HISTORY-TAKING
As with other fields of clinical medicine, accuracy in diagnosis and appropriateness of management depend on an orderly protocol that begins with taking an accurate and careful history (
Table 14.1). Review of the personal medical history is an essential part of the assessment of orbital and neuro-ophthalmologic problems. For example, failure to uncover a past history or even a family history of thyroid disease is to ignore a substantial clue to the single most common cause of uni- or bilateral proptosis. Likewise, the presence or absence of vision loss in a patient with orbital congestion and ophthalmoplegia helps to localize an apical from a cavernous sinus lesion. A history of poorly controlled diabetes might suggest the possibility of an opportunistic fungus such as those causing mucormycosis. Clearly, any previous cancer history is suspect, although metastases constitute only 3% to 7% of all biopsied orbital masses
2 (nasopharyngeal and sinus neoplasms accounting for 23% of secondary orbital masses in the British Columbia series
3). A history of cranial or facial trauma likewise must be assessed, but is usually not subtle.
In addition, to family history a complete review of systems is important and frequently of diagnostic value. It is recognized, for instance, that optic glioma is a relatively frequent manifestation of neurofibromatosis (see Volume 2, Chapter 5). Therefore, in a child with unexplained chronic proptosis, the occurrence of skin lesions (birthmarks, skin lumps, or tumors), seizures, or central nervous system (CNS) masses in blood relatives is critical information. Ideally, such family members should be examined or further details obtained. Dysthyroidism also has a distinct familial predilection.
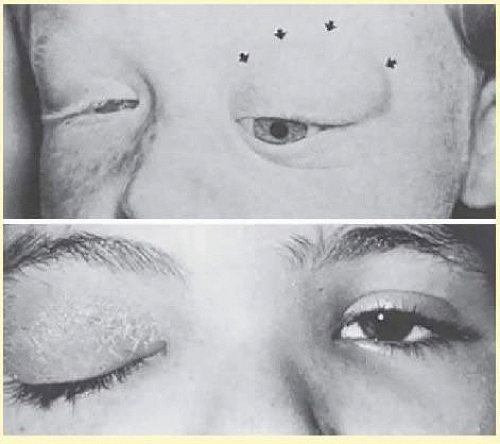
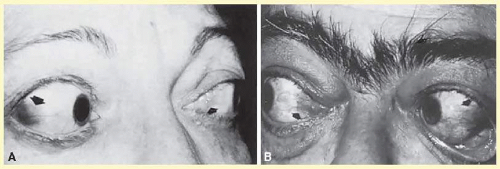
A carefully noted history of rapidly progressive proptosis in a child (
Fig. 14.3) should be considered an orbital emergency, with the clinician’s responsibility being to rule out a life-threatening tumor such as rhabdomyosarcoma or metastatic neuroblastoma. A similar picture may evolve with acute orbital congestion associated especially with ethmoidal or maxillary sinusitis, in children with or without fever.
4,5 In contrast, in an adult, with the exception of metastatic tumors, most orbital neoplasms produce insidiously progressive exophthalmos. Inflammatory orbital “pseudotumor”
6 is the only common cause of relatively abrupt, usually painful, proptosis with diplopia in the otherwise well adult. Myositis occurs in children or adults.
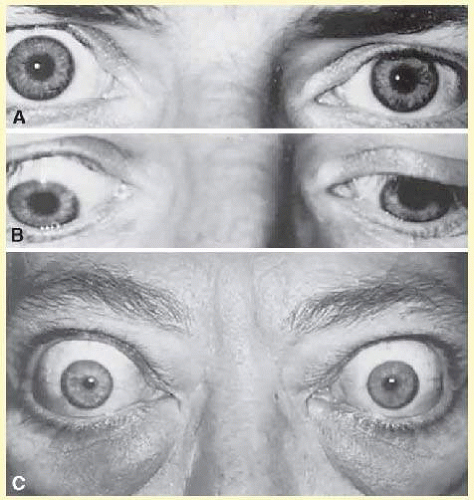
7 The acute phase of Graves’ disease may mimic other orbital congestive syndromes (see below), but usually this most common orbitopathy is subacute or chronic and characterized by achiness and pressure rather than significant pain (
Fig. 14.4). In contrast, intermittent painful proptosis, at times accompanied by spontaneous subconjunctival hemorrhage or lid ecchymoses, is practically pathognomonic of lymphangiomas
8 or, with a history of postural variability indicating a possible venous varix. Presentation can occur over a wide age spectrum, with severe coughing or prolonged retching, or during protracted obstetrical labor, pressure in intraorbital veins may be momentarily raised to the point of rupture with formation of a usually painful retrobulbar hematoma.
