 Orbital Vascular and Hemorrhagic Lesions
Orbital Vascular and Hemorrhagic LesionsOrbital Capillary Hemangioma
General Considerations
Capillary hemangioma (benign hemangioendothelioma; strawberry hemangioma) is an important cutaneous vascular tumor of childhood. In the ocular region, it usually begins on the eyelid (see section on eyelid tumors), but it can occasionally occur in the orbit (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20). About 7% of ocular adnexal capillary hemangiomas arise in the orbit posterior to the orbital septum (12). In the authors’ series, orbital capillary hemangioma accounted for 1% of all biopsied orbital lesions in all age groups (2) and for 4% of all orbital biopsies in children (3). In the more recent clinical review of 1,264 cases, orbital capillary hemangioma accounted for 4% of all orbital masses (4). In the authors’ series of 1,264 consecutive space-occupying orbital lesions, the 36 capillary hemangiomas accounted for 17% of the 213 vascular lesions and for 3% of all lesions (4).
Clinical Features
When it occurs in the orbit, capillary hemangioma is usually apparent shortly after birth as a soft mass deep to the eyelid. It is more pronounced when the child strains or cries. Occasionally, it occurs in the deeper portions of the orbit without eyelid signs. Associated hemangioma on the periocular skin facilitates making the orbital diagnosis. The main complications are amblyopia and strabismus. Lesions .1 cm in diameter are more likely to cause these complications, whereas lesions ,1 cm in diameter are considerably less likely to do so (18). The lesion usually shows enlargement for 1 to 2 years and then undergoes gradual regression, similar to eyelid capillary hemangioma. Orbital capillary hemangioma may be associated with large visceral hemangiomas, which can cause platelet entrapment and thrombocytopenia, a condition called the Kasabach-Merritt syndrome (1).
Orbital capillary hemangioma is rare in adults. However, an orbital tumor with similar histopathologic features has been reported to arise in the medial rectus muscle of a 73-year-old woman (14).
Diagnostic Approaches
With computed tomography (CT) and magnetic resonance imaging (MRI), orbital capillary hemangioma varies from case to case. It can be a round or ovoid circumscribed mass or an irregular or diffuse mass. It shows marked homogeneous enhancement with contrast agents. It is important that rhabdomyosarcoma can have similar features and should be included in the differential diagnosis. However, rhabdomyosarcoma rarely is present in infancy but generally occurs in children aged between 5 and 15 years.
Pathology and Pathogenesis
Histopathologically, orbital capillary hemangioma is composed of lobules of proliferating small vascular channels separated by thin fibrous septa. The pathogenesis of capillary hemangioma has been largely unknown. However, it has been recognized that placenta and capillary hemangiomas have unique immunohistochemical similarities. This has led to speculation that infantile hemangiomas could be of placental origin. Two theories have been proposed to explain this hemangioma- placental connection. First, angioblasts may proliferate toward placental tissue in the site where the hemangioma develops. A second intriguing theory is that cells of placental origin could embolize to the target areas (15,16).
Management
Initial management of orbital capillary hemangioma should include refraction and occlusive patching treatment for associated amblyopia. If there is no threat to vision, the lesion can be cautiously observed. Oral or local injection of cortico steroids can hasten regression of the lesion. Ultrasound guidance has been used to accurately place the needle in the tumor (10). However, corticosteroids have a number of potential complications, including retinal artery obstruction, linear perilymphatic subcutaneous fat atrophy, eyelid depigmentation, eyelid necrosis, and adrenal gland suppression (7,18,19). Interferon-a-2b has also been reported to be effective in hastening tumor regression (9). Surgical excision is an appropriate treatment for select well-circumscribed tumors (8,13).
Selected References
1. Shields JA. Vasculogenic tumors and malformations. Capillary hemangioma. In: Shields JA, ed. Diagnosis and Management of Orbital Tumors. Philadelphia: WB Saunders; 1989:124-128.
2. Shields JA, Bakewell B, Augsburger DG, et al. Classification and incidence of space-occupying lesions of the orbit. A survey of 645 biopsies. Arch Ophthalmol 1984;102:1606-1611.
3. Shields JA, Bakewell B, Augsburger DG, et al. Space-occupying orbital masses in children. A review of 250 consecutive biopsies. Ophthalmology 1986;93:379-384.
4. Shields JA, Shields CL, Scartozzi R. Survey of 1264 patients with orbital tumors and simulating lesions: the 2002 Montgomery Lecture, part 1. Ophthalmology 2004;111:997-1008.
5. Haik BG, Jakobiec FA, Ellsworth RM, et al. Capillary hemangioma of the lids and orbit: an analysis of the clinical features and therapeutic results in 101 cases. Ophthalmology 1979;86:760-792.
6. Egbert JE, Paul S, Engel WK, et al. High injection pressure during intralesional injection of corticosteroids into capillary hemangiomas. Arch Ophthalmol 2001;119:677-683.
7. O’Keefe M, Lanigan B, Byrne SA. Capillary haemangioma of the eyelids and orbit: a clinical review of the safety and efficacy of intralesional steroid. Acta Ophthalmol Scand 2003;81:294-298.
8. Aldave AJ, Shields CL, Shields JA. Surgical excision of selected amblyogenic periorbital capillary hemangiomas. Ophthalmic Surg Lasers 1999;30: 754-757.
9. Hastings MM, Milot J, Barsoum-Homsy M, et al. Recombinant interferon alfa-2b in the treatment of vision-threatening capillary hemangiomas in childhood. JAAPOS 1997;1:226-230.
10. Neumann D, Isenberg SJ, Rosenbaum AL, et al. Ultrasonographically guided injection of corticosteroids for the treatment of retroseptal capillary hemangiomas in infants. JAAPOS 1997;1:34-40.
11. Gunalp I, Gunduz K. Vascular tumors of the orbit. Doc Ophthalmol 1995; 89:337-345.
12. Haik BG, Jakobiec FA, Ellsworth RM, et al. Capillary hemangioma of the lids and orbit: an analysis of the clinical features and therapeutic results in 101 cases. Ophthalmology 1979;86:760-792.
