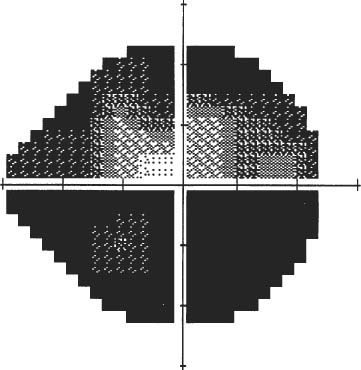
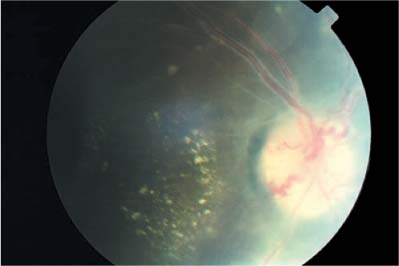
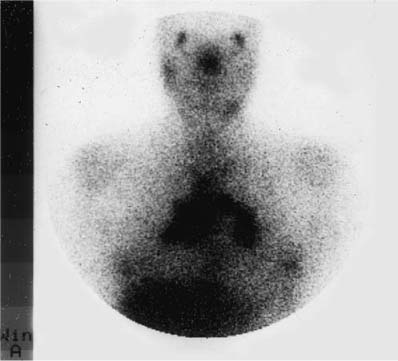
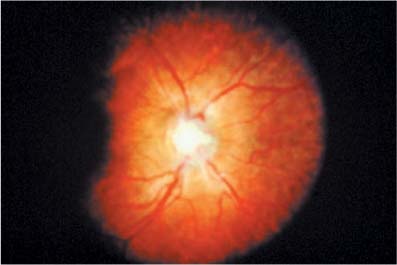
Chapter 21 This chapter deals with other forms of inflammatory optic neuropathy aside from the idiopathic optic neuritis that is so closely linked to multiple sclerosis and is described in Chapter 20. The first priority is to realize that the patient does not have a classic case of optic neuritis. There are “red flags” (in both the patient history and the examination) that should alert you of this possibility. These include: Whenever you encounter these red flags, you should expand your differential diagnosis to include several of the entities that are discussed in this chapter, and undertake a directed diagnostic evaluation. However, there is rarely anything specific about the ocular involvement in these forms of inflammatory optic neuropathies that would allow one to make a specific diagnosis. Thus, the systemic and laboratory evaluation are crucial to instituting specific therapy. Sarcoidosis is a multisystem disease of unknown etiology. There are multiple theories about its pathogenesis, including frank infection or allergic responses to organisms that are ubiquitous and typically nonpathogenic, including mycobacterial species.1 Sarcoid has a predilection for the lungs and for glandular tissue such as the lacrimal, submandibular, and parotid glands. The urgency of evaluation is linked to how long the patient has had visual loss. If the visual loss has been static for many months and optic atrophy is present, then there is less urgency to the evaluation. Conversely, when the visual loss is acute, sarcoid optic neuropathy may respond very rapidly to therapy; thus, rapid evaluation within days may be beneficial. There is often nothing about the visual presentation of the case of truly isolated acute sarcoid optic neuritis that reliably distinguishes it from typical optic neuritis. The prolonged course over time, the development of other signs and symptoms, and on occasion, the profound visual improvement with the initiation of systemic corticosteroid therapy (or, conversely, the rebound to steroid taper) may help identify these cases. Sarcoidosis is a worldwide disease that may be seen in all ethnic groups, though in the United States it is of higher incidence in African Americans, with females more often affected than males. The peak incidence is in young adults. Neurologic disease is seen in 5 to 16% of cases, and ophthalmic disease is seen in ~20 to 25% of all patients with sarcoidosis, higher if there is pulmonary disease.1,2 There are several types of optic neuropathy in sarcoidosis: (1) nonspecific inflammation indistinguishable from idiopathic optic neuritis; (2) infiltration of the optic nerves and/or sheaths, mimicking an optic nerve mass such as a glioma or meningioma; (3) direct compression of the nerve, such as from an orbital granuloma; and (4) parachiasmal involvement. Thus the extent of the visual loss and pattern of the loss may be quite variable, ranging from a small central scotoma noted in one eye, to peripheral constriction, to bitemporal field loss. Pain is variable. It is our impression that it is more often seen in cases with uveitis and less frequently in cases with chiasmal and posterior optic nerve involvement. Depending on the location and the mode of optic nerve involvement, acuity may be completely spared or it may be severely affected. Depending on the location and mode of optic nerve involvement, the visual field may show central scotomas, peripheral constriction, bitemporal field defects, or if the optic tract is involved, homonymous hemianopsia. Optic nerve sarcoidosis is one of the entities that is suggested by simultaneous optic neuritis and raised intracranial pressure (as are tuberculosis and syphilis, discussed later). In these cases, one may see peripheral field loss and acute central visual loss (Fig. 21–1). If the visual loss is unilateral or asymmetric, one typically sees a relative afferent pupillary defect. If it is bilateral and symmetric, one may not. The optic disc may be normal (e.g., retrobulbar