Purpose
To examine by histopathology the degree of nerve regeneration in human corneal grafts and to determine the anatomic organization and morphology of the regenerated nerves.
Design
Experimental laboratory investigation.
Methods
Twelve corneal grafts from 12 patients (7 men and 5 women) aged 34-93 (mean, 66.9 years) were included. The most common indication for regrafting was late endothelial failure. The mean duration of graft survival was 6.41 years (range, 1-14 years). The freshly obtained specimens with a narrow rim of host tissue incorporating the graft-host junction were subjected to the acetylcholinesterase method for the demonstration of corneal nerves.
Results
Subbasal nerves were found in 75% and 25% of the grafts at the periphery and center, respectively. They were mostly originated from the host subbasal nerves. Regenerated stromal nerves were detected in 83% of the specimens; half of them showed extension into the center of the graft. A lack of the normal link between the subbasal and stromal nerves was observed and almost all of the regenerated stromal nerves were found to remain within the stroma and did not contribute to the epithelial innervation.
Conclusions
A persistent anatomic disorganization of the corneal nerves in human grafts was found even 14 years after surgery. This could explain the significant reduction of corneal sensation reported in previous studies.
Though penetrating keratoplasty (PKP) is still a common and successful form of organ transplantation, modern corneal transplantation is directed towards replacement of the damaged layer with a healthy one derived from a cadaver donor eye. The procedures employed are endothelial keratoplalsty (EK) for endothelial diseases, deep anterior lamellar keratoplasty (DALK) for stromal diseases, and PKP only when the full thickness of the cornea is involved. The latter 2 procedures involve cutting the nerves along the entire circumference of the cornea. Restoration of corneal graft sensation depends on the regeneration of nerves into the donor graft. In some corneal surgical procedures that involve severing the nerves, such as laser in situ keratomilieusis, wherein nerves are transected at the flap edge, corneal sensitivity returns to normal after several months. In PKP, however, sensitivity is known to be reduced for decades after surgery.
Graft re-innervation has been studied both by histology and by in vivo confocal microscopy. Data from these investigations showed a variable degree of subbasal and epithelial re-innervation of donor grafts with essentially slow and limited stromal innervation. On the other hand, corneal sensation in PKP does not seem to correspond to the actual state of the anatomic re-innervation. Incomplete restoration of corneal sensitivity has been found in a graft where the surface epithelial and subbasal nerve supply was re-established.
The aim of this study was to examine by histopathology the degree of nerve regeneration in human corneal grafts and to determine the anatomic organization and morphology of the regenerated nerves.
Materials and Methods
The study included 12 patients (7 men and 5 women) aged 34-93 (mean, 66.9 years). Common indications for first PKPs were Fuchs endothelial dystrophy in 4 patients, herpes simplex virus (HSV)-related corneal scarring in 2 patients, and limbal stem cell deficiency in 2 patients. Details of all indications are given in Table 1 . Nine of 12 patients were regrafted for late endothelial failure of the previous grafts. Late endothelial failure was defined as a gradual decompensation of a previously clear graft without an apparent cause. Patients’ demographics and clinical data are presented in Table 1 . The repeat PKP procedure was performed by a similar technique in all patients. Corneas were trephined using a disposable suction trephine (Hessburg Barron; Katena Products, Denville, New Jersey, USA) and grafts were then secured into the recipient bed with 16 interrupted 10-0 nylon sutures. The average graft size was 7.5 mm. The freshly obtained failed graft buttons with a narrow rim of host tissue incorporating the graft-host junction were subjected to the Karnovsky and Roots modification of nonspecific acetylcholinesterase (AchE) method for corneal nerve demonstration.