13. Deans RM, Harris GJ, Kivlin JD. Surgical dissection of capillary hemangiomas. An alternative to intralesional corticosteroids. Arch Ophthalmol 1992;110:1743-1747.
14. Cockerham KP, Sachs DM, Cockerham GC, et al. Orbital hemangioblastoma arising in a rectus muscle. Ophthal Plast Reconstr Surg 2003;19:248-250.
15. North PE, Waner M, Mizeracki A, et al. A unique microvascular phenotype shared by juvenile hemangiomas and human placenta. Arch Dermatol 2001;137:559-570.
16. North PE, Waner M, Brodsky MC. Are infantile hemangiomas of placental origin? Ophthalmology 2002;109:633-634.
17. DePotter P, Dolinskas C, Shields CL, et al. Vascular tumors. In: DePotter P, Shields JA, Shields CL, eds. MRI of the Eye and Orbit. Philadelphia: JB Lippincott; 1994:159-181.
18. Ceisler E, Blei F. Ophthalmic issues in hemangiomas of infancy. Lymphat Res Biol 2003;:321-330.
19. Goyal R, Watts P, Lane CM, et al. Adrenal suppression and failure to thrive after steroid injections for periocular hemangioma. Ophthalmology 2004;111:389-395.
20. Ceisler E, Blei F. Ophthalmic issues in hemangiomas of infancy. Lymphat Res Biol 2003;1:321-330.
Orbital Capillary Hemangioma
Orbital capillary hemangioma can occur in the deep orbit and produce proptosis or displacement of the globe or it can occur in the anterior portion of the orbit and present as a reddish-blue, fluctuant, subcutaneous eyelid mass. The more common cutaneous eyelid capillary hemangioma is discussed in this text.
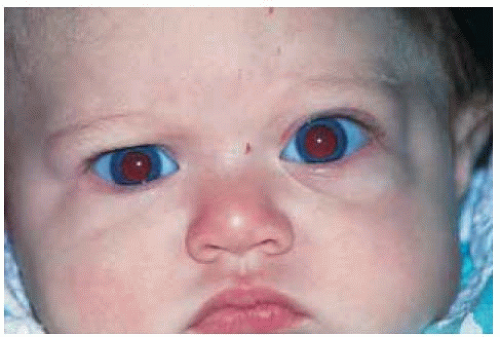 Figure 28.1. Prominence of left lower eyelid secondary to orbital capillary hemangioma in a 4-month-old girl. |
 Figure 28.2. Prominence of left lower eyelid secondary to orbital capillary hemangioma in a 2-year-old girl. |
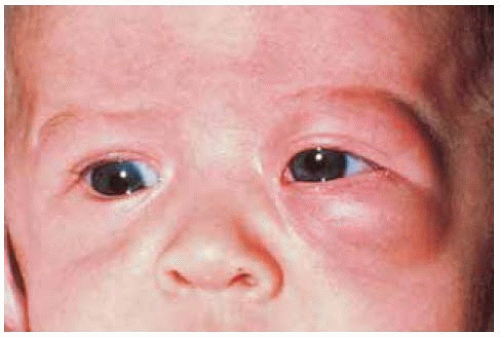 Figure 28.3. Prominence of left lower and upper eyelids secondary to orbital capillary hemangioma in a 1-year-old girl. |
 Figure 28.4. Extension of orbital capillary hemangioma into the medial aspect of the conjunctiva. The child had visceral hemangiomas and may have had a variant of the Kasabach-Merritt syndrome. |
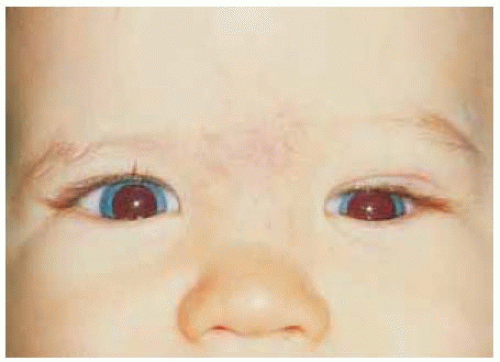 Figure 28.5. Slight downward displacement of the left eye in an 8-month-old boy with superior orbital capillary hemangioma. |
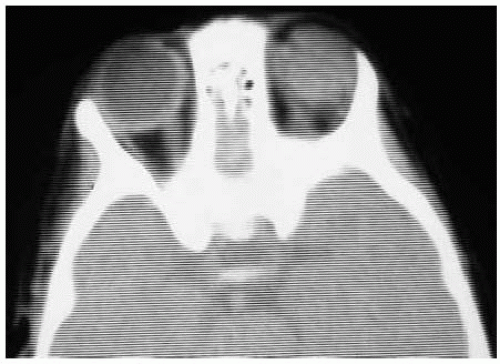 Figure 28.6. Axial computed tomography of child shown in Figure 28.5 demonstrating a diffuse mass superior to the left eye. |
Orbital Capillary Hemangioma: Clinical Variations and Regression
Orbital capillary hemangioma can have a variety of clinical manifestations. A common feature of infantile capillary hemangiomas, however, is their tendency to grow rapidly in infancy and then to stabilize and gradually regress.