involvement) or may be swollen. There may be a granuloma visible on the optic nerve head (Fig. 21–2). The anterior manifestations of ocular sarcoidosis include conjunctival nodules, keratic precipitates, and iris nodules (Busacca at the border of the iris, Koeppe nodules in the substance of the iris). Other manifestations include uveitis and lacrimal gland enlargement. More posteriorly other signs, such as vitreous opacities, snowballs, or candle wax drippings are seen. In the retina, one may see periphlebitis (Fig. 21–3). This finding is important because, although it may be seen in optic neuritis, it is usually not extensive, and recognizing it in the presence of an ocular or neurologic symptom may be the first real step in diagnosing occult sarcoidosis. Although in some cases the periphlebitis is obvious, the detection of periphlebitis may be aided with a fluorescein angiogram. Choroidal granulomas are not rare (Fig. 21–4), and are seen as deep to the retina. Sarcoid may rarely include a retinal granuloma.3 FIGURE 21–1 Visual field of right eye of patient with presumed sarcoid optic neuropathy with acuity of counting fingers OS and 20/30 OD. The color vision was preserved. This field loss, with color vision preserved and good acuity, is typical of optic perineuritis. FIGURE 21–2 Optic nerve granuloma in sarcoid optic neuritis. The acuity was 20/20, the granuloma resorbed, and the acuity returned to 20/20 with corticosteroid therapy. If the patient is known to have sarcoidosis, and develops an optic neuropathy in the course of the already established disease, the diagnosis is usually by inference unless something about the clinical course suggests that sarcoid is not the etiology. In the patient without established sarcoidosis, the diagnosis is more challenging. Often it is suggested by other ocular signs that suggest sarcoid or similar diseases, such as periphlebitis or choroidal granuloma. However, in the patient with no other findings, and only an atypical course for optic neuritis as the red flag, ancillary testing plays a key role. FIGURE 21–3 Periphlebitis in a patient with optic neuritis. This finding establishes sarcoidosis as a key element in the differential diagnosis. FIGURE 21–4 Choroidal granuloma in a patient with sarcoidosis. In sarcoid, there are many forms of optic neuropathy. In the case where a granuloma is acting like a mass lesion and compressing the nerve, a lesion may be seen. In cases with infiltrative optic neuropathy, there may be scant, if any, findings. Magnetic resonance imaging (MRI) is the imaging modality of choice in neurosarcoidosis. In some cases, one may see intense enhancement of the optic nerve. The chiasm and or tract may enhance (Fig. 21–5). In other cases, mild enhancement of the optic nerve may not be strongly suggestive of sarcoid, but enhancement of the meninges, particularly at the base of the skull just anterior to the chiasm (an area often overlooked) may suggest sarcoidosis. FIGURE 21–5 T1-weighted magnetic resonance imaging (MRI) scan with gadolinium showing enhancement of optic tract. The hallmark of neurosarcoidosis is lymphocytic pleocytosis. Elevated protein levels may also be seen. A normal spinal fluid does not absolutely rule out that sarcoid is the etiology of the optic neuritis. Contrary to what is believed by many, neither an abnormal chest x-ray nor an elevated angiotensinconverting enzyme (ACE) level is necessary for diagnosing sarcoid. If one is suspicious of sarcoidosis, an aggressive workup at presentation, including chest x-ray, ACE, gallium scan (Fig. 21–6), purified protein derivative (PPD), anergy panel, pulmonary function tests, and 24-hour urine calcium, may help to establish the diagnosis, in addition to the previously mentioned MRI scanning and lumbar puncture. The typical pathology is the noncaseating granuloma, although rarely one may encounter caseation. In general, it is wise to seek a tissue diagnosis at onset, as well as to stage the patient for the extent of the systemic disease process. The tissue diagnosis is best established when one biopsies obvious lesions, such as a lacrimal or conjunctival nodule, or when the gallium