 Orbital Cystic Lesions
Orbital Cystic LesionsOrbital Dermoid Cyst
General Considerations
Cystic lesions in the orbit are fairly common (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24,25). In the authors’ series of 1,264 orbital masses seen on the oncology service, the 70 orbital cysts seen accounted for 6% of all orbital lesions. Dermoid cyst was the most common, accounting for 26 cases, or 37% of all cystic lesions (4). Overall, about 61% of head and neck dermoid cysts occur in the periorbital region (24). It is a congenital lesion that forms from epithelial cells that are entrapped during embryogenesis beneath the surface epithelium, often near bony sutures. Orbital dermoid cysts have been classified into juxtasutural, sutural, and soft tissue variants, with subcategories of each (5). In a clinicopathologic series of 197 cases from the Oncology Service and Pathology Department of Wills Eye Hospital, it was found that about 70% were located superotemporally at the zygomaticofrontal suture, 20% superonasally at the maxillofrontal suture, and 5% in the nasal soft tissue; other locations were less common (5).
Clinical Features
Orbital dermoid cyst classically occurs as a firm, fixed subcutaneous lesion near the orbital rim superotemporally in a young child. Less often, it develops at the orbital rim superonasally or in the deeper orbital soft tissues. Such a soft tissue nasal cyst is generally derived from conjunctival epithelium and is sometimes call a “conjunctivoid” (8). In most cases, there is a visible and palpable mass beneath the skin. The less common deep orbital cyst causes proptosis and/or displacement of the globe and is sometimes referred to as a “giant dermoid cyst” (12,19). The anterior dermoid can rupture spontaneously or after trauma and produce a subcutaneous inflammatory reaction that resembles cellulitis or dacryoadenitis. A draining cutaneous fistula can develop in such cases (13,25).
Diagnostic Approaches
The classic dermoid cyst can usually be diagnosed based on the clinical appearance of a subcutaneous mass superotemporally at the orbital rim. However, the findings are not pathognomonic and other less common benign and malignant lesions can have a similar appearance. Imaging studies show a cystic lesion with enhancement of the wall but no significant enhancement of the lumen. Adjacent bone changes, usually a smooth fossa, are demonstrated in about 85% of cases (17). Fluid levels and calcification are frequently seen (17,23). In some instances, a dermoid cyst can have extraorbital and intraorbital components that are connected through a defect in bone (dumbbell dermoid) (7).
Pathology
Histopathologically, orbital dermoid cyst is lined by surface epithelium (epidermis or conjunctiva). Cysts lined by conjunctival epithelium are more often found in the orbital soft tissue nasally (8,9). The cyst wall can contain dermal appendages, sebaceous glands, and sweat glands, features that are diagnostic of a dermoid cyst. The cyst lumen contains desquamated epithelial cells, sebaceous material, and hair (5).
Management
Management of orbital dermoid cyst ranges from observation to surgical excision, with most being removed surgically because the patient presents with a visible lesion or ocular symptoms owing to rupture of the cyst and secondary orbital inflammation. An anteriorly located orbital dermoid cyst can be excised by way of a cutaneous or conjunctival approach. An eyelid crease incision may provide a better cosmetic result (21). A deeper cyst may require a lateral orbitotomy. If such a deep cyst cannot be removed intact, it can be aspirated and more easily removed in a collapsed state. Care should be taken to avoid surgical rupture of the cyst if possible. If rupture occurs, vigorous irrigation and instillation of antibiotics or corticosteroids is advisable to prevent postoperative inflammation. The prognosis for vision and life are excellent.
Selected References
1. Shields JA. Cystic lesions of the orbit. Dermoid cyst. In: Shields JA, ed. Diagnosis and Management of Orbital Tumors. Philadelphia: WB Saunders; 1989:94-97.
2. Shields JA, Bakewell B, Augsburger DG, et al. Classification and incidence of space-occupying lesions of the orbit. A survey of 645 biopsies. Arch Ophthalmol 1984;102:1606-1611.
3. Shields JA, Bakewell B, Augsburger DG, et al. Space-occupying orbital masses in children. A review of 250 consecutive biopsies. Ophthalmology 1986;93:379-384.
4. Shields JA, Shields CL, Scartozzi R. Survey of 1264 patients with orbital tumors and simulating lesions: the 2002 Montgomery Lecture, part 1. Ophthalmology 2004;111:997-1008.
5. Shields JA, Kaden IH, Eagle RC Jr, et al. Orbital dermoid cysts. Clinicopathologic correlations, classification, and management. The 1997 Josephine E. Schueler Lecture. Ophthal Plast Reconstr Surg 1997;13: 265-276.
6. Shields JA, Shields CL. Orbital cysts of childhood—classification, clinical features, and management. The 2003 Angeline Parks Lecture. Surv Ophthalmol 2004;49:281-299.
7. Emerick GT, Shields CL, Shields JA, et al. Chewing-induced visual impairment from a dumbbell dermoid cyst. Ophthal Plast Reconstr Surg 1997;13:57-61.
8. Jakobiec FA, Bonanno PA, Sigelman J. Conjunctival adnexal cysts and dermoids. Arch Ophthalmol 1978;96:1404-1409.
9. Shields JA, Augsburger JJ, Donoso LA. Orbital dermoid cyst of conjunctival origin. Am J Ophthalmol 1986;101:726-729.
10. Bickler-Bluth ME, Custer PL, Smith ME. Giant dermoid cyst of the orbit. Arch Ophthalmol 1987;105:1434-1435.
11. Shields JA, Augsburger JJ, Donoso LA. Orbital dermoid cyst of conjunctival origin. Am J Ophthalmol 1986;101:726-769.
12. Grove AS Jr. Giant dermoid cysts of the orbit. Ophthalmology 1979;86: 1513-1520.
13. Pollard ZF, Calhoun J. Deep orbital dermoid with draining sinus. Am J Ophthalmol 1975;79:310-313.
14. Sathananthan N, Moseley IF, Rose GE, et al. The frequency and clinical significance of bone involvement in outer canthus dermoid cysts. Br J Ophthalmol 1993;77:789-794.
15. Sherman RP, Rootman J, Lapointe JJ. Orbital dermoids: Clinical presentation and management. Br J Ophthalmol 1984;68:642-652.
16. Mee JJ, McNab AA, McKelvie P. Respiratory epithelial orbital cysts. Clin Exp Ophthalmol 2002;30:356-360.
17. Chawda SJ, Moseley IF. Computed tomography of orbital dermoids: a 20-year review. Clin Radiol 1999;54:821-825.
18. Niederhagen B, Reich RH, Zentner J. Temporal dermoid with intracranial extension: report of a case. J Oral Maxillofac Surg 1998;56:1352-1354.
19. Leonardo D, Shields CL, Shields JA, et al. Recurrent giant orbital dermoid of infancy. J Pediatr Ophthalmol Strabismus 1994;31:50-52.