9,10 These Valsalva orbital hemorrhages usually resolve spontaneously.
In situations where the duration of proptosis is not clear, review of antecedent photographs (driver’s license, family snapshots, etc.) may be extremely helpful. The clinician should be aware that proptosis may be suddenly discovered rather than actually occurring rapidly, so that the evidence provided by review of previous photographs is helpful in dating true onset. Such photographs may be scrutinized with the illumination and magnification provided by the 20 diopter (D) lens.
Insidiously progressive orbital masses that produce axial (straightforward) displacement of the globe tend not to produce diplopia until they have progressed significantly. Diseases that have a propensity for infiltration of extraocular muscles such as myositis,
7,11 and the restrictive myopathy of Graves’ disease regularly results in diplopia early in their course. As a rule of thumb, pathology such as masses located superiorly in the orbit commonly produce deficits in upward gaze, nasal masses produce adduction deficits, and temporal masses produce abduction deficits. Orbital fractures can result in a variety of patterns of diplopia. Under ideal conditions, these physical observations should be confirmed by enhanced computed tomography (CT) or magnetic resonance imaging (MRI); standardized ultrasonography may be a useful and complementary diagnostic tool when available if an inflammatory process is considered.
Problems with vision can be due to direct compression of the orbital portion of the optic nerve or its circulation by both intra- and extraconal as well as extraorbital pathology but, as with neural structures elsewhere, if the progression is insidious, remarkable chronicity and growth can be seen with preserved and normal nerve function. Retrobulbar masses that indent the posterior pole of the globe may induce relative hyperopia, requiring additional plus lenses to improve acuity. Transient blurring of vision in extremes of gaze, especially abduction or noted during reading,
12 can be produced by any orbital mass, including dysthyroidism. This phenomenon may be related to compression of the optic nerve as it is dynamically stretched over a mass, compressed by contracting muscles, as the posterior wall of the globe becomes deformed, or as vascular flow is compromised (or combinations of these mechanical effects) and can even result in gaze evoked amaurosis.
Proptosis with true orbital pain (as opposed to ocular irritation or foreign body sensation) is relatively rare, with the following exceptions: acute orbital inflammation, metastases, elevated venous pressure due to arteriovenous fistulas or malformations; acute thrombosis of venous varices; and acute thrombosis of enlarged orbital veins associated with arteriovenous fistulas or vascular malformations. Orbital and eye pain may also be a symptom associated with the ophthalmoplegia of an orbital apex and/or cavernous sinus syndrome (see Chapter 12), or can be referred pain from meningeal based pathology. Atta et al.
13 have elaborated a syndrome of venous stasis orbitopathy, composed of proptosis, ophthalmoplegia, and injected conjunctival vessels, of vascular (arteriovenous fistulas) and nonvascular etiologies. These authors note the usefulness of standardized echography, especially with measurement of extraocular muscle diameters, to distinguish fistulas from mass lesions.
ORBITAL EXAMINATION
The ophthalmologist is secure in his ability to directly visualize the anterior and posterior segments of the globe, but the orbit is seemingly less amenable to direct observation. Nonetheless, an office evaluation of the orbit is not as limited as one might think with the appreciation of the standard eye examination as a sensitive and quantitative orbital and neurologic assessment. In addition to standard evaluation of visual function, pupils and ocular motility, the comprehensive eye exam yields observations regarding disruption of normal orbital anatomy and function as outlined in
Table 14.2. Even in an era of excellent imaging modalities, the eye exam remains indispensable in evaluating any disease involving or approaching the orbit because it quantitates function.
