Orbit
7.1 ORBITAL DISEASE
This section provides a framework to evaluate a variety of orbital diseases.
Symptoms
Eyelid swelling, bulging eye(s), and double vision are common. Pain and decreased vision can occur.
Signs
Critical. Proptosis and restriction of ocular motility, which can be confirmed by forced-duction testing (see Appendix 6, Forced-Duction Test and Active Force Generation Test). Resistance to retropulsion of the globe is common.
Differential Diagnosis of Pseudoproptosis
 Enlarged globe (e.g., myopia). Large, myopic eyes frequently have tilted discs and peripapillary crescents, and ultrasonography (US) reveals a long axial length.
Enlarged globe (e.g., myopia). Large, myopic eyes frequently have tilted discs and peripapillary crescents, and ultrasonography (US) reveals a long axial length.
 Enophthalmos of the fellow eye (e.g., after an orbital floor fracture).
Enophthalmos of the fellow eye (e.g., after an orbital floor fracture).
 Asymmetric eyelid position: Unilateral upper and/or lower eyelid retraction, or contralateral upper eyelid ptosis.
Asymmetric eyelid position: Unilateral upper and/or lower eyelid retraction, or contralateral upper eyelid ptosis.
Etiology
Rarely, specific signs of orbital disease are diagnostic. Otherwise, orbital disease can be grouped into five broad categories to help tailor the necessary work-up:
1. Inflammatory: Thyroid eye disease (TED), idiopathic orbital inflammatory syndrome (IOIS), sarcoidosis, Wegener granulomatosis, etc.
2. Infectious: Orbital cellulitis, subperiosteal abscess, etc.
3. Neoplastic (benign and malignant): Dermoid cyst, capillary hemangioma, rhabdomyosarcoma, metastasis, lymphangioma, optic nerve glioma, neurofibroma, leukemia, lymphoproliferation (including lymphoma), neurilemmoma, mucocele, etc.
4. Trauma: Orbital fracture, retrobulbar hemorrhage, orbital foreign body, carotid-cavernous fistula, etc.
5. Malformation: Congenital, vascular, etc.
Work-Up
1. History: Rapid or slow onset? Pain? Ocular bruit and/or pulsation? Fever, chills, systemic symptoms? History of cancer, diabetes, pulmonary disease, or renal disease? Skin rash? Trauma?
2. Vital signs, particularly temperature.
3. External examination:
—In addition to classic axial exophthalmos, also look for nonaxial displacement of the globe (e.g., hypoglobus, hyperglobus).
—Test for resistance to retropulsion by gently pushing each globe into the orbit with your thumbs.
—Feel along the orbital rim for a mass. Check the conjunctival cul-de-sacs carefully and evert the upper eyelid.
—Check extraocular movements. Measure any ocular misalignment with prisms (see Appendix 3, Cover/Uncover and Alternate Cover Tests).
—To examine for proptosis, tilt the patient’s head back and look from below (“ant’s-eye view”). Measure with a Hertel exophthalmometer. Position the exophthalmometer against the lateral orbital rims, not the lateral canthi. Upper limits of normal are approximately 22 and 24 mm in white people and black people, respectively. A difference between the two eyes of more than 2 mm is considered abnormal. Can be used in conjunction with a Valsalva maneuver if a venous malformation is suspected.
4. Ocular examination: Specifically check the size and reactivity of the pupils, visual fields, color vision (by color plates), intraocular pressure (IOP), optic nerves (pallor, swelling), posterior pole (especially for chorioretinal folds), and peripheral retina.
5. Imaging studies: Orbital computed tomography (CT) (axial and coronal views) or magnetic resonance imaging (MRI) with gadolinium and fat suppression, depending on suspected etiology. Orbital US with or without color Doppler imaging is useful if the diagnosis is uncertain or when a cystic or vascular lesion is suspected. See Chapter 14, Imaging Modalities in Ophthalmology.
6. Laboratory tests when appropriate: Triiodothyronine (T3), thyroxine (T4), selective thyroid-stimulating hormone (TSH), thyroid-stimulating immunoglobulin, complete blood count (CBC) with differential, Westergren erythrocyte sedimentation rate (ESR), antinuclear antibody (ANA), blood urea nitrogen (BUN)/creatinine (if CT contrast or gadolinium are indicated in at-risk individuals), fasting blood sugar, blood cultures, angiotensin-converting enzyme (ACE), cytoplasmic antineutrophil cytoplasmic antibody (cANCA), prostate-specific antigen, lactate dehydrogenase, etc.