20. Sathananthan N, Moseley IF, Rose GE, et al. The frequency and clinical significance of bone involvement in outer canthus dermoid cysts. Br J Ophthalmol 1993;77:789-794.
21. Kronish JW, Dortzbach RK. Upper eyelid crease surgical approach to dermoid and epidermoid cysts in children. Arch Ophthalmol 1988;106: 1625-1627.
22. Samuelson TW, Margo CE, Levy MH, et al. Zygomaticofrontal suture defect associated with orbital dermoid cyst. Surv Ophthalmol 1988;33:127-130.
23. Karatza E, Shields CL, Shields JA, et al. Calcified orbital cyst in an adult simulating a malignant lacrimal gland tumor. Ophthal Plast Reconstr Surg 2004;20:397-399.
24. Pryor SG, Lewis JE, Weaver AL, et al. Pediatric dermoid cysts of the head and neck. Otolaryngol Head Neck Surg 2005;132:938-942.
25. Wells TS, Harris GJ. Orbital dermoid cyst and sinus tract presenting with acute infection. Ophthal Plast Reconstr Surg 2004;20:465-467.
Orbital Dermoid Cyst: Typical Case of Epidermal Origin
Most dermoid cysts in the orbital region are located superotemporally near the zygomaticofrontal suture. A typical case with imaging, surgical approach, and pathology is shown.
Shields JA, Kaden IH, Eagle RC Jr, et al. Orbital dermoid cysts. Clinicopathologic correlations, classification, and management. The 1997 Josephine E. Schueler Lecture. Ophthal Plast Reconstr Surg 1997;13:265-276.
 Figure 27.1 Characteristic left superotemporal subcutaneous mass in a 2-month-old boy. |
 Figure 27.2. Closer view of the lesion. |
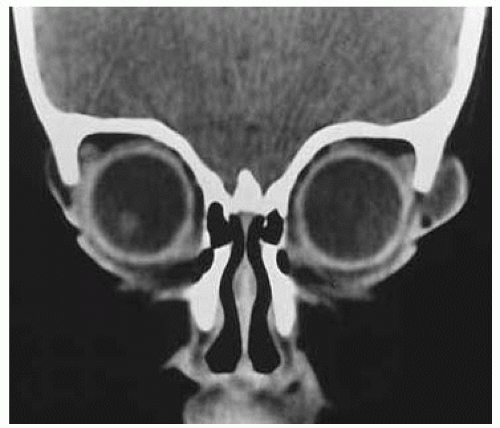 Figure 27.3. Coronal CT showing cystic lesion at the orbital rim. The lumen of the cyst is hypointense, similar to vitreous and orbital fat. |
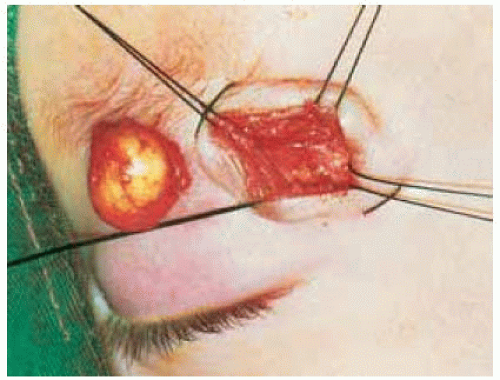 Figure 27.4. The cyst (to the left) has been removed by a cutaneous approach. One can use either an infrabrow or eyelid crease incision. The posterior aspect of the cyst is often adherent to the periosteum, requiring meticulous dissection to remove the cyst intact. |
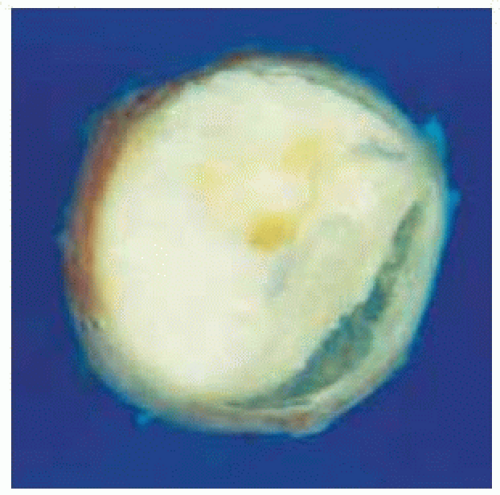 Figure 27.5. Gross appearance of cyst after fixation and sectioning. Note the capsule and the yellow material in the lumen. |
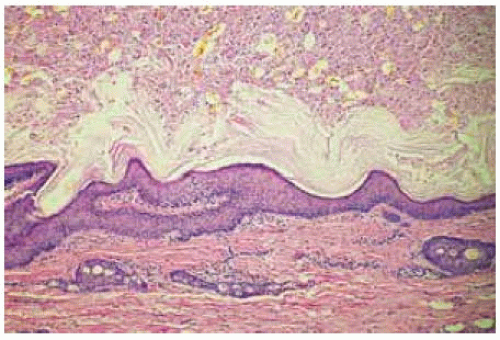 Figure 27.6. Histopathology through the cyst wall (below) and the lumen (above). The cyst is lined by keratinizing epithelium and has dermal elements (hair follicles and sebaceous glands) in the wall (below) and in the lumen (above). (Hematoxylin-eosin 25.) |
Orbital Dermoid Cyst: Lesion of Conjunctival Origin in a Child
Dermoid cysts lined by conjunctival epithelium usually occur in the orbital soft tissues nasally. It is possible that they originate from primitive epithelium destined to form the adult caruncle. In contrast with the typical dermoid cyst shown in Plate 250, this type is generally recognized in older children or adults. A clinicopathologic correlation is shown.
Shields JA, Augsburger JJ, Donoso LA. Orbital dermoid cyst of conjunctival origin. Am J Ophthalmol 1986;101:726-729.
