Several factors influence the results in ossiculoplasty, including the middle ear environment, the surgical technique, and the qualities of the prosthesis. There is no question that the first of these is the most important determinant of long-term hearing outcomes with ossiculoplasty in the chronic ear, but it is also the most difficult to understand for both novice and experienced ear surgeons. Prognostic features of the middle ear environment will be discussed later in this chapter in the context of results but should be considered early in the evaluation of a patient undergoing surgery for the chronic ear. By considering these during the preoperative assessment, patient stratification, realistic expectations, and informed consent are facilitated. The next most important factor influencing results is surgical technique, which will be the main focus of this chapter. By combining a fundamental understanding of middle ear mechanics and the consistent anatomical relationships that exist in even the diseased middle ear, the surgeon can have a direct impact on results. As long as good surgical technique is adhered to and care is taken to reinforce the reconstruction based on the middle ear environment, the qualities of the modern prosthesis are least important.
29.2 Patient Selection
When a patient is considered for tympanoplasty or ossiculoplasty, a thorough history, examination, and audiometric evaluation should be performed on both ears. Otoscopy and pneumatic insufflation under the binocular microscope, following careful removal of debris, provide a wealth of information. The results of the audiogram should always be correlated with the physical exam, including Weber and Rinne tuning fork tests, especially when a masking dilemma is present. If the audiogram and tuning fork exam do not agree, surgery should not be performed until this is reconciled.
A preoperative audiogram can be helpful in suggesting underlying pathology. Generally, a perforation will cause a conductive hearing loss of 5–40 dB, depending on its characteristics.1 When the tympanic membrane is intact, a conductive hearing loss greater than 35–40 dB strongly suggests the possibility of ossicular chain dysfunction. Furthermore, the pattern of hearing loss may be typical of particular scenarios; for example, fixation of the lateral ossicular chain generally causes a prominent low-tone conductive hearing loss having an air-bone gap (ABG) that partially closes in the middle and high frequencies. In comparison, stapes fixation tends to affect the middle and high frequencies to a relatively greater degree.2
The status of the Eustachian tube will impact surgical outcomes, yet there is no consensus on the optimal way to reliably assess its function. Auto-inflation using the Valsalva or Toyenbee maneuver is helpful, albeit a non-physiologic test of tubal patency. Details of Eustachian tube assessment are outlined in Chapter 15. The clinical status of the contralateral ear likewise can provide insight into tubal maturity and function in the diseased ear.3 As part of the Eustachian tube evaluation, the nose should be examined so that allergy, adenoiditis, and rhinosinusitis can be treated in an effort to promote optimized tubal function. Furthermore, aggressive medical treatment of infection involving the ear itself should be undertaken prior to surgery, including aural toilet and ototopical agent application.
Once patient assessment is complete, a few general rules should be applied to surgical candidacy. First, one should avoid elective surgery on an only-hearing ear as much as is reasonably possible. Second, when bilateral disease is present, surgery should be undertaken on the worse-hearing ear in the absence of any other compelling reason to do otherwise on account of underlying disease. Finally, special consideration should be given to the timing of surgery in the pediatric patient.
29.3 Qualities of the Prostheses
29.3.1 Materials
Numerous synthetic materials have been used in ossicular implants, such as porous high-density polyethylene, plastics, bioactive glass, stainless steel, gold, titanium, and hydroxyapatite (HA), the last two currently being most common in the United States and Europe. Promising short-term results continue to be published for most of these materials,4 but the long-term histological fate is uncertain in many instances. Each of the two most common currently used materials, HA and titanium, has advantages and disadvantages. Hydroxyapatite is produced by molding, resulting in smooth edges and grooves that have benefit when placed against the tympanic membrane and notched under the malleus, compared with the sharp stamped edges of titanium. Titanium, however, is lighter and more malleable, which makes it possible to change the angle of the prosthesis to facilitate the conical shape of the drum and to create a cradle for secure fit to the stapes. There seems to be no clear acoustic advantage of one over the other, with the results dictated more by the technique used and experience of the surgeon.5 A detailed discussion of biomaterials can be found in Chapter 8.