7. Consider a forced-duction test in select cases. See Appendix 6, Forced-Duction Test and Active Force Generation Test.
8. Consider an excisional or incisional biopsy, as dictated by the working diagnosis. Fine-needle aspiration biopsy has a limited role in orbital diagnosis.
Additional work-up, treatment, and follow-up vary according to the suspected diagnosis. See individual sections.
7.2 INFLAMMATORY ORBITAL DISEASE
7.2.1. THYROID EYE DISEASE
Synonyms: THYROID-RELATED ORBITOPATHY
OR GRAVES DISEASE
Ocular Symptoms
Early: Nonspecific complaints including foreign-body sensation, redness, tearing, photophobia, and morning puffiness of the eyelids. Early symptoms are often nonspecific and may mimic allergy, blepharoconjunctivitis, chronic conjunctivitis, etc.
Late: Eyelid and orbital symptoms including eyelid retraction, prominent eyes, persistent eyelid swelling, double vision, “pressure” behind the eyes, and decreased vision in one or both eyes.
Signs
(See Figure 7.2.1.1.)

FIGURE 7.2.1.1. Thyroid-related orbitopathy with eyelid retraction and proptosis of the right eye.
Critical. Retraction of the upper eyelids (highly specific) with lateral flare and eyelid lag on downward gaze (von Graefe sign), lagophthalmos. Lower lid retraction is less specific for TED. Unilateral or bilateral axial proptosis with variable resistance to retropulsion. When extraocular muscles are involved, elevation and abduction are commonly restricted and there is resistance on forced-duction testing. Although often bilateral, unilateral or asymmetric TED is also frequently seen. Thickening of the extraocular muscles (inferior, medial, superior, and lateral, in order of frequency) without involvement of the associated tendons may be noted on orbital imaging. Isolated enlargement of the superior or lateral recti muscles is highly atypical of TED and requires further work-up.
NOTE: Optic nerve compression caused by thickened extraocular muscles at the orbital apex can produce an afferent pupillary defect, reduced color vision, visual field, and visual acuity loss. Compressive optic neuropathy occurs in a minority of patients (5%) with TED but must be ruled out in every patient at every visit. Optic neuropathy in the setting of TED almost invariably occurs in the setting of restrictive strabismus and increased resistance to retropulsion. Counterintuitively, in cases of compressive optic neuropathy from TED, axial proptosis is usually either absent or mild.
Other. Reduced frequency of blinking, inferior chemosis, significantly elevated IOP (especially in upgaze), injection of the blood vessels over the insertion sites of horizontal rectus muscles, superior limbic keratoconjunctivitis, superficial punctate keratopathy, or infiltrate or ulceration from exposure keratopathy.
Systemic Signs
Hyperthyroidism is common. Symptoms include a rapid pulse, hot and dry skin, diffusely enlarged thyroid gland (goiter), weight loss, muscle wasting with proximal muscle weakness, hand tremor, pretibial dermopathy or myxedema, cardiac arrhythmias. Some patients are hypo- or euthyroid. Euthyroid patients should undergo thyroid function testing every 6 to 12 months; a significant proportion will develop thyroid abnormalities. Concomitant myasthenia gravis with fluctuating double vision and ptosis may occur in a minority of patients. TED does not necessarily follow the associated thyroid dysfunction and may occur months to years before or after the thyroid dysfunction. The clinical progression of TED also has only minimal correlation to control of the thyroid dysfunction.
Differential Diagnosis of Eyelid Retraction
 Previous eyelid surgery may produce eyelid retraction or eyelid lag.
Previous eyelid surgery may produce eyelid retraction or eyelid lag.
 Severe contralateral ptosis may produce eyelid retraction because of Hering Law, especially if the nonptotic eye is amblyopic.
Severe contralateral ptosis may produce eyelid retraction because of Hering Law, especially if the nonptotic eye is amblyopic.
 Third cranial nerve palsy with aberrant regeneration: The upper eyelid may elevate with downward gaze, simulating eyelid lag (pseudo-von Graefe sign). Ocular motility may be limited, but results of forced-duction testing and orbital imaging are normal. Eyelid retraction is typically accentuated in adduction or in downgaze. See 10.6, Aberrant Regeneration of the Third Nerve.