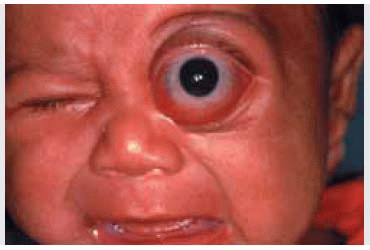
 Figure 28.7. Proptosis of the left eye in a 4-month-old girl. The associated cutaneous hemangioma should suggest an orbital hemangioma as the cause of the proptosis. |
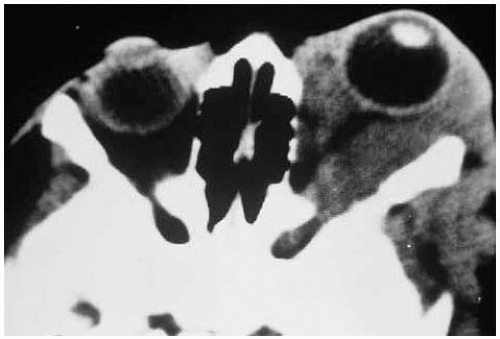 Figure 28.8. Axial computed tomography of patient shown in Figure 28.7. Note the diffuse involvement of the orbital soft tissues. |
 Figure 28.9. Characteristic subcutaneous mass superonasal to the right eye in a 5-month-old girl. |
 Figure 28.10. Appearance of child shown in Figure 28.9 at 23 months. The lesion has regressed without treatment. |
 Figure 28.11. Reddish-blue subcutaneous mass beneath right lower eyelid in a 4-month-old boy. |
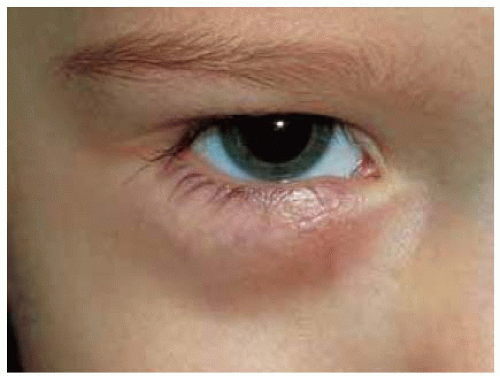 Figure 28.12. Appearance of child shown in Figure 28.11 at 24 months. The lesion has shown regression without treatment. |
Orbital Capillary Hemangioma: Simultaneous Eyelid and Adnexal Involvement
In some instances, a capillary hemangioma of the eyelid can be associated with orbital capillary hemangioma and extraocular cutaneous hemangiomas.
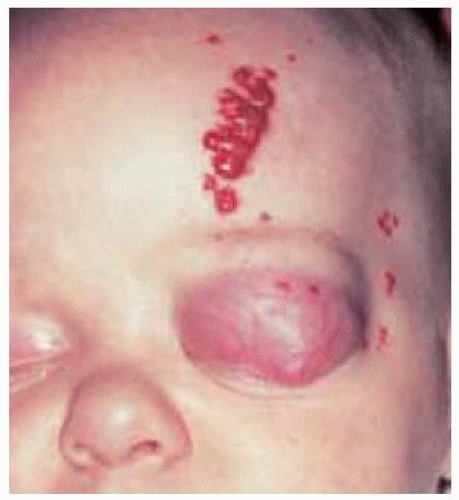 Figure 28.13. Capillary hemangioma of orbit with involvement of eyelid and forehead. |
 Figure 28.14. Closer view of eyelid lesion. Much of the eyelid component of the tumor is subcutaneous. |
 Figure 28.15. Closer view of forehead lesion showing red lobular mass. |
 Figure 28.16. Management of patient with patching of opposite eye and opening the affected eyelid with tape to forehead. |
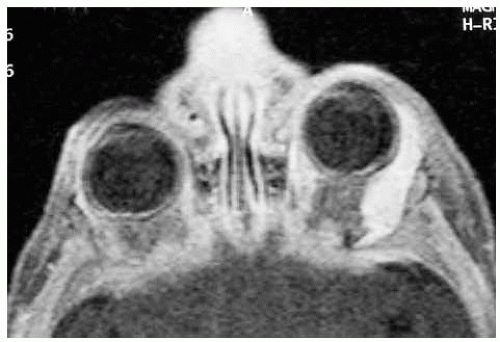 Figure 28.17. Magnetic resonance imaging in T1-weighted image showing enhancement of superotemporal temporal orbital mass. |
 Figure 28.18. Magnetic resonance imaging in T2-weighted image showing extensive hyperintense orbital mass. |
Orbital Capillary Hemangioma: Surgical Resection
In a very young infant, surgical excision may be the best treatment of a large, anterior, well-circumscribed orbital capillary hemangioma producing significant ocular signs and symptoms and that is destined to show further growth and visual loss. A clinicopathologic correlation is shown.
Aldave AJ, Shields CL, Shields JA. Surgical excision of selected amblyogenic periorbital capillary hemangiomas. Ophthalmic Surg Lasers 1999;30:754-757.
 Figure 28.19. Extensive inferior orbital mass producing a prominent blue appearance to the left lower eyelid in an infant girl. The lesion was growing rapidly. |
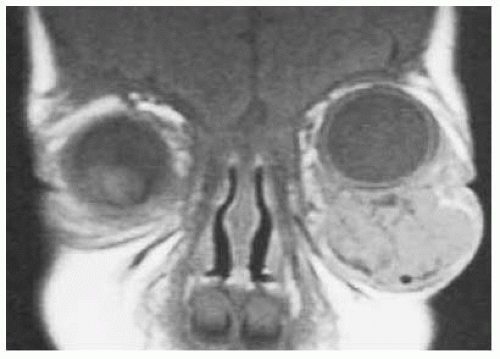 Figure 28.20. Coronal magnetic resonance imaging in T1-weighted image showing large but fairly well-circumscribed inferior orbital mass with upward displacement of the left eye. The mass was removed by way of an eyelid crease incision. |
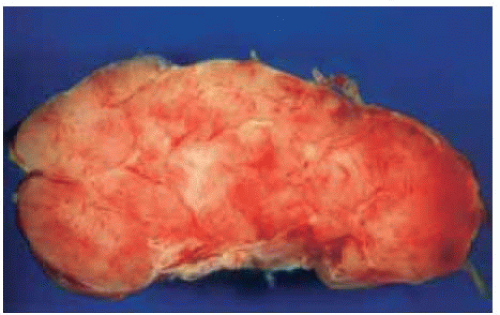 Figure 28.21. Appearance of the lesion after surgical excision and bisection, showing that the lesion was removed intact. |
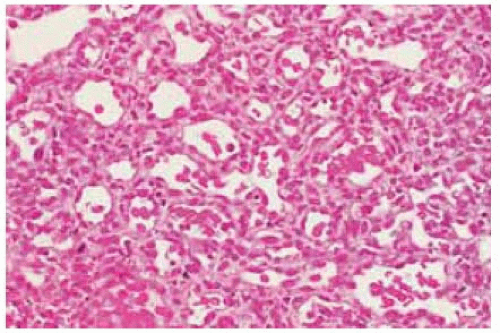 Figure 28.22. Low-magnification photomicrograph showing lobules of proliferating endothelial cells with fine blood vessels. (Hematoxylin-eosin 75.) |
 Figure 28.23. Appearance of same child 7 weeks after surgery showing good cosmetic outcome. |
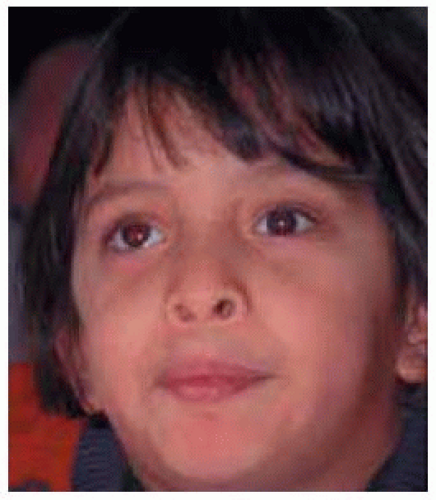 Figure 28.24. Appearance at age 7 years. |
Orbital Cavernous Hemangioma
General Considerations
Cavernous hemangioma is the most common vascular tumor of the orbit (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31). In the authors’ series of 1,264 orbital masses, the 77 cavernous hemangiomas accounted for 36% of vascular tumors and for 6% of all tumors in the series (3). In a series from Turkey, 41% of orbital vascular tumors were cavernous hemangiomas (16). In another report by the authors, it accounted for 8% of orbital tumors in patients $60 years of age (22).