scan points out abnormal tissue that may be biopsied. If the patient has been on steroids for a period of time before the diagnosis is entertained, abnormal laboratory tests or biopsy may be “normalized” by the steroid therapy, and one may have to repeat the evaluation again 2 to 3 months after the steroids have been weaned. FIGURE 21–6 Positive gallium scan in a patient with sarcoid optic neuritis, demonstrating uptake in both hila, the lacrimal glands, one parotid gland, and one submandibular gland. Systemic sarcoidosis that involves the nervous system is typically treated with corticosteroids; if this fails, other immunomodulatory agents such as methotrexate, azathioprine, cyclophosphamide, cyclosporine, and thalidomide may be employed. Sarcoid optic neuropathy is an uncommon disease best cared for by those who have experience with it. If the diagnosis is proven, or strongly suspected, we recommend referral to a neuroophthalmologist and an internal medicine subspecialist familiar with the systemic illness to direct the evaluation, staging, and therapy of the disease process. Tuberculosis is an infection caused by Mycobacterium tuberculosis. Unfortunately, tuberculosis (TB) is enjoying a worldwide resurgence, in part due to the prevalence of acquired immune deficiency syndrome (AIDS). Tuberculous optic neuritis is a rare disease, with little mentioned in the literature in the past 30 years. Unfortunately, this means that there are few physicians who have extensive experience with this disorder. This disease must be considered in anyone with an atypical optic neuritis, particularly if one is contemplating starting corticosteroid therapy (which could reactivate undiagnosed tuberculosis). As in any acute optic neuritis, the patients should be seen as soon as possible. There are two scenarios in which tuberculous optic neuritis should be suspected. One is the patient with known tuberculosis who develops an optic neuropathy. The other scenario, infrequently encountered, is when a patient with an atypical course of optic neuritis is found to have tuberculosis as a result of search for a systemic cause. TB is now a worldwide health problem, partly due to its reemergence in the setting of the AIDS epidemic. Despite this fact, one must remember that TB may be seen in a patient with a competent immune system even in the absence of pulmonary involvement. The kind of visual loss seen depends on the mode of optic nerve involvement. TB may affect the anterior visual pathways by acting like a mass (e.g., the tuberculoma), by direct infiltration of the optic nerve, or by a process secondary to tuberculous meningitis, with a subset of the latter being the classic form of opticochiasmatic arachnoiditis. This is seen because the inflammation of tuberculous meningitis is typically worse in the region of the basilar meninges. The presence or absence of pain is unreliable in the diagnosis of tuberculous optic neuritis. The loss of acuity can be mild or profound, and of slow or rapid onset. The mode of involvement may define the form of visual loss. Direct optic nerve infiltration/inflammation can cause a central scotoma, whereas involvement due to chronic meningeal inflammation can result in peripheral field loss. When the afferent visual system is involved, impaired direct light response is seen. If asymmetric, this will manifest as a relative afferent pupillary defect. The optic disc may initially be normal in appearance, edematous, or atrophic. Other ophthalmic signs include granulomatous uveitis, vitreitis, choroiditis, dacryoadenitis, and myositis. When there is tuberculous meningitis, cranial neuropathy may be seen. Neuroimaging in tuberculosis does not yield many specific findings. Enhancement of the optic nerves or meninges may be seen, possibly associated with hydrocephalus, cerebral edema, and tuberculomas. Lumbar puncture findings in tuberculosis are not specific. Elevated protein with mild pleocytosis is seen.4 The glucose may be very low. The demonstration of tuberculous bacteria by smear or culture is the gold standard, but polymerase chain reaction is a promising and sensitive adjunct.5 Diagnostic testing