Preliminary observations of the face, eyes, and eyelids should be made during history-taking, before the patient’s attention is called to the actual examination and before sympathomimetic agents are instilled for pupil dilation (
Fig. 14.4; see also Volume 2, Chapter 3,
Fig. 3.11); some patients will stare only during intense concentration or conscious effort to cooperate. Facial asymmetry should be identified even when dismissed as congenital or physiologic. Temporalis bulging can be the only sign of a sphenoid wing meningioma, and assessment of facial bone structure may lead to a diagnosis of dysostotic conditions or simple facial hypoplasia associated with congenital superior oblique palsies.
Anomalies of lid position and movement need not be bilateral. Ptosis is quite rare in Graves’ disease, but is fairly common with inflammatory pseudotumor. Lateral ptosis may result from orbital inflammation of the lacrimal gland (dacryoadenitis) or from a plexiform neurofibroma of the lid. Ptosis, in the absence of pain or other congestive orbital signs, should always bring to mind the possibility of myasthenia. Unilateral ptosis may account for contralateral lid retraction; thus, a patient with right partial ptosis may show relative retraction of the left upper lid, due to increased effort in an attempt to overcome the ptosis (Hering’s law of equivalent innervation is applicable to the two levator palpebrae).
14 If the eye with ptosis is occluded, or the lid mechanically raised, the opposite retracted lid will assume a normal position in such cases as opposed to pathologic cases of lid retraction. The differential diagnosis of lid retraction is:
Graves’ ophthalmopathy
Aberrant third nerve regeneration
Unilateral ptosis, with contralateral overaction of levator palpebrae (e.g., myasthenia)
Collier’s sign of dorsal midbrain (Parinaud) syndrome— bilateral
Hyperkalemic periodic paralysis
Congenital ptosis with retraction of the lid noted on downgaze
Mechanical or cicatricial changes
Lid swelling regularly results from the congestive edema of Graves’ disease, but also typically occurs in preseptal or orbital cellulitis, inflammatory pseudotumor, arteriovenous fistulas, and even with acute viral conjunctivitis. Most lid edema is accentuated by sleep, during which time the head is maintained in a relatively dependent position. Palpation of a discrete mass in the lids is exceedingly helpful, since potential biopsy is facilitated. The hue of the edema can be diagnostic ranging from the intense erythema of an infectious process to the boggy violacious faint erythema of an inflammatory process to the more purple ecchymotic appearance of an orbital hemorrhage, lymphangioma, or neuroblastoma.
Veins may be visible within the thin lid tissues, either passively dilated by diffusely increased orbital pressure or engorged by arterialization of orbital and adnexal vessels fed by arteriovenous communications. In the latter case, audible bruits and palpable thrills are evidence of turbulent, increased blood flow.
