PCV and should remain as the first-line agent of choice. Advantages of amoxicillin include reasonable efficacy in AOM , a good safety profile, low rates of gastrointestinal upset, acceptable palatability, and inexpensive cost compared with other commonly used second-line antibiotics. High-dose amoxicillin (80–90 mg/kg/day) is preferred to avoid suboptimal concentrations of amoxicillin in middle ear effusion [56, 57]. Despite the fact that high-dose amoxicillin is unlikely to be effective against β-lactamase–producing H. influenzae (56–64 % β-lactamase–positive) and M. catarrhalis (virtually 100 % β-lactamase-positive), current data support its effectiveness in new-onset AOM, although its continued effectiveness will need to be monitored [22].
Of the available FDA-approved antibiotic therapies for AOM (Table 3.2), only a handful are endorsed by the current AAP guideline [10], as there is concern or lack of information about the effectiveness of the rest of them. Intramuscular ceftriaxone, although recommended by the AAP as second-or third-line treatment, is not commonly used by clinicians for uncomplicated refractory AOM.
Table 3.2
Currently available FDA-approved antibiotics for AOM
FDA-approved antibiotics for the treatments of AOM | ||||
|---|---|---|---|---|
Frequency of use | Penicillins | Cephalosporins | Macrolides | Others |
Common | Amoxicillin | Cefdinir | ||
Amoxicillin-clavulanate | Cefprozil | |||
Uncommon | Cefaclor | Azithromycin | ||
Cefixime | Clarithromycin | |||
Cefpodoxime proxetil | ||||
Ceftibuten | ||||
Cefuroxime | ||||
Ceftriaxone | ||||
Rare | Cephalexin | Erythromycin | Trimethoprim-sulfamethoxazole | |
Ethylsuccinate/sulfisoxazole | ||||
The most commonly used second-line agent is amoxicillin-clavulanic acid. A formulation of this antibiotic that contains these agents in a 14:1 ratio allows for a high-dose regimen without excessive rates of diarrhea and has improved tolerability [58]. Amoxicillin-clavulanate is also preferred in a patient who has received amoxicillin in the past 30 days or has a history of recurrent AOM unresponsive to amoxicillin [10].
Several acceptable alternative initial therapies are available for penicillin-allergic patients. Cefpodoxime, cefuroxime, and cefdinir have been found to be reasonably effective in the treatment of AOM [10, 38]. Although in the past caution has been emphasized when prescribing cephalosporins to patients with true penicillin allergy, recent studies have shown that the true incidence of cross-sensitivity is almost negligible with the 2nd and 3rd generation cephalosporins endorsed by the APP guideline (cefpodoxime, cefuroxime and cefdinir) [59, 60].
Clindamycin has activity against most strains of the pneumococcus, but no activity against H. influenzae or M. catarrhalis, and its use should probably be reserved for cases in which S. pneumoniae has been cultured from middle ear fluid, or when this organism is strongly suspected. If clindamycin is used in an empirical fashion in a patient that has failed with a conventional regimen, it may be prudent to give it in combination with an agent that is β-lactamase stable, such as a second or third generation cephalosporin.
Studies have shown that one intramuscular injection of ceftriaxone (50 mg/kg) is as effective as a 10-day course of amoxicillin-clavulanate for the initial treatment of AOM [61]. For treatment of previously unresponsive cases, 3 consecutive days of therapy is superior to a single injection [62]. However, the use of ceftriaxone for treatment of otitis media should not be routine. A single dose of intramuscular ceftriaxone has been shown to increase penicillin resistance among the pneumococci colonizing the nasopharynx [63]. Although some refractory cases of AOM due to multiple resistant organisms will respond to a 3-consecutive-day schedule of intramuscular ceftriaxone [10], this approach to therapy is painful and often inconvenient.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