29.3.2 Prosthesis Design
Much has been discussed with regard to prosthesis design, including ideal weight, length, and general shape. However, most studies are performed with laser vibrometry in non-diseased cadaver bones, and whether or not these results can be extrapolated to the diseased ear is yet to be appreciated. The ideal weight of the prosthesis has been examined by a number of investigators. Some researchers suggest that a lighter prosthesis in the range of 3–4 mg functions more effectively6 whereas others have suggested a weight between 10–35 mg to yield the best acoustic response with the vibrometer.7 In the latter study, prostheses above this weight would cause low-frequency displacements to fall out of acceptable ranges, and prostheses below this weight would lead to high-frequency losses. Interestingly, the human incus normally weighs 30–40 mg. Realistically, prosthesis weight is probably not of critical importance in the diseased middle ear as long as it falls within these acceptable ranges. Cartilage is usually placed on top of the prosthesis head to present extrusion in most cases, and the added weight to the reconstruction appears to have no detrimental effect on the hearing result regardless of which material is used.
There are a myriad of prosthesis shapes available and an equal number of surgeons advocating one over the other. Suffice it to say that the goal of ossiculoplasty is to provide a reconstruction with immediate stability and long-term durability. It should comply with as many of the gain-benefit principles of ossicular acoustic mechanics as is practical. As such, the more stable the initial reconstruction, the higher likelihood of a good long-term outcome.
Most synthetic prostheses are divided into partial ossicular replacement prostheses (PORPs), to be used with an absent incus but present stapes superstructure, and total ossicular replacement prostheses (TORPs), which are used when both the incus and stapes superstructure are absent or in poor anatomical position. A PORP usually consists of a head to make contact to the tympanic membrane and/or malleus and a shaft or cradle to facilitate the stapes capitulum and superstructure. A TORP is similar in design but with a shaft or wire that runs directly to the footplate. Both PORPs and TORPS can be further subdivided into designs that are intended to directly impact the undersurface of the drumhead and those that are intended to engage the manubrium of the malleus.
Most ossicular prosthesis designs are inherently unstable in that they are top-heavy and will tend to tip unless adequately supported by the reconstruction technique. This effect can be negated somewhat with a design that is very light, such as titanium, or a head design that shifts the center of gravity over the shaft, as used in some molded HA designs. Short-term stability is likewise facilitated by effective 2-point (preferably bony) fixation. Thus, any design that incorporates the malleus should offer improved stability in that the prosthesis may be “locked” into place between the malleus manubrium and stapes. Furthermore, recent basic science research using infrared laser vibrometry as well as retrospective clinical studies on ossiculoplasty suggest that incorporating the malleus in the reconstruction provides increased acoustic gain.8
The primary goal of ossicular reconstruction is to maximally couple the stapes footplate to the tympanic membrane to re-establish the hydraulic lever effect, which is the most significant mechanism of acoustic gain of the middle ear mechanism. This gain results from the difference between the surface area of the tympanic membrane relative to that of the oval window (usually a ratio of nearly 21:1). Simply placing a prosthesis against the tympanic membrane by no means guarantees that the entire surface area will achieve coupling to the prosthesis, in contrast to placing the prosthesis to the malleus, which is optimally positioned for this purpose.
Flexibility of a prosthesis, allowing it to accommodate the conical shape of the eardrum and to be adjustable in length, would also be considered a relative benefit. As such, the choice of prosthesis is largely dependent on the philosophy of the surgeon but is dictated by the operative technique used.
These techniques can best be illustrated by addressing specific situations encountered in chronic middle ear surgery. The prostheses used in the examples to follow are a combination of HA and titanium of the author’s design, but the surgical technique and anatomical relationships extrapolate to many other synthetic PORPs and TORPs being used today.
29.4 Surgical Technique
29.4.1 General Principles
Although it is generally possible to ascertain the need for ossiculoplasty during the preoperative evaluation based on the audiogram and physical exam, one should be prepared for this contingency in every middle ear surgical case. In addition, it should be considered routine practice to inspect the ossicular chain visually and mechanically every time the middle ear is entered. This can be performed with gentle palpation of the malleus, taking note of concomitant movement of the stapes and visualization of the round window reflex (movement of the membrane and fluid in the niche with palpation of the chain).