 Figure 27.7. Soft tissue subcutaneous mass superonasally on right side in a 17-year-old woman. |
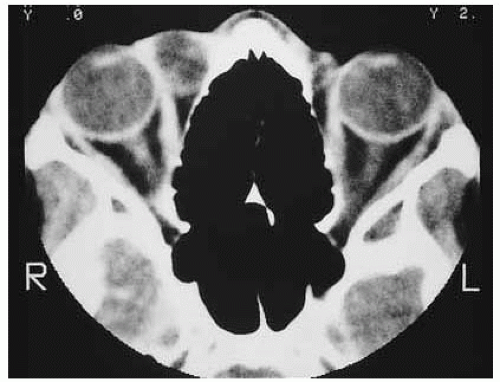 Figure 27.8. Axial computed tomography showing cystic nature of the lesion. |
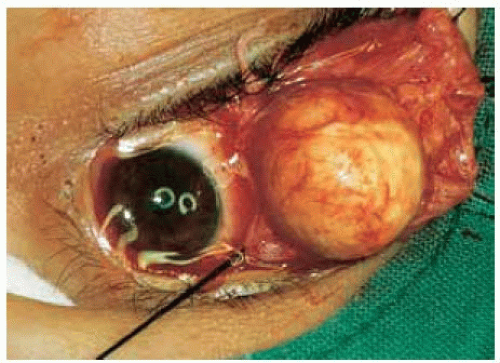 Figure 27.9. Cyst has been exposed and removed through a superonasal conjunctival approach. |
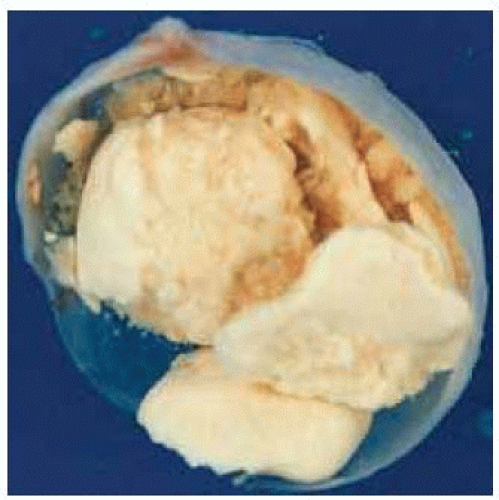 Figure 27.10. Gross appearance of cyst after fixation and sectioning. Note the very thin capsule and the yellow material in the lumen. |
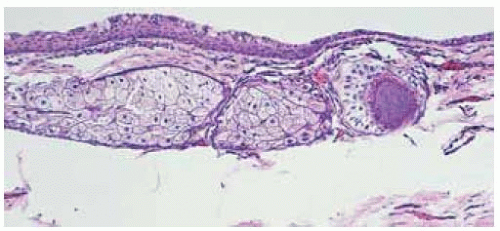 Figure 27.11. Photomicrograph showing wall of cyst with nonkeratinizing epithelium with goblet cells, hair shafts, and sebaceous glands. (Hematoxylin-eosin 25.) |
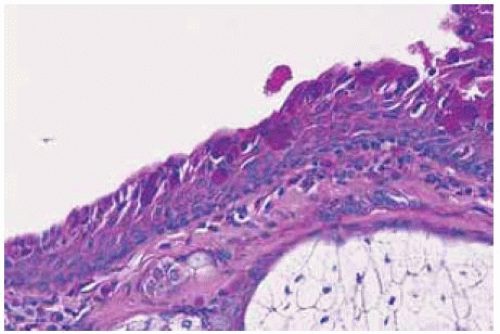 Figure 27.12. Photomicrograph showing wall of cyst with nonkeratinizing epithelium containing Periodic acid-Schiff-positive goblet cells. (Periodic acid-Schiff 50.) |
Orbital Dermoid Cyst: Lesion of Conjunctival Origin in an Adult
Although orbital dermoid cysts are congenital, the soft tissue dermoid cyst of conjunctival origin may lie dormant for many years before clinical detection. Such cysts have been recognized in patients 70 years old. A clinicopathologic correlation in a 50-year-old patient is shown.
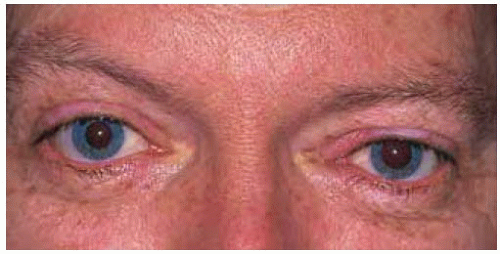 Figure 27.13. Slight blepharoptosis and inferotemporal displacement of left eye in a 50-year-old man. |
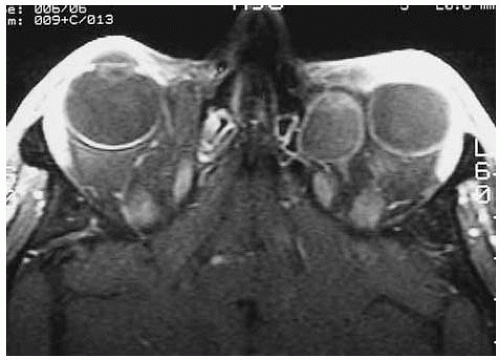 Figure 27.14. Axial magnetic resonance imaging in T1-weighted image, showing temporal displacement of left eye by cystic mass. |
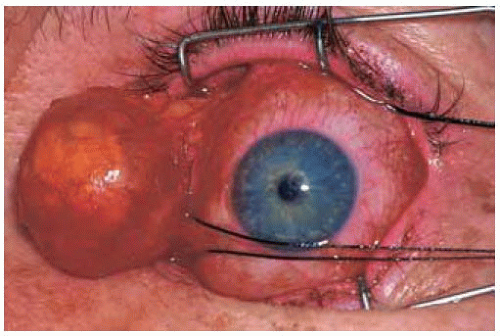 Figure 27.15. Lesion being removed intact by way of a forniceal incision in the conjunctiva. It was easily delivered by sharp and blunt orbital dissection. |
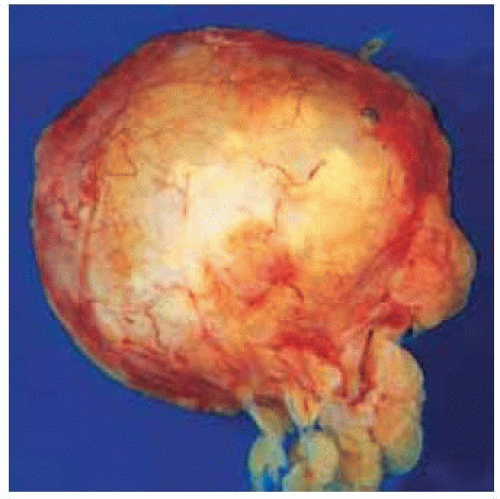 Figure 27.16. Gross appearance of the intact cyst after excision. Note the yellow material deep to the thin capsule. |
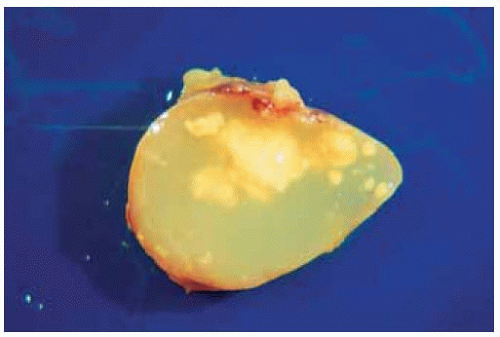 Figure 27.17. Gross appearance of cyst after fixation and sectioning. Note the very thin capsule and the yellow material in the lumen. |
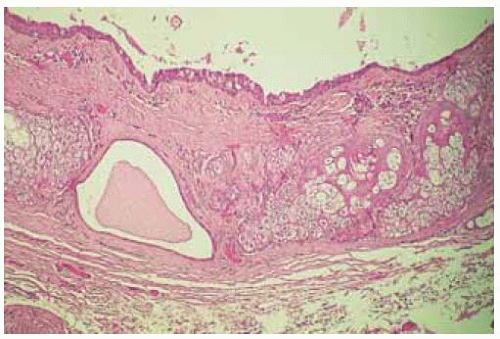 Figure 27.18. Histopathology through the cyst wall (below) and the lum en (above). The cyst is lined by nonkeratinizing epithelium with goblet cells and has dermal elements in the wall and in the lumen. (Hematoxylin-eosin 40.) |
Orbital Dermoid Cyst: Dumbbell Type
Dumbbell dermoid cysts are characterized by two cystic components connected by a channel through the adjacent bone, at the site of a bony suture. Like other subcutaneous dermoid cysts, they can break through the epidermis and produce a draining fistula.