Third cranial nerve palsy with aberrant regeneration: The upper eyelid may elevate with downward gaze, simulating eyelid lag (pseudo-von Graefe sign). Ocular motility may be limited, but results of forced-duction testing and orbital imaging are normal. Eyelid retraction is typically accentuated in adduction or in downgaze. See 10.6, Aberrant Regeneration of the Third Nerve.
 Parinaud syndrome: Eyelid retraction and limitation of upward gaze may accompany convergence-retraction nystagmus and mildly dilated pupils that react poorly to light with an intact near response (light-near dissociation).
Parinaud syndrome: Eyelid retraction and limitation of upward gaze may accompany convergence-retraction nystagmus and mildly dilated pupils that react poorly to light with an intact near response (light-near dissociation).
Work-Up
1. History: Duration of symptoms? Pain? Change in vision? Known thyroid disease or cancer? Smoker?
2. Complete ocular examination to establish the diagnosis and to determine whether the patient is developing exposure keratopathy (slit-lamp examination with fluorescein staining) or optic nerve compression (afferent pupillary defect, color plate deficiency, optic nerve edema). Diplopia is measured with prisms (see Appendix 3, Cover/Uncover and Alternate Cover Tests) and proptosis is measured with a Hertel exophthalmometer. Check IOP in both primary and upgaze (increase in upgaze correlated with severity of inferior rectus muscle enlargement). Dilated fundus examination with optic nerve assessment.
3. CT of the orbit (axial and coronal views without contrast) is performed when presentation is atypical (e.g., all cases of unilateral proptosis or any bilateral proptosis without upper eyelid retraction), or in the presence of severe congestive orbitopathy or optic neuropathy. CT in TED varies from patient to patient. In patients with restrictive strabismus and minimal proptosis (“myogenic variant”), imaging may show thickened extraocular muscles without the involvement of the associated tendons. In patients with full or nearly full extraocular motility, severe proptosis, and exposure keratopathy (“lipogenic variant”), increased fat volume with minimal muscle involvement is typical.
4. Formal visual field testing when signs or symptoms of optic nerve compression are present.
5. Thyroid function tests (T3, T4, selective TSH). These may be normal. Thyroid-stimulating immunoglobulin is sometimes ordered, but the clinical significance of this test is still unclear.
6. Work-up for suspected myasthenia gravis is necessary in selected cases. See 10.11, Myasthenia Gravis.
Treatment
1. Smoking cessation: All patients with TED who smoke must be explicitly told that continued tobacco use increases the risk of progression and the severity of the orbitopathy. This conversation should be clearly documented in the medical record.
2. Refer the patient to a medical internist or endocrinologist for management of systemic thyroid disease, if present. If TFTs are normal, the patient’s TFTs should be checked every 6 to 12 months.
3. Treat exposure keratopathy with artificial tears and lubrication or by taping eyelids closed at night (see 4.5, Exposure Keratopathy). Swimmer’s goggles at night may be helpful. The use of topical cyclosporine drops for the treatment of ocular surface inflammation in TED is still under investigation, but is a reasonable long-term treatment option if dry-eye syndrome is present.
4. Treat eyelid edema with cold compresses in the morning and head elevation at night. The use of systemic diuretics for eyelid edema is controversial and is usually not recommended.
5. Indications for orbital decompression surgery include: Optic neuropathy, worsening or severe exposure keratopathy despite adequate treatment, globe luxation, uncontrollably high IOP, cosmesis.
6. A stepwise approach is used for surgical treatment, starting with orbital decompression (if needed), followed by strabismus surgery (for significant strabismus, if present), followed by eyelid surgery. Alteration of this sequence may lead to unpredictable results.
The following recommendations are somewhat controversial:
 Corticosteroids: During the acute inflammatory phase, prednisone 1 mg/kg p.o. q.d., tapered over 4 to 6 weeks, is a reasonable temporizing measure to improve proptosis and diplopia in preparation for orbital decompression surgery. Recently, pulse intravenous corticosteroids have been recommended in the European literature to arrest the progression of the orbitopathy. The dosing schedule is still under investigation, but is being used more frequently by clinicians. Corticosteroid injection into the orbital fat for local control of orbitopathy has also been described, but at present the efficacy of this modality remains unclear. Chronic systemic corticosteroids for long-term management have been advocated by some, but in general should be avoided because of the systemic side effects.