Clinical Features
Orbital cavernous hemangioma is a benign tumor that tends to occur in adulthood as a relatively stationary or slowly progressive lesion that can produce painless proptosis. Because it most often occurs in the muscle cone, it usually produces axial proptosis. It does not generally produce inflammatory signs. Rarely, a cavernous hemangioma can present as an intraosseous lesion in the orbital bones (6,8,23). Orbital cavernous hemangioma is rarely bilateral (9). Although cavernous hemangioma is generally a solitary lesion, it can sometimes be multiple, particularly when seen in the blue rubber bleb nevus syndrome (13,21). In rare instances, multiple confluent cavernous hemangiomas have involved the orbit and brain simultaneously (26).
Diagnostic Approaches
Modern techniques of neuroimaging have been instrumental in making a more accurate diagnosis of orbital cavernous hemangioma (25). Since the advent of good imaging modalities like computed tomography and magnetic resonance imaging, this tumor is often being discovered more often as a coincidental finding when it is small and asymptomatic. As it slowly enlarges, it can produce marked proptosis, compression of the optic nerve, and choroidal folds. Imaging studies demonstrate a well-circumscribed round to ovoid mass, usually in the muscle cone. It shows mild enhancement with contrast agents. The differential diagnosis of a well-circumscribed, round to ovoid, solid orbital mass also includes peripheral nerve sheath tumors (schwannoma and neurofibroma), hemangiopericytoma, fibrous histiocytoma, solitary fibrous tumor, and melanoma. It has been suggested that orbital cavernous hemangioma can be differentiated from schwannoma by contrast-enhancement spread pattern methods on dynamic MRI (27).
Pathology
Histopathologically, orbital cavernous hemangioma is composed of dilated, congested vascular channels separated by connective tissue that contains smooth muscle. The pattern is generally quite typical but on occasion lymphangioma can have similar histopathologic features.
Management
Management of orbital cavernous hemangioma ranges from periodic observation for small, asymptomatic lesions to surgical excision for larger, symptomatic tumors. The surgical approach is determined by the size and location of the tumor. A conjunctival or cutaneous approach may be used for anterior lesions. We have had considerable success removing cavernous hemangiomas that are located in the anterior half of the orbit by a transconjunctival approach. Deep orbital tumors may require a lateral orbitotomy, sometimes with an osteotomy (Kronlein approach). Complete excision is important and meticulous surgery is necessary to avoid incomplete excision and recurrence. Techniques of transcranial approach are used for lesions located at the orbital apex (11).
Selected References
1. Shields JA. Vasculogenic tumors and malformations: cavernous hemangioma. In: Shields JA, ed. Diagnosis and Management of Orbital Tumors. Philadelphia: WB Saunders; 1989:128-132.
2. Shields JA, Bakewell B, Augsburger DG, et al. Classification and incidence of space-occupying lesions of the orbit. A survey of 645 biopsies. Arch Ophthalmol 1984;102:1606-1611.
3. Shields JA, Bakewell B, Augsburger DG, et al Space-occupying orbital masses in children. A review of 250 consecutive biopsies. Ophthalmology 1986;93:379-384.
4. Shields JA, Shields CL, Scartozzi R. Survey of 1264 patients with orbital tumors and simulating lesions: the 2002 Montgomery Lecture, part 1. Ophthalmology 2004;111:997-1008.
5. Weiss SW, Goldblum JR. Benign tumors and tumor-like lesions of blood vessels. In: Weiss SW, Goldblum JR, eds. Enzinger and Weiss’s Soft Tissue Tumors. 4th ed. St. Louis: CV Mosby; 2001:837-890.
6. DePotter P, Dolinskas C, Shields CL, et al. Vascular tumors. In: DePotter P, Shields JA, Shields CL, eds. MRI of the Eye and Orbit. Philadelphia: JB Lippincott; 1994:159-181.
7. Selva D, Strianese D, Bonavolonta G, et al. Orbital venous-lymphatic malformations (lymphangiomas) mimicking cavernous hemangiomas. Am J Ophthalmol 2001;131:364-370.
8. Colombo F, Cursiefen C, Hofmann-Rummelt C, et al. Primary intraosseous cavernous hemangioma of the orbit. Am J Ophthalmol 2001;131:151-152.
9. Shields JA, Hogan RN, Shields CL, et al. Bilateral cavernous haemangiomas of the orbit. Br J Ophthalmol 2000;84:928.
10. Thorn-Kany M, Arrue P, Delisle MB, et al. Cavernous hemangiomas of the orbit: MR imaging. J Neuroradiol 1999;26:79-86.
11. Maus M, Goldman HW. Removal of orbital apex hemangioma using new transorbital craniotomy through suprabrow approach. Ophthal Plast Reconstr Surg 1999;15:166-170.