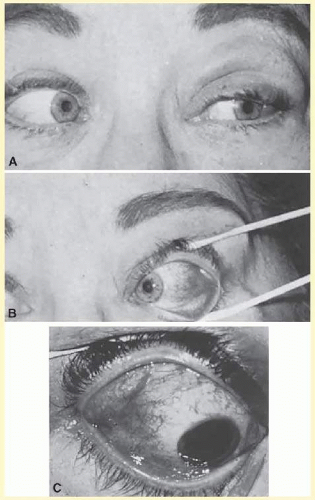
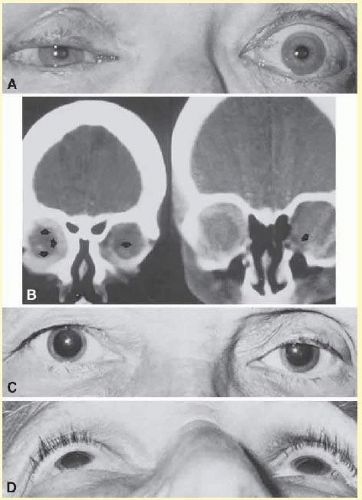
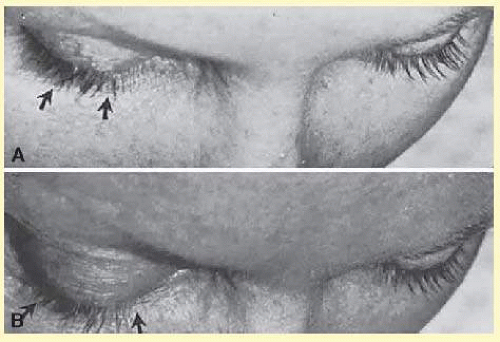
Abnormalities of the conjunctiva may serve as clues to orbital diagnosis. Generalized edema (chemosis) is too nonspecific a finding to be very helpful, as any retrobulbar mass may produce chronic or intermittent chemosis, presumably by interfering with venous drainage in the orbit. In Graves’ ophthalmopathy, the vessels overlying the insertions of especially the medial and lateral recti muscles are commonly enlarged, and indeed the muscle insertions themselves may be visibly hypertrophied (
Fig. 14.5). These conjunctival signs are exceedingly useful in identifying Graves’ orbitopathy and should be sought in cases of unexplained proptosis and/or diplopia. Engorgement of ocular surface vessels takes on a more or less specific pattern or tortuosity and a corkscrew configuration in the presence of arteriovenous fistula (see Volume 2, Chapter 17, Fig. 17.14).
Diffuse or focal hyperemia of deeper scleral and episcleral vessels (especially in the superior lateral quadrant of the globe) is seen in anterior scleritis (episcleritis), or as an anterior component of posterior scleritis that accompanies the painful ophthalmoplegia syndrome of idiopathic orbital inflammation (
Fig. 14.6).
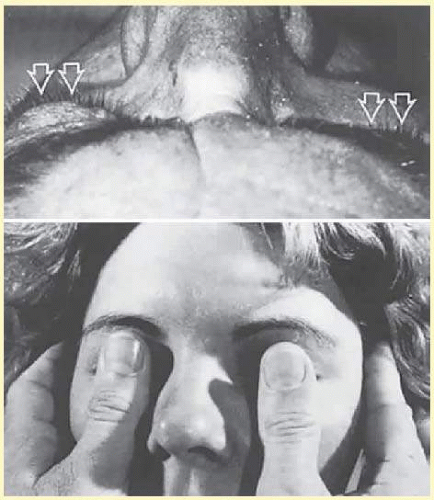
Proptosis should be palpated and looked for both straight on and looking up at the patient from below (
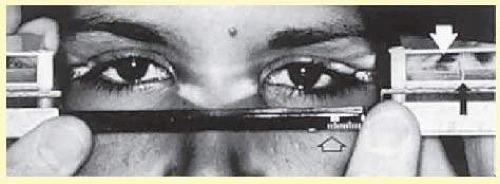
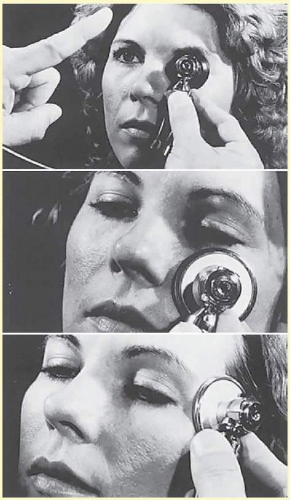
Fig. 14.7). The position of the globes relative to the orbital rims is subject to considerable individual and racial variations. Not the least problem is accuracy and reproducibility of measurements as obtained by a number of exophthalmometric techniques, of which the Hertel exophthalmometer is the most common, and probably the most accurate (
Fig. 14.8). In a study of 681 normal adults ranging in age from 18 to 91 years, mean normal protrusion values were 15.4 mm in white women, 16.5 mm in white men, 17.8 mm in black women, and 18.5 mm in black men; upper limits of normal were 20.1, 21.7, 23.0, and 24.7 mm, respectively.