Corticosteroids: During the acute inflammatory phase, prednisone 1 mg/kg p.o. q.d., tapered over 4 to 6 weeks, is a reasonable temporizing measure to improve proptosis and diplopia in preparation for orbital decompression surgery. Recently, pulse intravenous corticosteroids have been recommended in the European literature to arrest the progression of the orbitopathy. The dosing schedule is still under investigation, but is being used more frequently by clinicians. Corticosteroid injection into the orbital fat for local control of orbitopathy has also been described, but at present the efficacy of this modality remains unclear. Chronic systemic corticosteroids for long-term management have been advocated by some, but in general should be avoided because of the systemic side effects.
 Orbital irradiation: The use of orbital radiation in the management of TED is still under active debate. It may be used as a modality in the acute inflammatory phase of TED. Irradiation may have a limited benefit for the management of diplopia and compressive optic neuropathy, but does not improve proptosis in TED. It may, however, prevent the progression of disease and provide long-term control. Should be used with caution in patients with diabetes, as it may worsen diabetic retinopathy, and in vasculopaths, as it may increase the risk of radiation retinopathy or optic neuropathy. As a result, all patients offered radiation therapy should be informed of the potential risks.
Orbital irradiation: The use of orbital radiation in the management of TED is still under active debate. It may be used as a modality in the acute inflammatory phase of TED. Irradiation may have a limited benefit for the management of diplopia and compressive optic neuropathy, but does not improve proptosis in TED. It may, however, prevent the progression of disease and provide long-term control. Should be used with caution in patients with diabetes, as it may worsen diabetic retinopathy, and in vasculopaths, as it may increase the risk of radiation retinopathy or optic neuropathy. As a result, all patients offered radiation therapy should be informed of the potential risks.
Radiation is best performed according to strict protocols with carefully controlled dosage and shielding, under the supervision of a radiation oncologist familiar with the technique. Typically, a total dose of 2,000 cGy is administered in 10 fractions over 2 weeks.
Treatment may transiently exacerbate inflammatory changes, and a methylprednisolone dose pack may mitigate these symptoms. Improvement is often seen within a few weeks of treatment, but may take several months to attain maximal effect. It is unusual for radiation to succeed if a trial of corticosteroids has failed.
 Biologics: Limited data are available on the use of biologic agents (rituximab, infliximab) for the treatment of TED that is progressing despite the use of more conventional therapy. At present, small series have shown promise, but the use of such agents is off-label and should be considered experimental.
Biologics: Limited data are available on the use of biologic agents (rituximab, infliximab) for the treatment of TED that is progressing despite the use of more conventional therapy. At present, small series have shown promise, but the use of such agents is off-label and should be considered experimental.
 Visual loss from optic neuropathy: Treat immediately with prednisone 100 mg p.o. q.d with close monitoring. Radiation therapy may be offered for mild-to-moderate optic neuropathy, with the understanding that there is typically a lag in the treatment effect. Posterior orbital decompression surgery (for mild-to-severe optic neuropathy) is usually effective in rapidly reversing or stabilizing the optic neuropathy. The role of anterior or soft-tissue (fat) decompression for compressive optic neuropathy is controversial and in all likelihood has a very limited effect. Decompression of the medial orbital apex typically results in the reversal of the optic neuropathy, but recurrence is possible if orbital inflammation progresses. Isolated deep lateral wall decompression has also been advocated by some specialists.
Visual loss from optic neuropathy: Treat immediately with prednisone 100 mg p.o. q.d with close monitoring. Radiation therapy may be offered for mild-to-moderate optic neuropathy, with the understanding that there is typically a lag in the treatment effect. Posterior orbital decompression surgery (for mild-to-severe optic neuropathy) is usually effective in rapidly reversing or stabilizing the optic neuropathy. The role of anterior or soft-tissue (fat) decompression for compressive optic neuropathy is controversial and in all likelihood has a very limited effect. Decompression of the medial orbital apex typically results in the reversal of the optic neuropathy, but recurrence is possible if orbital inflammation progresses. Isolated deep lateral wall decompression has also been advocated by some specialists.
Follow-Up
1. Optic nerve compression requires immediate attention and close follow-up.
2. Patients with advanced exposure keratopathy and severe proptosis also require prompt attention and close follow-up.
3. Patients with minimal-to-no exposure problems and mild-to-moderate proptosis are reevaluated every 3 to 6 months. Because of the potential risk of optic neuropathy, patients with restrictive strabismus may be followed more frequently and are instructed to check for red desaturation on a weekly basis.