Emerick GT, Shields CL, Shields JA, et al. Chewing-induced visual impairment from a dumbbell dermoid cyst. Ophthal Plast Reconstr Surg 1997;13:57-61.
 Figure 27.19. Subcutaneous mass temporal to left eye in a 29-year-old woman. |
 Figure 27.20. Axial computed tomography of patient shown in Figure 27.19, showing bilobed cystic lesion communicating through an enlarged zygomaticofrontal suture. Note that the lumen of the lesion is dark, similar to orbital fat. The lesion was excised piecemeal. |
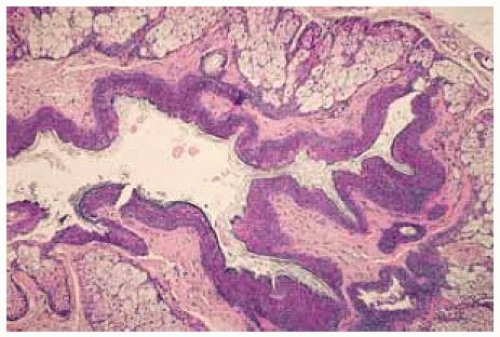 Figure 27.21. Histopathology of excised cyst shown in Figure 27.20 demonstrating the keratinizing epithelium with numerous sebaceous glands in the wall. (Hematoxylin-eosin 40.) |
 Figure 27.22. Draining cutaneous fistula superotemporal to right eye in an 8-year-old boy. Such a fistula in this location is highly suggestive of a ruptured dermoid cyst. |
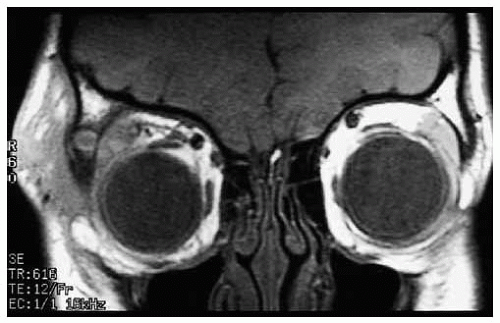 Figure 27.23. Coronal magnetic resonance imaging in T1-weighted image of patient shown in Figure 27.22 revealing the bony defect connecting the two irregular lobes of the cyst. |
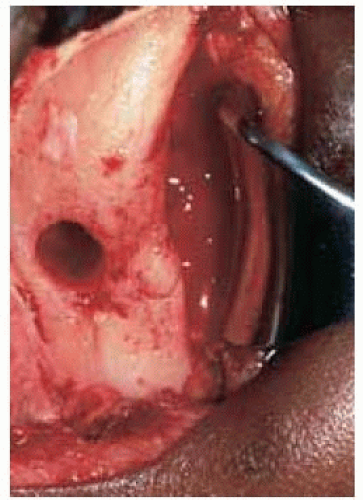 Figure 27.24. Osseous defect seen at time of surgery after piecemeal removal of the dermoid cyst in patient shown in Figure 27.22. |
Orbital Dermoid Cyst: Dumbbell Type, Surgical Resection
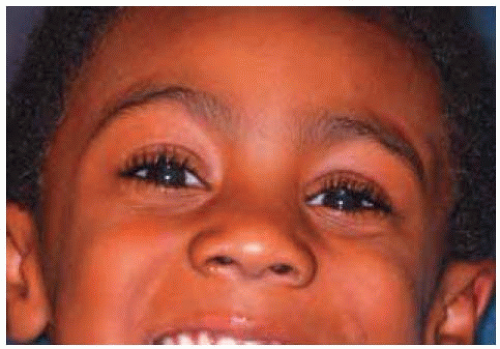 Figure 27.25. Facial appearance of 6-year-old boy. There was minimal soft tissue subcutaneous swelling temporal to left eye. |
 Figure 27.26. Axial computed tomography showing osseous defect in zygoma of left eye (to the right in the image). Note the normal bone on the contralateral side. |
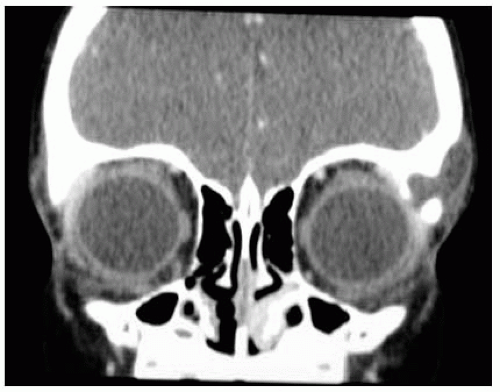 Figure 27.27. Coronal computed tomography more clearly showing the osseous defect. |
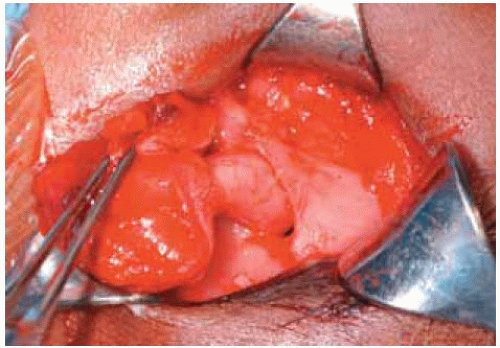 Figure 27.28. Surgical photograph showing subcutaneous component of the cyst (retracted with forceps to the left) and the tubular component of the cyst passing through the bony defect (in the center). |
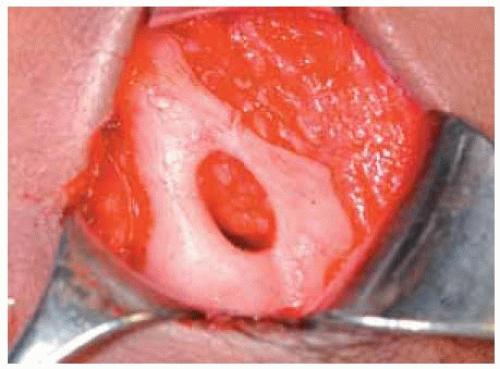 Figure 27.29. After removal of the dermoid cyst, the oval hole in the bone is clearly visualized. |
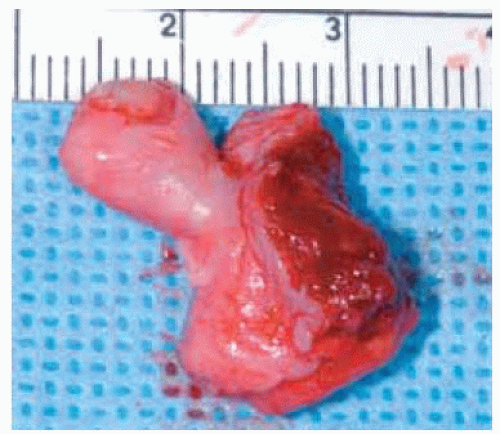 Figure 27.30. Gross appearance of the bilobed dermoid cyst immediately after surgical removal. The component up and to the left represents the tubular intraosseous component of the lesion. |
Orbital Dermoid Cyst: Deep Orbital Type
Large dermoid cysts located in the posterior orbit pose more of a diagnostic and therapeutic challenge. Such cysts can slowly grow to a large size at a young age and can recur after excision. A clinicopathologic correlation is depicted.