12. Gdal-On M, Gelfand YA. Surgical outcome of transconjunctival cryosurgical extraction of orbital cavernous hemangioma. Ophthalmic Surg Lasers 1998;29:969-973.
13. McCannel CA, Hoenig J, Umlas J, et al. Orbital lesions in the blue rubber bleb nevus syndrome. Ophthalmology 1996;103:933-936.
14. Mojon D, Odel JG, Rios R, et al. Presumed orbital hemangioma associated with the blue rubber bleb nevus syndrome. Arch Ophthalmol 1996;114:618-619.
15. Acciarri N, Giulioni M, Padovani R, et al. Orbital cavernous angiomas: surgical experience on a series of 13 cases. J Neurosurg Sci 1995;39:203-209.
16. Gunalp I, Gunduz K. Vascular tumors of the orbit. Doc Ophthalmol 1995;89:337-345.
17. Hassler W, Schaller C, Farghaly F, et al. Transconjunctival approach to a large cavernoma of the orbit. Neurosurgery 1994;34:859-861.
18. Bajaj MS, Nainiwal SK, Pushker N, et al. Multifocal cavernous hemangioma: a rare presentation. Orbit 2003;22:155-159.
19. Rootman J. Vascular malformations of the orbit: hemodynamic concepts. Orbit 2003;22:103-120.
20. Kim YH, Baek SH, Choi WC. The transconjunctival approach to a large retrobulbar cavernous hemangioma of the orbit. Korean J Ophthalmol 2002;16:37-42.
21. Chang EL, Rubin PA. Bilateral multifocal hemangiomas of the orbit in the blue rubber bleb nevus syndrome. Ophthalmology 2002;109:537-541.
22. Demirci H, Shields CL, Shields JA, et al. Orbital tumors in the older adult population. Ophthalmology 2002;109:243-248.
23. Hwang K. Intraosseous hemangioma of the orbit. J Craniofac Surg 2000;11:386-387.
24. Shields JA, Shields CL, Eagle RC. Cavernous hemangioma of the orbit. Arch Ophthalmol 1987;105:853.
25. Ansari SA, Mafee MF. Orbital cavernous hemangioma: role of imaging. Neuroimaging Clin N Am 2005;15:137-158.
26. Puca A, Colosimo C, Tirpakova B, et al. Cavernous hemangioma extending to extracranial, intracranial, and orbital regions. Case report. J Neurosurg 2004;101:1057-1060.
27. Tanaka A, Mihara F, Yoshiura T, et al. Differentiation of cavernous hemangioma from schwannoma of the orbit: a dynamic MRI study. AJR Am J Roentgenol 2004;183:1799-1804.
28. Yan J, Wu Z. Cavernous hemangioma of the orbit: analysis of 214 cases. Orbit 2004;23:33-40.
29. Bajaj MS, Nainiwal SK, Pushker N, et al. Multifocal cavernous hemangioma: a rare presentation. Orbit 2003;22:155-159.
30. Harris GJ, Perez N. Surgical sectors of the orbit: using the lower fornix approach for large, medial intraconal tumors. Ophthal Plast Reconstr Surg 2002;18:349-354.
31. Kim YH, Baek SH, Choi WC. The transconjunctival approach to a large retrobulbar cavernous hemangioma of the orbit. Korean J Ophthalmol 2002;16:37-42.
Orbital Cavernous Hemangioma
With the advent of computed tomography and magnetic resonance imaging, some orbital cavernous hemangiomas are discovered at an early stage, when they are asymptomatic. Such lesions can usually be followed without treatment because they often remain asymptomatic for many years. The patient can be examined once or twice a year with pupil examination, visual acuity, color vision, exophthalmometry, ophthalmoscopy, visual fields, and CT or MRI studies. If the patient begins to develop findings that could cause visual loss, the surgical removal of the tumor is generally appropriate. Like other orbital tumors, they can produce fundus changes like choroidal folds, optic disc edema, and compression of the globe.