| Patient | Sex | Age | Side | Indication for Previous Graft(s) | Number of Previous Grafts | Type of Previous Graft Surgery | Duration of Graft (Years) | Indication for Last Regraft |
|---|---|---|---|---|---|---|---|---|
| 1 | F | 43 | L | Therapeutic PKP for Pseudomonas corneal ulcer | 1 | PKP | 3.25 | Late endothelial failure |
| 2 | M | 54 | R | Two previous failed grafts after recurrence of HSV keratitis with scarring | 3 | 3 PKPs | 9 | Recurrence in the third graft with graft failure |
| 3 | M | 60 | R | Corneal decompensation following multiple RD surgery | 1 | PKP | 14 | Late endothelial failure |
| 4 | F | 39 | L | Tectonic graft for melting and perforation – diabetes-related neurotrophic ulcer | 1 | PKP | 4 | Late endothelial failure |
| 5 | M | 78 | R | Previous 2 grafts for LSCD | 2 | 1st = DALK 2nd = PKP | 1 | LSC failure |
| 6 | M | 85 | L | Failed graft for HSV keratitis | 1 | PKP | 12 | Late endothelial failure |
| 7 | F | 65 | R | FED | 1 | Triple | 5 | Late endothelial failure |
| 8 | M | 85 | L | FED | 1 | Triple | 9 | Late endothelial failure |
| 9 | F | 83 | L | FED | 1 | Triple | 6 | Late endothelial failure |
| 10 | M | 34 | L | Vascularization, melting and descemetocele for LSCD | 1 | PKP | 8.25 | Late endothelial failure |
| 11 | F | 93 | L | PBK | 1 | PKP | 4.5 | Late endothelial failure |
| 12 | M | 84 | L | FED + BK | 1 | Triple | 1 | Graft rejection with endothelial failure |
Image Analysis and Statistical Testing
The stained corneas were scanned en face using a Hamamatsu NanoZoomer digital pathology (NDP) microscope system (Hamamatsu, Hamamatsu City, Japan). Subbasal and stromal nerves were qualitatively evaluated and the degree of graft re-innervation was assessed by measuring the extent of centripetal movement of nerves toward the central cornea. The graft was divided into 2 zones: the central zone, measuring at a 2.0-mm radius from the center, and the peripheral zone, measuring at a >2.0-mm radius from the graft center. Mann-Whitney U test was used to compare the mean duration of grafts with central and peripheral extension of the stromal nerves. The subbasal nerve plexuses and the number and distribution of the subbasal terminal bulbs were also analyzed.
Control
Six fresh postmortem corneas donated with family consent from 3 deceased patients (1 female, 2 male; mean age 57.3 years) with no previous ocular disease or surgery were also stained with the AchE technique and used as controls. All corneas from this group showed the normal architecture of nerves described in detail previously using the same technique.
Results
Subbasal Nerves
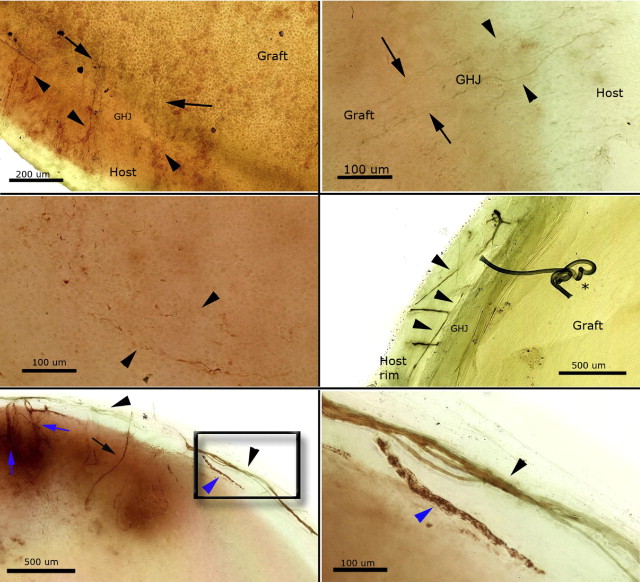
Subbasal nerves were found in 9 of the 12 patients (75%) at the graft periphery and 3 patients (25%) at the center of the graft. Almost all of these nerves originated from the host subbasal nerves and crossed the graft-host junction radially ( Figure 1 , Top left and right). These nerves appeared thin, tortuous, and reduced in number ( Figure 1 , Middle left). The clockwise whorl configuration of the subbasal nerve plexus was not detected in any cornea.
Stromal Nerves
Several stromal nerve bundles from the host tissue appeared to stop at the edge of the grafts ( Figure 1 , Middle right). Some of them demonstrated circumferential extension for several millimeters along the graft-host junction, sometimes accompanied by a blood vessel ( Figure 1 , Bottom left and right). The blood vessels could be easily differentiated from the nerves. They were of irregular thickness and undulating course, and presented a nonhomogenous staining pattern attributable to red blood cells, which were darkly stained, and lack of normal longitudinal striations of axons within the nerve bundles. A detailed description of the differences between nerves and blood vessels, including images, stained by the AchE technique can be found in the Supplemental Material (available at AJO.com ).