Leonardo D, Shields CL, Shields JA, et al. Recurrent giant orbital dermoid of infancy. J Pediatr Ophthalmol Strabismus 1994;31:50-52.
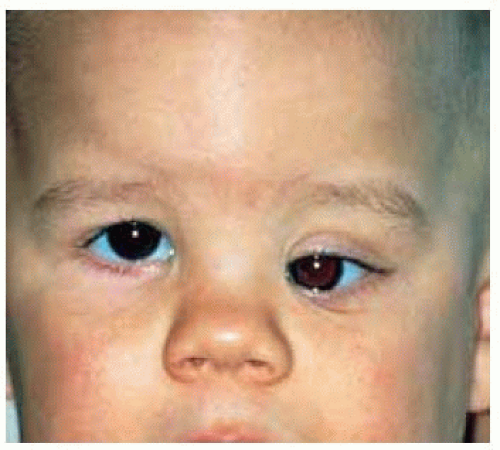 Figure 27.31. Proptosis and downward displacement of the left eye in a 2-year-old boy. The findings were noted shortly after birth and had become progressively worse. |
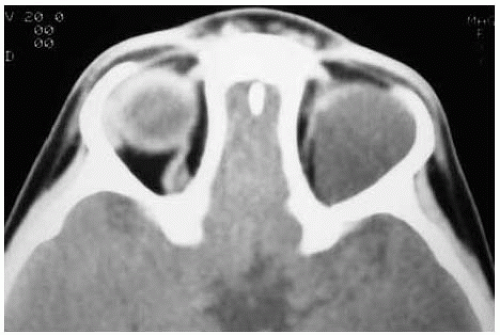 Figure 27.32. Axial computed tomography showing large superior orbital mass in the left orbit. |
 Figure 27.33. Coronal computed tomography showing mass above the globe. Note that the orbit is larger and there is superior displacement of the orbital roof. |
 Figure 27.34. Outline of incision for lateral orbitotomy. |
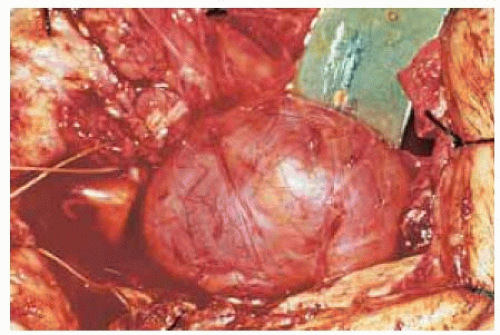 Figure 27.35. Cystic mass exposed after lateral orbitotomy. It was aspirated and removed. |
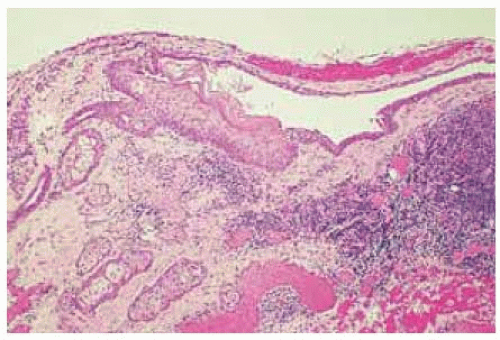 Figure 27.36 Histopathology of a portion of the collapsed cyst showing features of a dermoid cyst. Although most of the cyst was lined by nonkeratinizing epithelium similar to conjunctiva, a small portion of it showed keratinizing epithelium. The lesion recurred in the temporal orbit about 2 years later and was excised surgically with a good result. (Hematoxylin-eosin 25.) |
Orbital Simple Primary Cyst of Conjunctival
General Considerations
Simple epithelial cysts can be classified according to the type of epithelium that lines the cyst. This can be epidermis, respiratory epithelium, glandular epithelium, or conjunctiva (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16). In the authors’ series of 1,264 orbital masses, the 12 simple epithelial cysts accounted for 17% of cystic lesions and for 1% of all orbital lesions. Each type of cyst has similar clinical features and only the conjunctival epithelial cysts are described here (4).
A simple orbital cyst of conjunctival origin can be primary, without an apparent cause, or it can be secondary to surgical or nonsurgical trauma. In contrast with a dermoid cyst of conjunctival origin (discussed previously), a simple conjunctival cyst does not contain dermal appendages within its walls. In a review of 128 cases of conjunctival adnexal and dermoid cysts, there were 5 simple conjunctival cysts (7). In another series of 11 conjunctival cysts of the orbit, 6 were presumed to be primary, without a history of antecedent surgery or trauma (6).
Clinical Features
A primary conjunctival cyst can become apparent at any age, with patient ages in one series ranging from 4 to 45 years old at the time of diagnosis (7). The patient usually presents with a soft, fluctuant mass in the anterior superonasal aspect of the orbit, without visual loss, proptosis, or displacement of the globe. As the cyst enlarges, it can induce pain, tenderness, motility disturbance, displacement of the globe, and refractive error. The features of a secondary conjunctival cyst vary with the type of prior surgery or trauma. After strabismus surgery, the cyst may be visible near the insertion of the affected rectus muscle, but can extend deeper into the orbital soft tissues. After retinal detachment surgery, it can be located deeper in the orbit and affect a rectus muscle. After enucleation, it may appear as an asymptomatic mass in the anophthalmic orbit or it may cause difficulty with retention of the ocular prosthesis. This type of cyst can also occur in the anterior aspect of the orbit after conjunctival inflammations such as Stevens-Johnson syndrome (13).
Diagnostic Approaches
In many instances, the diagnosis of the orbital cyst of conjunctival origin can be established by direct visualization of a clear cyst that appears in the conjunctival region. Computed tomography and magnetic resonance imaging generally demonstrate a clear, nonenhancing cyst that is confined to orbital soft tissues without bone erosion.
Pathology and Pathogenesis
Conjunctival epithelial cyst is lined by attenuated nonkeratinizing stratified squamous epithelium without adnexal structures in its wall. The epithelium characteristically contains mucous-secreting goblet cells identical to those found in the conjunctiva. It is believed that such cysts occur as a result of misdirected cleavage of mesoderm during formation of the superior conjunctival fornix (14).