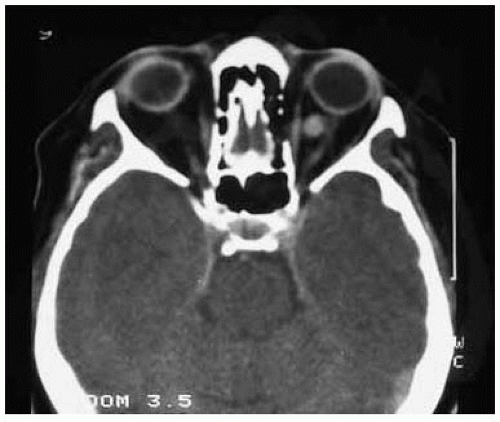 Figure 28.25. Axial computed tomography of small asymptomatic cavernous hemangioma in anterior orbit immediately posterior to the globe and nasal to the optic nerve. Management was periodic observation only. |
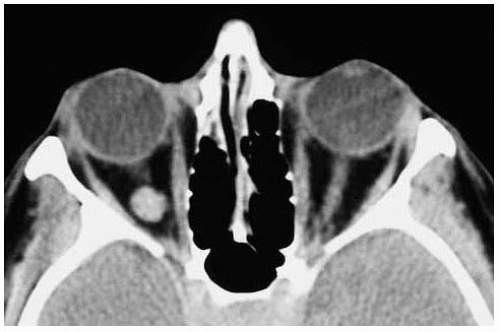 Figure 28.26. Axialcomputed tomography of small asymptomatic cavernous hemangioma closer to the orbital apex. A lesion like this is difficult to remove surgically. Management was periodic observation only. |
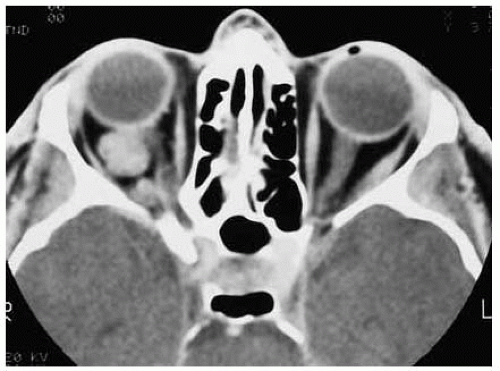 Figure 28.27. Axial computed tomography of slightly larger but asymptomatic cavernous hemangioma in midportion of orbit in muscle cone. Management was periodic observation only. |
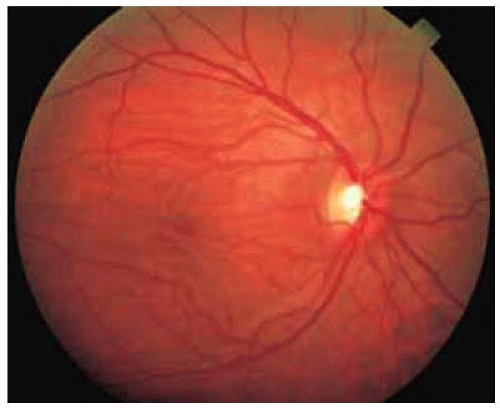 Figure 28.28. Fundus photograph showing characteristic horizontal choroidal folds secondary to another intraconal cavernous hemangioma. |
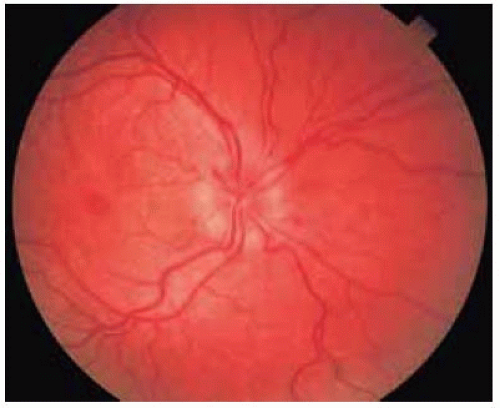 Figure 28.29. Optic disc edema secondary to optic nerve compression by orbital cavernous hemangioma. |
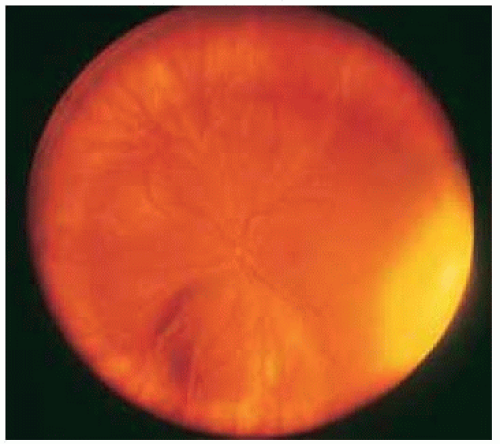 Figure 28.30. Wide-angle fundus photograph showing compression of inferior portion of globe by an orbital cavernous hemangioma. Such an elevation can sometimes be confused with an intraocular neoplasm. |
Orbital Cavernous Hemangioma: Surgical Removal by Conjunctival Approach
In cases of suspected orbital cavernous hemangioma, one must determine the best approach to surgical removal. If a portion of the tumor is located fairly anteriorly, a conjunctiva approach, rather than cutaneous approach, can be employed in selected cases. An example is shown of a relatively large cavernous hemangioma that was removed by a conjunctival approach. In such instances, a cryoprobe can facilitate removal of the tumor.
 Figure 28.31. Axial proptosis of left eye by orbital cavernous hemangioma. |
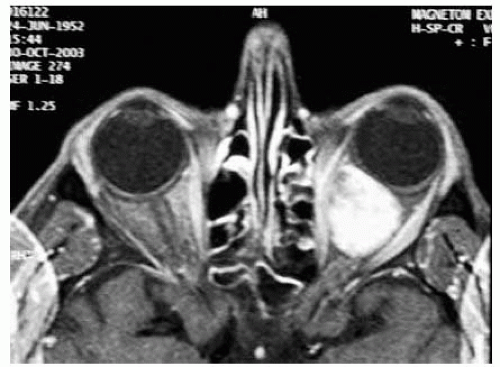 Figure 28.32. Axial magnetic resonance imaging with T1-weighted image and fat suppression, demonstrating large, round, cavernous hemangioma in muscle cone. |
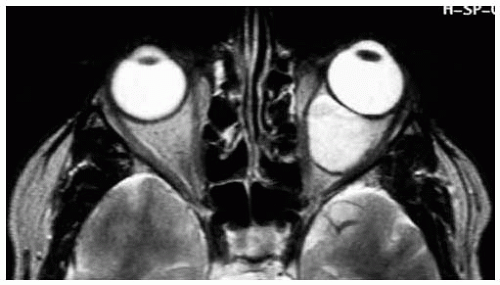 Figure 28.33. Same lesion seen in T1-weighted image. Note that the tumor is causing forward displacement and indentation of the globe. Based on the inferonasal location of the mass, it was elected to remove by a conjunctival approach. |
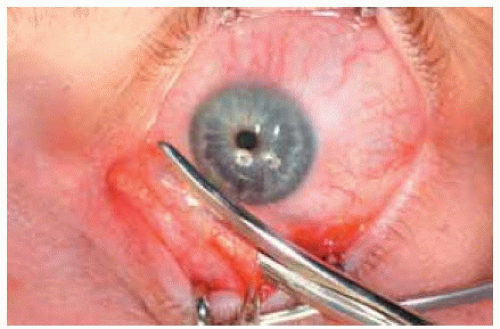 Figure 28.34. Incision with scissors being made in the bulbar conjunctiva inferonasally. |
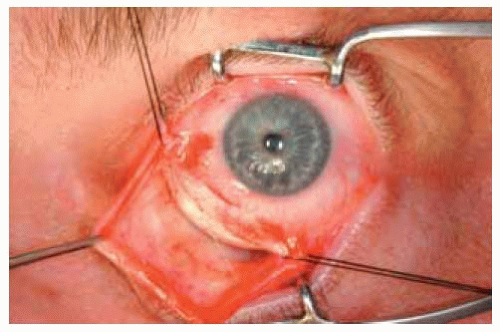 Figure 28.35. The incision has been completed and traction sutures have been placed beneath the insertions of the medial and inferior rectus muscles to assist in rotation of the globe for better exposure. |
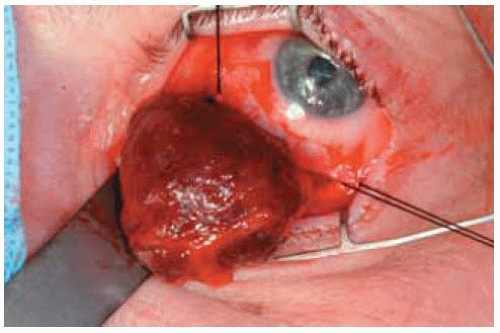 Figure 28.36. Typical orbital cavernous hemangioma being removed. Some sizable cavernous hemangiomas can be removed quickly and successfully by the conjunctival approach. |
Orbital Cavernous Hemangioma: Globe and Optic Nerve Compression
Depicted is a clinicopathologic correlation of a cavernous hemangioma with globe compression and optic discedema in which the tumor was removed through a horizontal forniceal conjunctival incision.