4. Patients with fluctuating diplopia or ptosis should be evaluated for myasthenia gravis.
5. All patients with TED are instructed to return immediately with any new visual problems, worsening diplopia, or significant ocular irritation.
7.2.2. IDIOPATHIC ORBITAL INFLAMMATORY SYNDROME
Synonyms: INFLAMMATORY ORBITAL PSEUDOTUMOR
Symptoms
May be acute, recurrent, or chronic. An explosive, painful onset is the hallmark of idiopathic orbital inflammatory syndrome (IOIS). Pain, prominent red eye, “boggy” pink eyelid edema, double vision, or decreased vision. Children may have concomitant constitutional symptoms (fever, headache, vomiting, abdominal pain, lethargy) and bilateral presentation, which are not typical in adults.
Signs
Critical. Proptosis and/or restriction of ocular motility, usually unilateral, typically of explosive onset. On imaging studies, soft-tissue anatomy is involved in varying degrees. The extraocular muscles are thickened in cases of myositis, with involvement of the associated tendons. The sclera (in posterior scleritis), Tenon capsule (in tenonitis), orbital fat, or lacrimal gland (in dacryoadenitis) may be involved. The paranasal sinuses are usually clear.
Other. Boggy, pink eyelid erythema and edema, conjunctival injection and chemosis, lacrimal gland enlargement or a palpable orbital mass, decreased vision, uveitis, increased IOP, hyperopic shift, optic nerve swelling or atrophy (uncommon).
NOTE: Bilateral IOIS in adults can occur, but should prompt a careful evaluation to rule out a systemic cause (e.g., sarcoidosis, Wegener granulomatosis, metastases, lymphoma). Children may have bilateral disease in one-third of the cases and may have associated systemic disorders.
Differential Diagnosis
 Orbital cellulitis and/or abscess.
Orbital cellulitis and/or abscess.
 TED.
TED.
 Other inflammatory conditions (e.g., sarcoidosis, Wegener granulomatosis).
Other inflammatory conditions (e.g., sarcoidosis, Wegener granulomatosis).
 Lymphoproliferative disease (including lymphoma).
Lymphoproliferative disease (including lymphoma).
 Primary orbital malignancy.
Primary orbital malignancy.
 Metastasis.
Metastasis.
 Rhabdomyosarcoma.
Rhabdomyosarcoma.
 Leaking dermoid cyst.
Leaking dermoid cyst.
 Lymphangioma with acute hemorrhage.
Lymphangioma with acute hemorrhage.
 Spontaneous orbital hemorrhage.
Spontaneous orbital hemorrhage.
 Necrotic choroidal melanoma.
Necrotic choroidal melanoma.
Work-Up
See 7.1, Orbital Disease, for general orbital work-up.
1. History: Previous episodes? Any other systemic symptoms or diseases? History of cancer? Smoking? Last mammogram, chest X-ray, colonoscopy, prostate examination? History of breathing problems? A careful review of systems is warranted.
2. Complete ocular examination, including ocular motility, exophthalmometry, IOP, and optic nerve evaluation.
3. Vital signs, particularly temperature.
4. Orbital CT (axial and coronal views) with contrast: may show a thickened posterior sclera (the “ring sign” of 360 degrees of scleral thickening), orbital fat or lacrimal gland involvement, or thickening of the extraocular muscles (including their tendons). Bony erosion is very rare in IOIS and warrants further work-up.
5. Blood tests as needed (e.g., bilateral or atypical cases): ESR, CBC with differential, ANA, BUN, creatinine, and fasting blood sugar (before instituting systemic steroids). Consider checking ACE levels and a chest X-ray if sarcoidosis is suspected and cANCA if Wegener granulomatosis is suspected. Mammography, chest imaging, and prostate evaluation are warranted in specific or atypical cases.
6. Consider incisional biopsy when the diagnosis is uncertain, the case is atypical or recurrent, the patient has a history of cancer, or a patient with an acute presentation does not respond to adequate systemic steroids within a few days. Also consider biopsy in cases of presumed inflammatory dacryoadenitis, because this procedure carries a low morbidity, and the use of corticosteroids may mask the true pathology on future biopsy.