Management
The management of a suspected conjunctival orbital cyst necessarily varies from case to case. A small asymptomatic cyst can be followed without treatment. However, most larger cysts should be removed surgically, with an attempt to completely excise the lesion without disrupting its epithelial lining. This can usually be accomplished with meticulous dissection by an anterior orbital approach, depending on the size and location of the lesion.
Selected References
1. Shields JA. Cystic lesions of the orbit. Dermoid cyst. In: Shields JA, ed. Diagnosis and Management of Orbital Tumors. Philadelphia: WB Saunders; 1989:89-122.
2. Shields JA, Bakewell B, Augsburger DG, et al. Classification and incidence of space-occupying lesions of the orbit. A survey of 645 biopsies. Arch Ophthalmol 1984;102:1606-1611.
3. Shields JA, Bakewell B, Augsburger DG, et al. Space-occupying orbital masses in children. A review of 250 consecutive biopsies. Ophthalmology 1986;93:379-384.
4. Shields JA, Shields CL, Scartozzi R. Survey of 1264 patients with orbital tumors and simulating lesions: The 2002 Montgomery Lecture, part 1. Ophthalmology 2004;111:997-1008.
5. Shields JA, Shields CL. Orbital cysts of childhood—classification, clinical features, and management. The 2003 Angeline Parks Lecture. Surv Ophthalmol 2004;49:281-299.
6. Goldstein MH, Soparkar CN, Kersten RC, et al. Conjunctival cysts of the orbit. Ophthalmology 1998;105:2056-2060.
7. Jakobiec FA, Bonanno PA, Sigelman J. Conjunctival adnexal cysts and dermoid. Arch Ophthalmol 1978;96:1404-1409.
8. Metz HS, Searl S, Rosenberg P, et al. Giant orbital cyst after strabismus surgery. JAAPOS 1999;3:185-187.
9. Basar E, Pazarli H, Ozdemir H, et al. Subconjunctival cyst extending into the orbit. Int Ophthalmol 1998;22:341-343.
10. De Potter P, Kunin AW, Shields CL, et al. Massive orbital cyst of the lateral rectus muscle after retinal detachment surgery. Ophthal Plast Reconstr Surg 1993;9:292-297.
11. Johnson DW, Bartley GB, Garrity JA, et al. Massive epithelium-lined cyst after scleral buckling. Am J Ophthalmol 1992;113:439-444.
12. Smit TJ, Koornneef L, Zonneveld FW. Conjunctival cysts in anophthalmic orbits. Br J Ophthalmol 1991;75:342-343.
13. Desai V, Shields CL, Shields JA. Orbital cyst in a patient with Stevens Johnson syndrome, Cornea 1992;11:592-594.
14. Rose GE, O’Donnell BA. Congenital orbital cysts associated with the common sheath of superior rectus and levator palpebrae superioris muscles Ophthalmology 1995;102:135-138.
15. Boynton JR, Searl SS, Ferry AP, et al. Primary nonkeratinized epithelial (“conjunctival”) orbital cysts. Arch Ophthalmol 1992;110:1238-1242.
16. McCarthy RW, Beyer CK, Dallow RL, et al. Conjunctival cysts of the orbit following enucleation. Ophthalmology 1981;88:30-35.
Orbital Cyst of Conjunctival Origin: Primary Idiopathic Type
Some orbital cysts are lined by conjunctival epithelium without dermal elements in the cyst wall. A cyst of this type is called a “simple conjunctival epithelial cyst of the orbit.” Such a cyst can occur as an idiopathic lesion or it can be secondary to implantation of conjunctival epithelium after surgical or nonsurgical trauma. A clinicopathologic correlation of the idiopathic variant is shown.
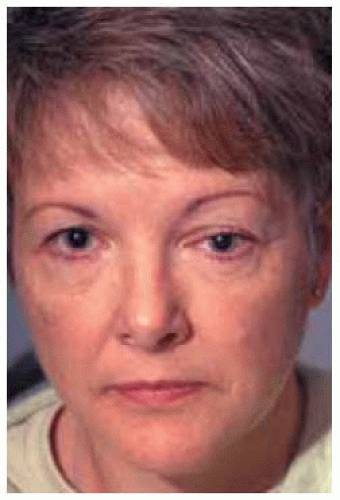 Figure 27.37. Facial appearance of a 52-year-old woman with proptosis and downward displacement of left eye. |
 Figure 27.38. Closer view showing both eyes. |
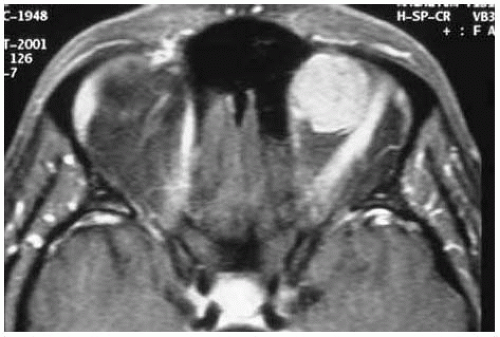 Figure 27.39. Axial magnetic resonance imaging in T1-weighted image showing hyperintense mass in orbit superonasally. |
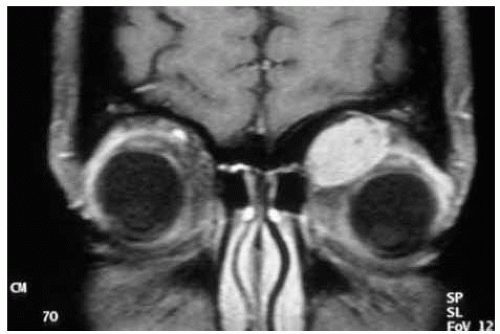 Figure 27.40. Coronal magnetic resonance imaging in T1-w eighted image further delineating the mass in the orbit superonasally. |
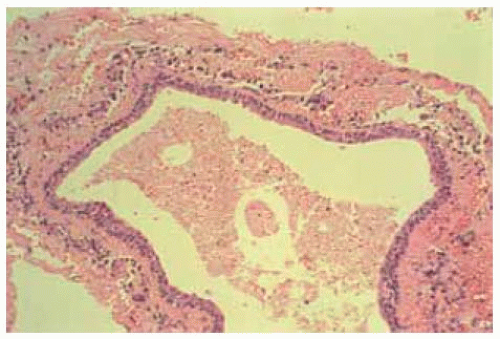 Figure 27.41. Photomicrograph showing cyst lined by nonkeratinizing stratified epithelium compatible with conjunctival epithelium. No goblet cells are appreciated in this field. The lumen contains necrotic cellular debris. (Hematoxylin-eosin 25.) |
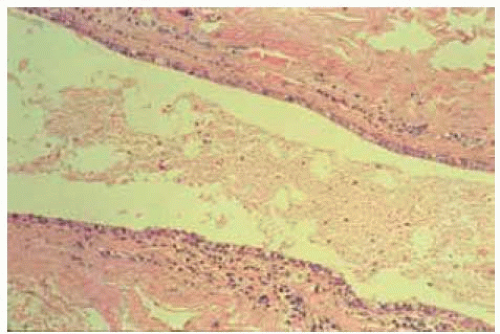 Figure 27.42. Slightly higher magnification photomicrograph of same lesion showing mild infiltration of chronic inflammatory cells in the cyst wall but no dermal structure. (Hematoxylin-eosin 25.) |
Orbital Cyst of Conjunctival Origin: Secondary Type, After Enucleation
An orbital cyst can develop in an anophthalmic orbit following enucleation for any cause. It presumably arises from rests of conjunctival epithelium. Depicted is a clinicopathologic correlation of a orbital conjunctival cyst that developed years after enucleation for retinoblastoma.