15 No normal individual showed more than 2 mm of asymmetry.
Thus, there is presently no precise reproducible technique for quantitating proptosis, as minor deviations in positioning of exophthalmometers at the lateral orbital rim result in variations in readings.
16 Even imaging studies have failed to provide a practical solution for this problem.
Some situations give the appearance of proptosis when the globes are in fact less asymmetric, such as unilateral lid retraction, wherein the involved eye appears larger; unilateral mild ptosis, wherein the contralateral eye appears larger due to an elevated lid height and asymmetry of facial bones including orbital rims; and unilateral enophthalmos,
17 wherein the normal contralateral eye appears prominent in comparison (
Fig. 14.9). The differential diagnosis of enophthalmos is included in
Table 14.3.
In a small number of patients, differences in the axial lengths of the globes may account for relative unilateral proptosis. This situation is resolved by finding differences in the amount of myopia.
There is little evidence to support the claim that a complete third nerve palsy results in sufficient relaxation of the muscle cone to produce detectable proptosis.
Pulsation of the globe is encountered most commonly with acquired carotid-cavernous fistulas, and rarely in other conditions.
18 Causes of pulsation are listed in
Table 14.4.
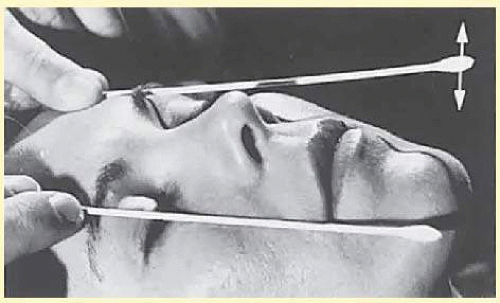
Biomicroscopical examination usually reveals even minimal pulsation, best seen during measurement of intraocular tension by Goldmann applanation tonometry. Cotton-swab sticks may be placed tangentially across the corneal apices, such that transmitted pulsations are amplified by the length of the swab (
Fig. 14.10).
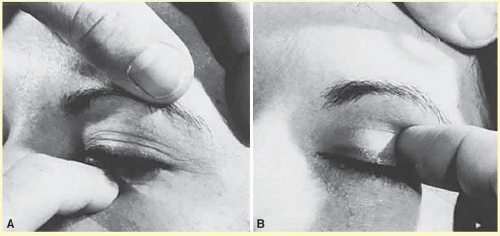
Exploration of the orbital rim by fingertip palpation (
Fig. 14.11) may reveal masses lying in the tissues of the lids and also in the anterior portions of the orbit. Palpation of the orbital and facial bones is mandatory in assessing a patient with facial trauma looking for bony stepoffs or instability from a fracture.
Auscultation of the globe and face is an occasionally useful maneuver to confirm the presence of vascular bruits, as encountered in acquired arteriovenous fistulas or congenital vascular malformations. Bruits may be more intense over zygoma or mastoid bones, where the diaphragm of the stethoscope is more effective than the bell, with which the globe itself is better auscultated (
Fig. 14.12). Symmetrical cranial or ocular bruits are commonly present in normal children and therefore must be evaluated with caution.
Forced expiration against resistance (Valsalva maneuver) raises venous pressure in the neck, face, and head, such that orbital masses with significant draining veins will increase in volume, evidenced by transient increase in proptosis (
Fig. 14.13). This phenomenon is typically demonstrable in the presence of congenital venous varices or arteriovenous malformations, but may also be seen with acquired carotid-cavernous fistula or with primary or secondary bony defects that permit transmission of intracranial pressure to orbital contents. Crying infants with such lesions may show this sign spontaneously or with head-hanging.