Treatment
1. Prednisone 80 to 100 mg p.o. q.d. as an initial dose in an adult, along with gastric prophylaxis (e.g., ranitidine 150 mg p.o. b.i.d.). Pediatric dosages typically begin with 1 mg/kg/day of prednisone. All patients are warned about potential systemic side effects and are instructed to follow up with their primary physicians to monitor blood sugar and electrolytes.
2. Low-dose radiation therapy may be used when the patient does not respond to systemic corticosteroids, when disease recurs as corticosteroids are tapered, or when corticosteroids pose a significant risk to the patient. Radiation therapy should only be used once orbital biopsy has excluded other etiologies.
Follow-Up
Reevaluate in 1 to 2 days. Patients who respond to steroids are maintained at the initial dose for 3 to 5 days, followed by a slow taper to 40 mg/day over 2 weeks, and an even slower taper below 20 mg/day, usually over several weeks. If the patient does not respond dramatically to appropriate corticosteroid doses, biopsy should be strongly considered.
7.3 Infectious Orbital Disease
7.3.1. ORBITAL CELLULITIS
Symptoms
Red eye, pain, blurred vision, double vision, eyelid swelling, nasal congestion/discharge, sinus headache/pressure/congestion, tooth pain, infra- and/or supraorbital pain, or hypesthesia.
Signs
(See Figures 7.3.1.1 and 7.3.1.2.)

FIGURE 7.3.1.1. Orbital cellulitis.

FIGURE 7.3.1.2. CT of right orbital cellulitis showing fat stranding and right ethmoiditis.
Critical. Eyelid edema, erythema, warmth, and tenderness. Conjunctival chemosis and injection, proptosis, and restricted ocular motility with pain on attempted eye movement are usually present. Signs of optic neuropathy (e.g., afferent pupillary defect, dyschromatopsia) may be present in severe cases.
Other. Decreased vision, retinal venous congestion, optic disc edema, purulent discharge, decreased periorbital sensation, fever. CT scan usually shows an adjacent sinusitis (typically an ethmoid sinusitis), possibly a subperiosteal orbital collection.
Differential Diagnosis
See 7.1, Orbital Disease.
Etiology
 Direct extension from a paranasal sinus infection (especially ethmoiditis), focal periorbital infection (e.g., dacryoadenitis, dacryocystitis, panophthalmitis), or dental infection.
Direct extension from a paranasal sinus infection (especially ethmoiditis), focal periorbital infection (e.g., dacryoadenitis, dacryocystitis, panophthalmitis), or dental infection.
 Sequela of orbital trauma (e.g., orbital fracture, penetrating trauma, retained intraorbital foreign body).
Sequela of orbital trauma (e.g., orbital fracture, penetrating trauma, retained intraorbital foreign body).
 Sequela of orbital surgery or paranasal sinus surgery.
Sequela of orbital surgery or paranasal sinus surgery.
 Sequela of other ocular surgery (less common).
Sequela of other ocular surgery (less common).
 Vascular extension (e.g., seeding from a systemic bacteremia or locally from facial cellulitis via venous anastomoses).
Vascular extension (e.g., seeding from a systemic bacteremia or locally from facial cellulitis via venous anastomoses).
 Secondary orbital venous stasis and inflammation from a septic cavernous sinus thrombosis.
Secondary orbital venous stasis and inflammation from a septic cavernous sinus thrombosis.
NOTE: In cases of unsuspected retained foreign body, cellulitis may develop months after injury (see 3.12, Intraorbital Foreign Body).
Organisms
 Adult: Staphylococcus species, Streptococcus species, Bacteroides.
Adult: Staphylococcus species, Streptococcus species, Bacteroides.
 Children: Haemophilus influenzae (rarely in vaccinated children).
Children: Haemophilus influenzae (rarely in vaccinated children).
 Following trauma: Gram-negative rods.
Following trauma: Gram-negative rods.
 Dental abscess: Mixed, aggressive aerobes and anaerobes.
Dental abscess: Mixed, aggressive aerobes and anaerobes.
 Immunocompromised patients (diabetes, chemotherapy, HIV infection): Fungi (Mucormycosis/Zygomycosis, Aspergillus).
Immunocompromised patients (diabetes, chemotherapy, HIV infection): Fungi (Mucormycosis/Zygomycosis, Aspergillus).
Work-Up
See 7.1, Orbital Disease, for a nonspecific orbital work-up.