 Figure 28.37. Slight proptosis of left eye in a 40-year-old man. The pupil was dilated pharmacologically at the time of the photograph. |
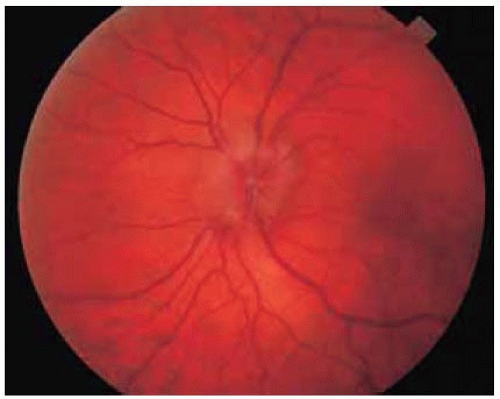 Figure 28.38. Optic disc edema secondary to optic nerve compression by the tumor. |
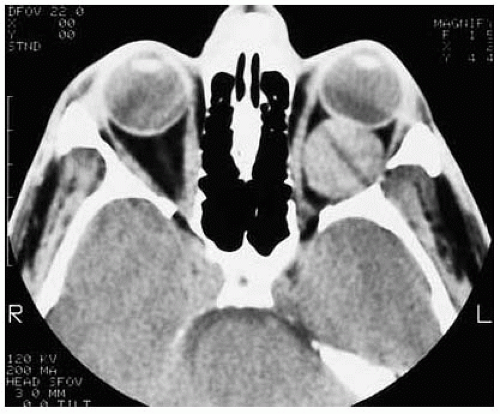 Figure 28.39. Axial computed tomography showing tumor in muscle cone. |
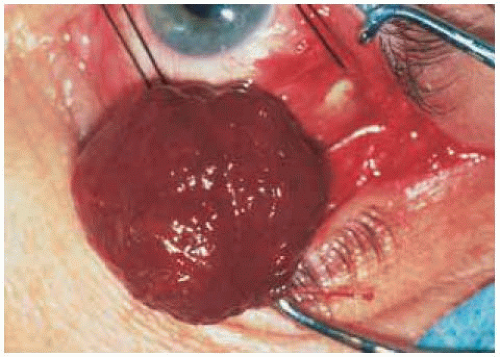 Figure 28.40. Appearance of reddish-blue tumor at the time of removal via an inferotemporal conjunctival incision. |
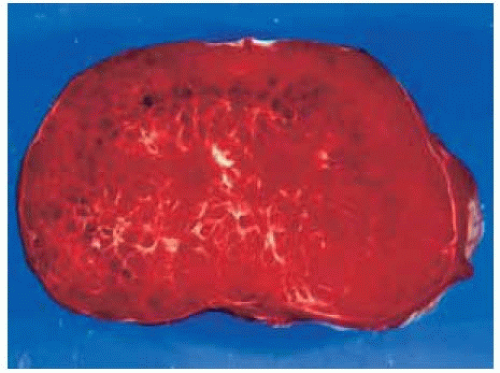 Figure 28.41. Gross appearance after sectioning showing red vascular tumor. |
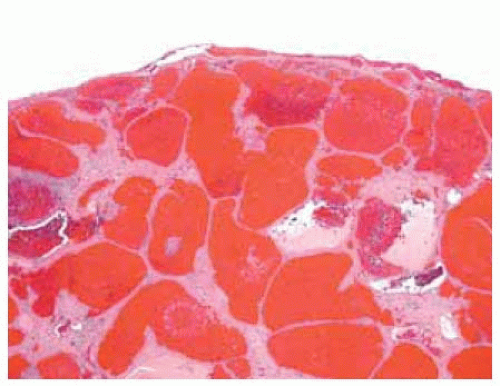 Figure 28.42. Histopathology showing the large congested cavernous vascular channels. (Hematoxylin-eosin 20.) |
Orbital Cavernous Hemangioma: Superotemporal Orbitotomy
Larger tumors in the muscle cone or tumors located laterally in the posterior aspect of the orbit can be removed by a superolateral orbitotomy with a skin incision and extraperiosteal approach. An osteotomy (Kronlein approach) is not usually necessary.