29.4.2 Incus Erosion
Due to its location relative to the common pathways of development of cholesteatoma and tympanic membrane atelectasis, as well as its rather tenuous blood supply suspended between the stapes and malleus, erosion of the long process of the incus is the most common ossicular defect. It can be encountered in roughly one-third of cases involving a chronic posterior tympanic membrane perforation due to a variety of factors, such as pressure necrosis, inflammation, and hydrolytic enzymes produced by cholesteatoma matrix.
Although an eroded incus is usually obvious during middle ear exploration, in some cases palpation is required to uncover the presence of a more subtle fibrous union between the stapes and incus. The key factor in this situation is the degree of bony contact remaining, which, if present to some reasonable degree, may compel the surgeon to leave the incus untouched. However, if contact is deficient and movement with palpation is incomplete, reconstruction is recommended.
There are basically two options for reconstruction when incus erosion is present. The first involves an attempt to reconstruct the incudostapedial joint with a Type II (modified) tympanoplasty as discussed in Chapter 27. All of the Type II reconstructive techniques share many of the same theoretical advantages and disadvantages. On the positive side, they reestablish the natural incudomalleal lever with minimal disruption of the normal anatomical relationships and native ossicular connections. The primary disadvantages relate to uncertain long-term durability as little is known about the pathophysiology and natural history of incus necrosis. If erosion is related to avascular necrosis, one may speculate that the remnant of the lenticular process, if used in ossicular reconstruction, may be subject to future loss. Given the relatively small acoustic gain afforded by preservation of the incudomalleal lever, Type II reconstruction of the diseased middle ear (2–3 dB) might not be worth the risk of possible revision.
The most commonly used reconstructive option for incus necrosis involves removal of the incus remnant and reconstruction between the stapes and malleus (or tympanic membrane), generally as a Type III minor columella mechanism. The fundamental anatomic principles governing this reconstruction are the same regardless of the graft or prostheses used. Some key relationships include the vertical height from the stapes capitulum to the plane of the neck of the malleus at the attachment of the tensor tympani tendon (2–2.5 mm) and the horizontal or translational distance from the capitulum to this same point (3–3.5 mm) (▶ Fig. 29.1). Although the malleus manubrium can become rotated medially as an effect of middle ear disease processes, especially along its distal aspect, in the author’s experience, the malleus neck is spared from major rotational variation due to its anchoring attachments, which allow it to be used as a consistent prosthesis target in ossicular reconstruction. This is due to the fact that the axis of malleus medial rotation lies at the attachment of the fan-shaped anterior malleolar ligament to the anterior tympanic spine as well as the underlying tensor tympani tendon, which anchors the malleus to the cochleariform process. In the rare instance where the neck of the malleus is pathologically displaced to an extreme degree, it may be necessary to reposition it, as discussed in Chapter 30.
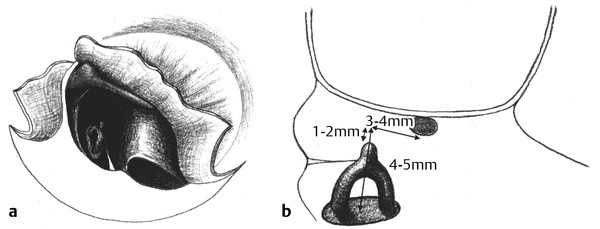
Fig. 29.1 Middle ear anatomy relevant to ossiculoplasty. (a) The tensor tympani tendon and the anterior malleal ligament anchor the malleus neck at the cochleariform process and anterior tympanic spine, respectively. These structures provide stability for tympanoplasty and ossiculoplasty procedures and should not be violated unless necessary. (b) The stapes capitulum is typically 2 mm in height below the undersurface of the neck of the malleus, which is the proper target for the ossicular reconstruction interface. This same site is approximately 3 mm in the lateral dimension from the capitulum; thus, 3 mm of reach is generally required for a sculpted ossicular graft or synthetic prosthesis.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