1. History: Trauma or surgery? Ear, nose, throat, or systemic infection? Tooth pain or recent dental abscess? Stiff neck or mental status changes? Diabetes or an immunosuppressive illness?
2. Complete ophthalmic examination: Look for an afferent pupillary defect, limitation of or pain with eye movements, proptosis, increased resistance to retropulsion, elevated IOP, decreased color vision, decreased skin sensation, or an optic nerve or fundus abnormality.
3. Check vital signs, mental status, and neck flexibility.
4. CT scan of the orbits and paranasal sinuses (axial and coronal views, with contrast if possible) to confirm the diagnosis and to rule out a retained foreign body, orbital or subperiosteal abscess, paranasal sinus disease, or cavernous sinus thrombosis.
5. CBC with differential.
6. Blood cultures (especially helpful in pediatric cases).
7. Explore and debride any penetrating wound, if present, and obtain a Gram stain and culture of any drainage (e.g., blood and chocolate agars, Sabouraud dextrose agar, thioglycolate broth).
8. Consult Neurology or Neurosurgery for suspected meningitis for management and possible lumbar puncture. If paranasal sinusitis is present, consider consultation with Otorhinolaryngology for possible surgical drainage. Consider an Infectious Disease consultation in atypical, severe, or unresponsive cases. If a dental source is suspected, Oral Maxillofacial Surgery should be consulted for assessment, since infections from this area tend to be aggressive, potentially vision threatening, and may spread into the cavernous sinus.
NOTE: Mucormycosis/zygomycosis is an orbital, nasal, and sinus disease occurring in diabetic or otherwise immunocompromised patients. Typically associated with severe pain and external ophthalmoplegia. Profound visual loss may rapidly occur. Metabolic acidosis may be present. Sinoorbital mucormycosis/zygomycosis is rapidly progressive and life-threatening. See 10.10, Cavernous Sinus and Associated Syndromes (Multiple Ocular Motor Nerve Palsies).
Treatment
1. Admit the patient to the hospital and consider consultation with Infectious Disease and Otorhinolaryngology.
2. Broad-spectrum intravenous antibiotics to cover Gram-positive, Gram-negative, and anaerobic organisms are recommended for 48 to 72 hours, followed by oral medication for at least 1 week. The specific antibiotic agents vary. In patients from the community with no recent history of hospitalization, nursing home stay, or institutional stay, we currently recommend:
—Ampicillin-sulbactam 3 g i.v. q6h in adults; 300 mg/kg per day in four divided doses in children, maximum daily dose 12 g ampicillin-sulbactam (8 g ampicillin component).
or
—Piperacillin-tazobactam 4.5 g i.v. q8h or 3.375 g q6h in adults; 240 mg of piperacillin component/kg/day in three divided doses in children, maximum daily dose 18 g piperacillin.
 For adults who are allergic to penicillin but can tolerate cephalosporins, use vancomycin as dosed below plus:
For adults who are allergic to penicillin but can tolerate cephalosporins, use vancomycin as dosed below plus:
—Ceftriaxone 2 g i.v. q.d. and metronidazole 500 mg i.v. q6–8h (not to exceed 4 g per day).
 For adults who are allergic to penicillin/cephalosporin, treat with a combination of a fluoroquinolone (for patients >17 years of age, moxifloxacin 400 mg i.v. daily or ciprofloxacin 400 mg i.v. q12h or levofloxacin 750 mg i.v. q.d.) and metronidazole 500 mg i.v. q6–8h.
For adults who are allergic to penicillin/cephalosporin, treat with a combination of a fluoroquinolone (for patients >17 years of age, moxifloxacin 400 mg i.v. daily or ciprofloxacin 400 mg i.v. q12h or levofloxacin 750 mg i.v. q.d.) and metronidazole 500 mg i.v. q6–8h.
 Given the prevalence of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA), treatment with trimethoprim-sulfamethoxazole, tetracycline derivatives, vancomycin, or clindamycin may also be started initially. Some clinicians prefer to save these antibiotics and institute them only if the patient fails to improve or worsens over the first 48 hours of intravenous therapy. In patients suspected of harboring hospital-associated MRSA or in those suspected of meningitis, intravenous vancomycin is started at 15 mg/kg q12–24h in adults with normal renal function and 40 mg/kg per day in two or three divided doses in children, with a maximum daily dose of 2 g.