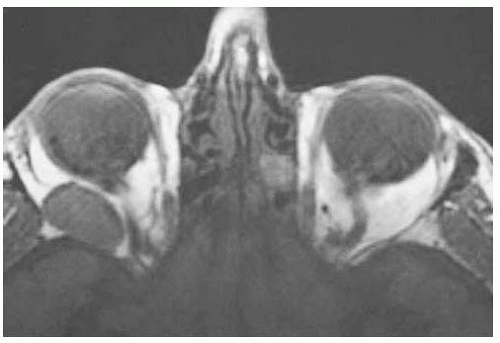 Figure 28.43. Axial magnetic resonance imaging in T1-weighted image showing circumscribed mass in posterolateral aspect of orbit in a 66-year-old man. It was judged to be located a little too posteriorly for removal by conjunctival approach. |
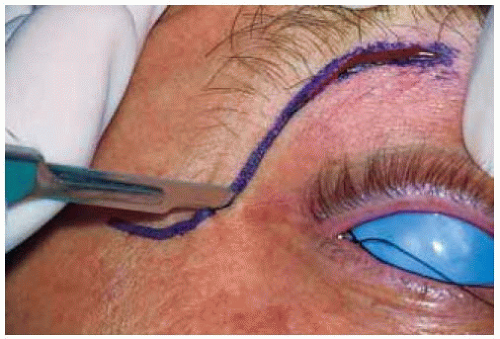 Figure 28.44. Outline of superolateral orbitotomy by a classic cutaneous incision in patient shown in Figure 28.43. |
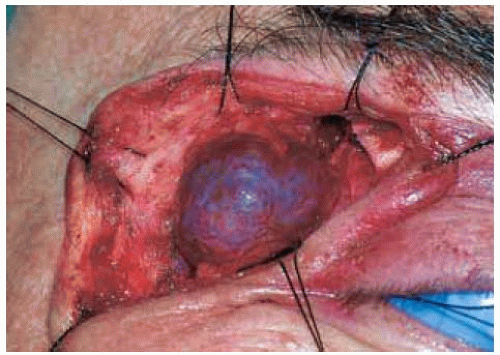 Figure 28.45. Same tumor being removed without an osteotomy. The tumor looks smaller here than suggested on the MRI, because of gradual tumor decompression from manipulation during surgery. |
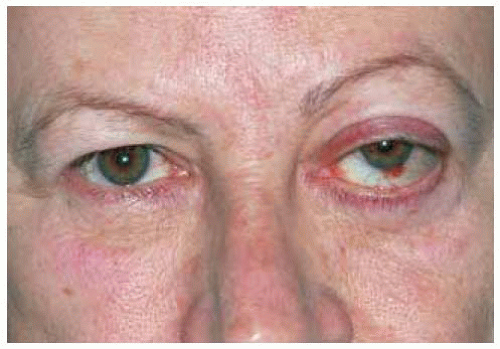 Figure 28.46. Proptosis of left eye in a 61-year-old woman. There is a small conjunctival hemorrhage near the limbus inferiorly, which is rare with cavernous hemangioma and may be unrelated to the tumor. |
 Figure 28.47. Axial computed tomography of woman shown Figure 28.46, demonstrating large mass in muscle cone extending almost to orbital apex. |
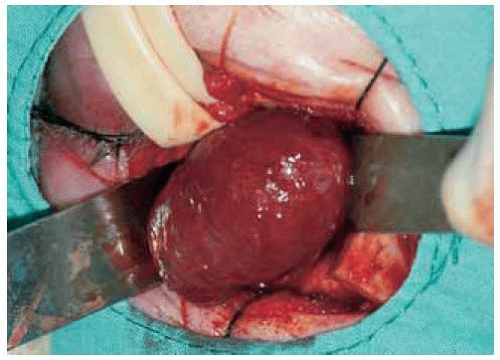 Figure 28.48. Tumor shown in Figure 28.47 being removed by superolateral orbitotomy with osteotomy. |
Orbital Cavernous Hemangioma: Superonasal Orbitotomy
In cases where the tumor is nasal to the optic nerve, a superonasal orbitotomy can be employed. Although a conjunctival incision could have been used in the case shown, the skin-extraperiosteal approach offers better surgical exposure. This patient was seen several years ago; today, we may have used a conjunctival approach in such case.
 Figure 28.49. Proptosis of left eye in a 52-year-old woman. The patient was followed for 5 years previously and proptosis increased and optic disc compression occurred. The normal pupil was dilated pharmacologically at the time of the photograph. |
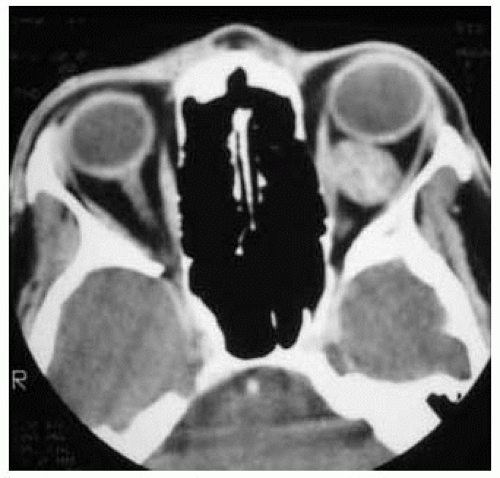 Figure 28.50. Axial computed tomography showing mass in the muscle |
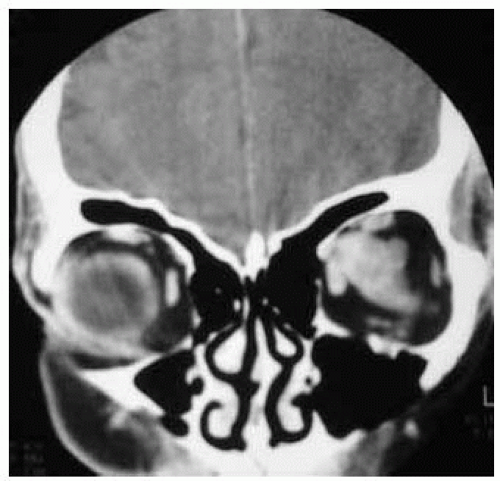 Figure 28.51. Coronal computed tomography showing that the mass is nasal to the optic nerve. |
 Figure 28.52. Outline of superonasal cutaneous eyelid crease approach. |
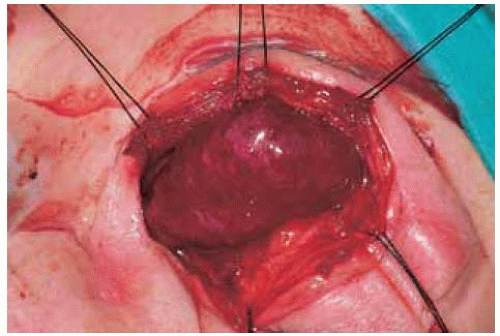 Figure 28.53. Tumor exposed by way of superonasal approach. |
 Figure 28.54. Appearance of wound after closure with interrupted 6-0 silk sutures. Today, the authors more often use absorbable 5-0 mild chromic sutures for closure. |
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