 Figure 27.43. Downward displacement and proptosis of the enucleation prosthesis in an 18-year-old man who underwent enucleation elsewhere for retinoblastoma 16 years earlier. |
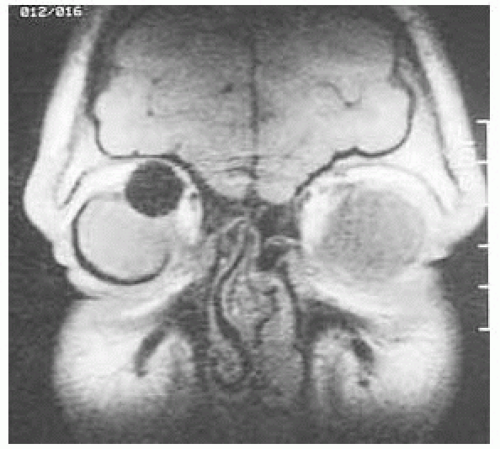 Figure 27.44. Coronal magnetic resonance imaging showing large cyst, the size of a normal globe, displacing the silastic ball implant superonasally. |
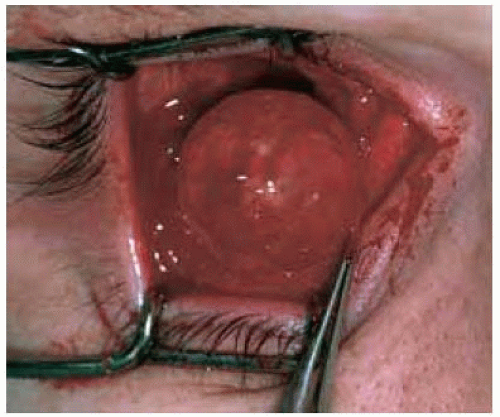 Figure 27.45. View of implant at the time of surgery to remove the cyst. |
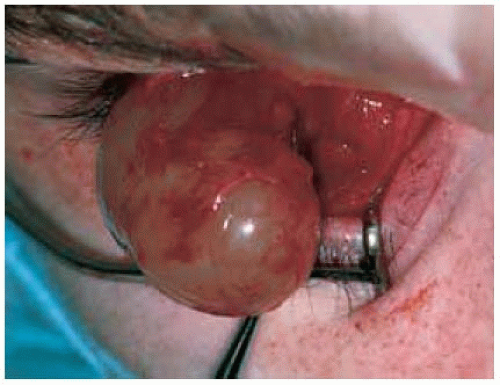 Figure 27.46. View of the large cyst that is being rem oved after the implant was taken out. |
 Figure 27.47. Appearance of cyst (to the left) and the removed implant (to the right) immediately after surgical removal. |
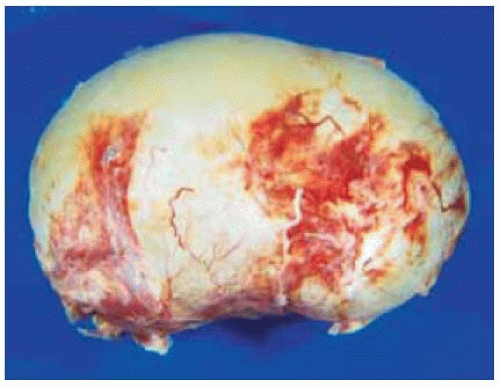 Figure 27.48. Gross view of the cyst after fixation. The clear cyst was lined by conjunctival epithelium. |
Orbital Cyst of Conjunctival Origin: Secondary Type, After Retinal Detachment Surgery
An orbital cyst can develop after retinal detachment surgery, presumably from displacement of conjunctival epithelium into the deeper orbital tissues. A clinicopathologic correlation is shown.
De Potter P, Kunin AW , Shields CL, et al. Massive orbital cyst of the lateral rectus muscle after retinal detachment surgery. Ophthal Plast Reconstr Surg 1993;9:292-297.
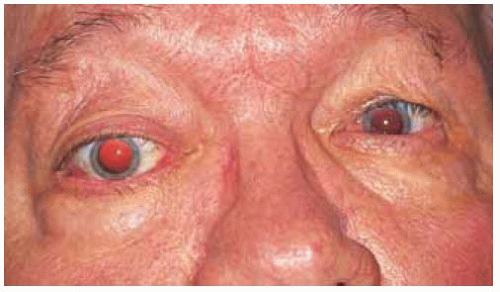 Figure 27.49. Proptosis of the right eye in a 76-year-old man who had undergone ipsilateral retinal detachment surgery several years earlier. |
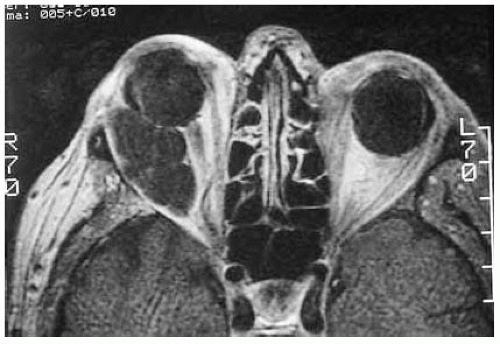 Figure 27.50. Axial magnetic resonance imaging in T1-w eighted image, showing irregular cyst in lateral portion of orbit. |
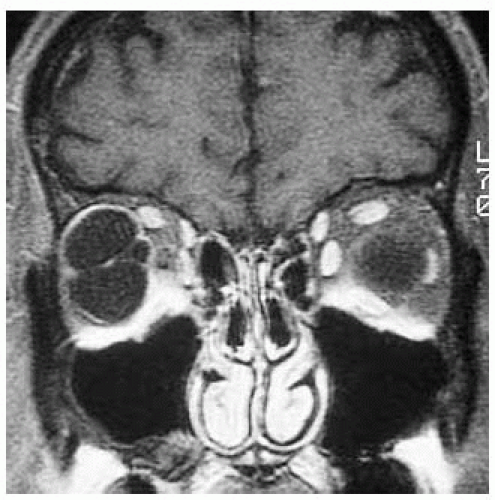 Figure 27.51. Coronal magnetic resonance imaging in T1-w eighted image showing the cyst. |
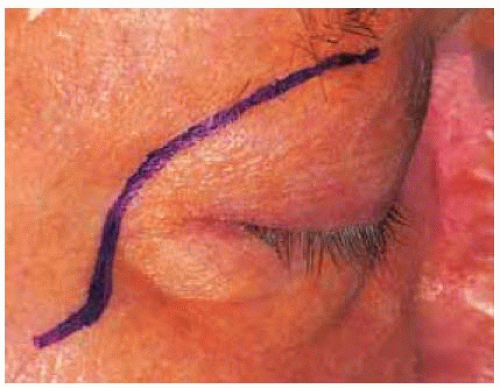 Figure 27.52. Outline of superotemporal orbitotomy incision to remove the cyst. |
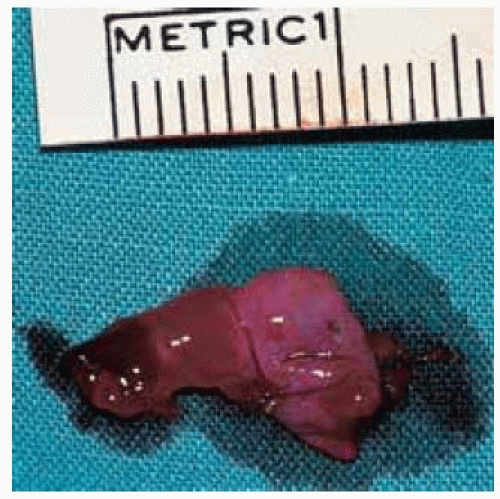 Figure 27.53. A portion of the collapsed cyst is shown after it was aspirated and removed piecemeal. |
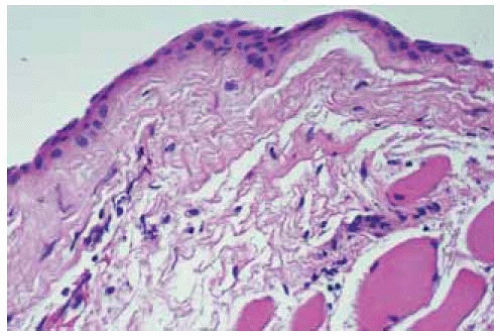 Figure 27.54. Histopathology of the wall of the cyst showing nonkeratinizing epithelium. (Hematoxylin-eosin 25.) |
Orbital Cyst: Simple Conjunctival Type Associated With Stevens-Johnson Syndrome
It is possible that adhesions between the tarsal and bulbar conjunctiva can entrap conjunctival epithelium and lead to a cyst. That may have been the mechanism in this case.