Where accompanying physical signs are absent or minimal, the single most useful technique in distinguishing nonrestrictive ophthalmoplegia (e.g., cranial nerve palsies, myasthenia, chronic progressive external ophthalmoplegia) from a restrictive myopathy (e.g., Graves’ ophthalmopathy) is the forced (passive) duction test. In 1967, Stephens and Reinecke
19 reported a method for quantitation of the forced duction test, but no standardized accessible and practical instrument is currently available. There are various techniques to test for mechanical resistance to rotation of the globe, but typically this can be assessed in an examination chair with topical anesthetic applied with a cotton swab to the muscle insertion after which the muscle can be grabbed with a forceps or pushed with a cotton swab. The forced duction test will be positive, that is, there will be resistance to mechanical rotation of the globe, in the following situations: Graves’ restrictive myopathy, inflammatory pseudotumor (myositis), infiltrating carcinoma, and incarceration of extraocular muscles and their surrounding soft tissue attachments that herniate into orbital wall fractures. Because of secondary fibrotic contractures of extraocular muscles, on rare occasions the forced duction test will be positive in the chronic fixed form of ocular myasthenia, in advanced chronic external ophthalmoplegia, with extremely long-standing sixth or third nerve palsies, and the syndrome of Congenital Fibrosis of the Extraocular Muscles. A restrictive myopathy also may occur in long-standing postcataract diplopia.
In situations where the globe is mechanically restricted (again, Graves’ disease is typical) intraocular tension may be elevated, or pressure may inordinately rise on attempted upward gaze.
20,21 However, it must be recognized that intraocular pressure increases linearly with vertical excursions of the globe, changes of as much as 7 mm Hg being recorded in normal subjects.
22 Indeed, this phenomenon in normal subjects brings into question the validity of this procedure as an adjunct in the diagnosis of Graves’ orbitopathy.
23 Carotid cavernous or dural arterial fistulas also typically elevate intraocular tension by raising episcleral venous drainage pressure.
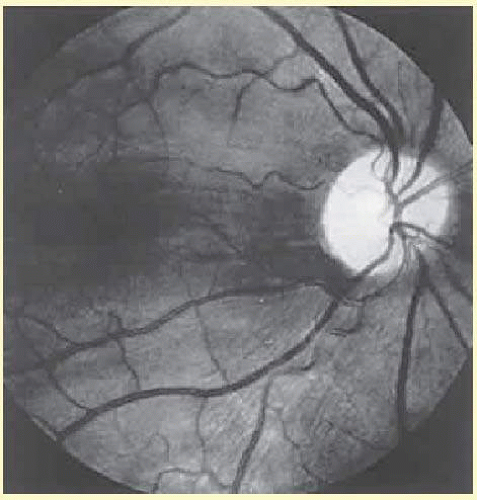
The ocular fundus may be altered by any retrobulbar mass in the following ways: indentations of the posterior wall of the globe produces chorioretinal striae (
Fig. 14.14), while compression at the equator of the globe and beyond results in a more diffuse flattening, best appreciated by indirect ophthalmoscopy, and accentuated by rotation of the eye toward the quadrant(s) of the orbit occupied by the tumor; dilation and tortuosity of retinal veins (venous hemorrhages or occlusions suggest relatively high pressures, as encountered with arteriovenous fistulas); retinal arterial occlusions, especially in orbital phycomycoses such as mucormycosis; edema or frank elevation of the optic nerve head; optic atrophy in chronic compression; optociliary shunt vessels of the disk, especially with perioptic meningioma; and retinal detachment or choroidal suffusion with inflammatory lesions or scleritis. De La Paz and Boniuk
24 have extensively reviewed the fundus manifestations of orbital disease.
Optic disc swelling (
Table 14.5) does not necessarily suggest actual infiltration of the nerve or its meninges, this fundus finding being rather nonspecific and observed potentially with any increase in retrobulbar mass. Indeed, in orbital context, disc edema is seen most commonly with Graves’ orbitopathy. On rare occasions, optic gliomas produce a picture of disc swelling with or without venous occlusion, and perioptic meningiomas may be characterized by a clinical triad of slowly progressive visual loss, pallor admixed with disk swelling, and papillary retinociliary venous shunts (see Chapter 5, Part II).