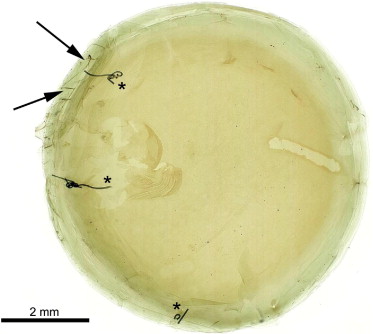
Stromal re-innervation was detected in 10 of 12 grafts (83%). Two grafts (Patients 5 and 7) showed complete corneal denervation with no evidence of single nerve fiber or thick nerve bundle within the peripheral or central corneal stroma ( Figure 2 ) .
In grafts with evident stromal re-innervation, 5 out of 10 demonstrated stromal nerve extension into the central zone (Patients 3, 4, 9, 10, and 11). In the remaining grafts, nerves extended up to 2.2 mm from the edge. The mean duration since surgery of the grafts that showed central extension of the stromal nerves was 7.35 ± 4.06 years, and this was not statistically different from the mean duration of the grafts that showed only peripheral extension of the stromal nerves (6.85 ± 4.55 years) ( P = .917).
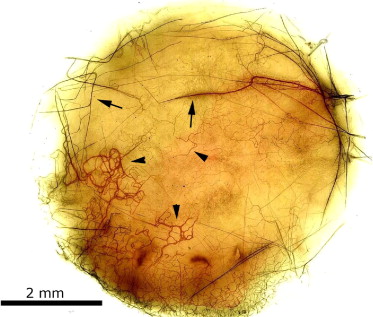
Most of the regenerated nerves were of variable thickness and had either a very tortuous and irregular course or a straight course with abrupt angulations ( Figure 3 ) . The vast majority of these abnormal nerves appeared to remain within the stroma and manifested in 2 different ways: 1) most of them joined each other and formed a very complex network of interconnecting nerves ( Figure 3 , arrowheads); and 2) a few nerves ended abruptly within the stroma and showed characteristic terminal swellings or growth cones ( Figure 4 , Top left and right).
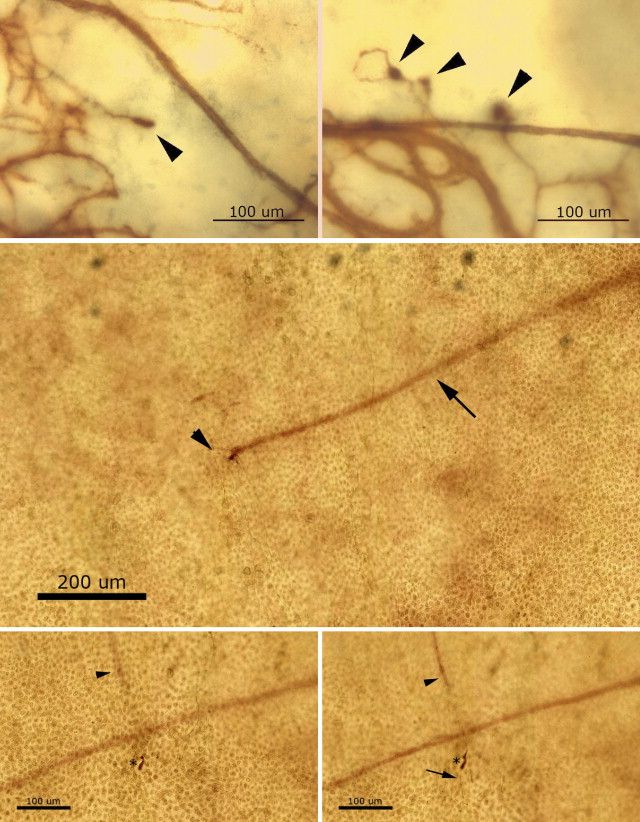
Almost all the stromal nerves did not follow the normal distribution pattern wherein the nerves tend to bifurcate into 2 or more thinner branches and move anteriorly to penetrate the Bowman zone, ending in terminal bulbs that give rise to subbasal nerves. Only 3 nerves in 2 grafts (Patients 4 and 11) were seen to have this normal pattern ( Figure 4 , Middle, and Bottom left and right).
Results
Subbasal Nerves
Subbasal nerves were found in 9 of the 12 patients (75%) at the graft periphery and 3 patients (25%) at the center of the graft. Almost all of these nerves originated from the host subbasal nerves and crossed the graft-host junction radially ( Figure 1 , Top left and right). These nerves appeared thin, tortuous, and reduced in number ( Figure 1 , Middle left). The clockwise whorl configuration of the subbasal nerve plexus was not detected in any cornea.