Desai V, Shields CL, Shields JA. Orbital cyst in a patient with Stevens-Johnson syndrome, Cornea 1992;11:592-594.)
 Figure 27.55. Blepharoptosis of an irritated, uncomfortable right eye in a 10-year-old girl who had Stevens-Johnson syndrome with severe ocular involvement. The cyst had recurred after simple aspiration. |
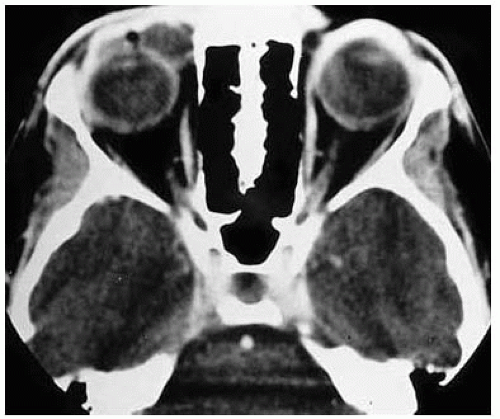 Figure 27.56. Axial computed tomography showing cystic lesion superior and nasal to the globe. |
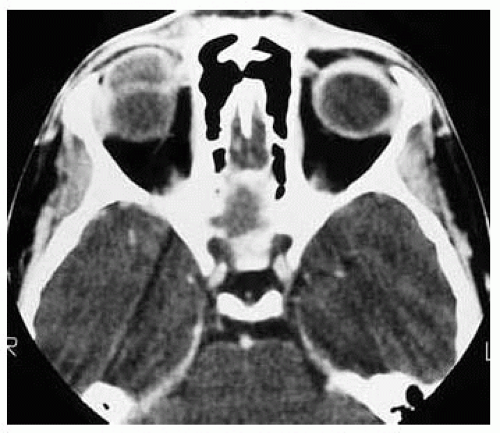 Figure 27.57. Axial computed tomography at a higher level, showing extent of the cyst. |
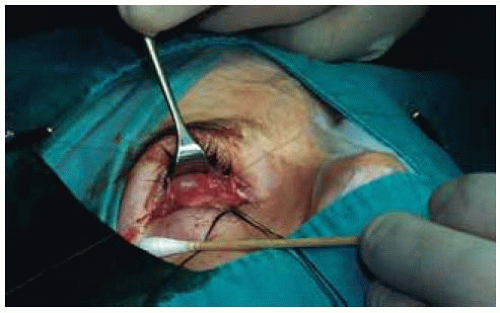 Figure 27.58. Surgical view of the cyst beneath the superior fornix. The cyst was removed and a buccal mucous membrane graft was done. |
 Figure 27.59. Histopathology showing nonkeratinizing epithelium surrounded by dense fibrosis secondary to chronic inflammation. (Hematoxylin-eosin 10.) |
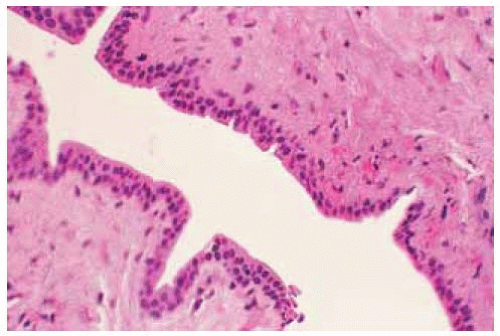 Figure 27.60. Histopathology on slightly higher power, showing nonkeratinizing epithelium. (Hematoxylin-eosin 30.) |
Orbital Teratoma (Teratomatous Cyst)
General Considerations
Teratoma is a congenital, multicystic mass that most often occurs in the gonads but can occur in other sites, including the orbit (1,2,3,4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23,24). By strict definition, a true teratoma contains histologic structures representing all three embryonic germ layers: ectoderm, mesoderm, and endoderm. Orbital teratoma is sufficiently uncommon that individual case reports are usually cited in the literature. In a review of literature in 1980 the authors cited 51 reported cases of true orbital teratoma (19). Almost all of the reported cases were unilateral, but there are occasional reports of bilateral cases. There appears to be a 2:1 female preponderance and a slight preference for the left eye. Although teratomas in other parts of the body have been known to undergo malignant transformation, teratomas that are confined to the orbit are generally benign. Malignant transformation of pure orbital teratoma has been reported, but there is controversy as to the validity of some of those reports (17,21). Surprisingly, there were no orbital teratomas among the 1,264 consecutive orbital space-occupying lesions seen on the oncology service (4).
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