for tuberculosis has traditionally included chest x-ray, PPD, sputum smear, aspiration of gastric contest for staining/culture, and fiberoptic bronchoscopy with biopsy/washings. Recently, polymerase chain reaction has been established as a sensitive tool. Tuberculosis therapy includes isonicotinic acid hydrazide (INH), ethambutol, rifampin, streptomycin, and pyrazinamide. The therapeutic recommendations differ in the immunecompromised and the immunecompetent, and recommendations change rapidly. Furthermore, as the worldwide tuberculosis epidemic linked to AIDS has continued, there has been a large increase in cases demonstrating multiple drug resistance. When faced with neurotuberculosis, the physician should seek the advice of an infectious disease specialist. One must remember to be vigilant for the development of iatrogenic optic neuropathy from the use of antituberculous agents, notably seen with ethambutol and INH. Corticosteroid therapy for TB optic neuritis is controversial and should not be used unless an infectious disease specialist and a neuroophthalmologist, neurologist, or ophthalmologist experienced in TB optic neuritis concurs with their use. There is no set standard for the follow-up of cases of tuberculous optic neuritis. Intervals of care and visual assessment should be linked to the duration of illness at the point that the patient is diagnosed. Syphilis, also known as lues, or the Great Imitator, is a bacterial infection caused by the spirochete Treponema pallidum. Like tuberculosis, its incidence was waning until the era of AIDS, which has led to new challenges in diagnosis and therapy. If a patient with known syphilis presents with acute visual loss and optic neuritis is suspected, evaluation is emergent.
OTHER INFLAMMATORY OPTIC NEUROPATHIES
HISTORY RED FLAGS
 Simultaneous bilateral involvement of the optic nerves
Simultaneous bilateral involvement of the optic nerves
 Documented progression beyond a week after onset
Documented progression beyond a week after onset
 Recurrence, especially if this occurs as corticosteroids are being tapered
Recurrence, especially if this occurs as corticosteroids are being tapered
 Presence of other neurologic symptoms of simultaneous onset (aside from local ocular pain)
Presence of other neurologic symptoms of simultaneous onset (aside from local ocular pain)
 Presence of an acute illness in the immediate period before the onset of the optic neuritis (e.g., fevers, acute asthma)
Presence of an acute illness in the immediate period before the onset of the optic neuritis (e.g., fevers, acute asthma)
 Presence of a systemic illness that may cause a secondary optic neuritis
Presence of a systemic illness that may cause a secondary optic neuritis
EXAMINATION RED FLAGS
 Pupillary findings inconsistent with multiple sclerosis, such as Argyll-Robertson pupils
Pupillary findings inconsistent with multiple sclerosis, such as Argyll-Robertson pupils
 Proptosis
Proptosis
 Anterior uveitis
Anterior uveitis
 Ophthalmoplegia
Ophthalmoplegia
 Sensory involvement of the trigeminal nerve
Sensory involvement of the trigeminal nerve
 Retinal findings such as periphlebitis, arterial occlusive disease, granulomas, or macular stars
Retinal findings such as periphlebitis, arterial occlusive disease, granulomas, or macular stars
 Presence of another cranial nerve sign or another neurologic sign simultaneous in onset to the optic neuritis
Presence of another cranial nerve sign or another neurologic sign simultaneous in onset to the optic neuritis
SARCOIDOSIS
URGENCY OF EVALUATION
DIAGNOSIS
Symptoms
Demographics
Visual Loss
Pain
Signs
Visual Acuity
Visual Field
Pupils
Optic Disc
Other Findings
ANCILLARY TESTING

Neuroimaging

Lumbar Puncture
Laboratory Tests
Pathological Diagnosis
THERAPY
FOLLOW-UP AND REFERRAL
TUBERCULOSIS
URGENCY OF EVALUATION
DIAGNOSIS
Symptoms
Demographics
Visual Loss
Pain
Signs
Visual Acuity
Visual Field
Pupils
Optic Disc
Other Abnormalities
ANCILLARY TESTING
Neuroimaging
Lumbar Puncture
Laboratory Tests
TREATMENT
FOLLOW-UP AND REFERRAL
SYPHILIS
URGENCY OF EVALUATION
DIAGNOSIS
Symptoms
Demographics
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