Given the prevalence of community-associated methicillin-resistant Staphylococcus aureus (CA-MRSA), treatment with trimethoprim-sulfamethoxazole, tetracycline derivatives, vancomycin, or clindamycin may also be started initially. Some clinicians prefer to save these antibiotics and institute them only if the patient fails to improve or worsens over the first 48 hours of intravenous therapy. In patients suspected of harboring hospital-associated MRSA or in those suspected of meningitis, intravenous vancomycin is started at 15 mg/kg q12–24h in adults with normal renal function and 40 mg/kg per day in two or three divided doses in children, with a maximum daily dose of 2 g.
NOTE: Antibiotic dosages may need to be reduced in the presence of renal insufficiency or failure. Peak and trough levels of vancomycin are usually monitored, and dosages are adjusted as needed. BUN and creatinine levels are monitored closely.
3. Nasal decongestant spray as needed for up to 3 days. Nasal corticosteroid spray may also be added to quicken the resolution of sinusitis.
4. Erythromycin ointment q.i.d. for corneal exposure and chemosis if needed.
5. If the orbit is tight, an optic neuropathy is present, or the IOP is severely elevated, immediate canthotomy/cantholysis may be needed. See 3.10, Traumatic Retrobulbar Hemorrhage, for technique.
6. The use of systemic corticosteroids in the management of orbital cellulitis remains controversial. If systemic corticosteroids are considered, it is probably safest to wait 24 to 48 hours until an adequate intravenous antibiotic load has been given (three to four doses).
Follow-Up
Reevaluate at least twice daily in the hospital for the first 48 hours. Severe infections may require multiple daily examinations. Clinical improvement may take 24 to 36 hours.
1. Progress is monitored by:
—Patient’s symptoms.
—Temperature and white blood cell count (WBC).
—Visual acuity and evaluation of optic nerve function.
—Ocular motility.
—Degree of proptosis and any displacement of the globe (significant displacement may indicate an abscess).
NOTE: If clinical deterioration is noted after an adequate antibiotic load (three to four doses), a CT scan of the orbit and brain with contrast should be repeated to look for abscess formation (see 7.3.2, Subperiosteal Abscess). If an abscess is found, surgical drainage may be required. Radiographic findings may lag behind the clinical examination, and so clinical deterioration itself may be an indication for surgical drainage. Other conditions that should be considered when the patient is not improving include cavernous sinus thrombosis, meningitis, or a noninfectious etiology.
2. Evaluate the cornea for signs of exposure.
3. Check IOP.
4. Examine the retina and optic nerve for signs of posterior compression (e.g., chorioretinal folds), inflammation, or exudative retinal detachment.
5. When orbital cellulitis is clearly and consistently improving, then the regimen can be changed to oral antibiotics (depending on the culture and sensitivity results) to complete a 10- to 14-day course. We often use:
—Amoxicillin/clavulanate: 25 to 45 mg/kg/day p.o. in two divided doses for children, maximum daily dose of 90 mg/kg/day; 875 mg p.o. q12h for adults.
or
—Cefpodoxime: 10 mg/kg/day p.o. in two divided doses for children, maximum daily dose of 400 mg; 200 mg p.o. q12h for adults.
Doxycycline or trimethoprim-sulfamethoxazole are also reasonable alternatives, especially if CA-MRSA is suspected.
The patient is examined every few days as an outpatient until the condition resolves and instructed to return immediately with worsening signs or symptoms.
NOTE: Medication noncompliance is an extremely common reason for recurrence or failure to improve. The oral antibiotic regimen should be individualized for ease of use and affordability. Effective generic alternatives include doxycycline and trimethoprim/sulfamethoxazole.
7.3.2. SUBPERIOSTEAL ABSCESS
Signs and Symptoms
Similar to orbital cellulitis, though may be magnified in scale. Suspect an abscess if a patient with orbital cellulitis fails to improve or deteriorates after 48 to 72 hours of intravenous antibiotics.
Differential Diagnosis
 Intraorbital abscess: Rare, because periosteum is an excellent barrier to intraorbital spread. May be seen following penetrating trauma, previous surgery, retained foreign body, extrascleral extension of endophthalmitis, extension of subperiosteal abscess (SPA), or from endogenous seeding. Treatment is surgical drainage and intravenous antibiotics. Drainage may be difficult because of several isolated loculations.
Intraorbital abscess: Rare, because periosteum is an excellent barrier to intraorbital spread. May be seen following penetrating trauma, previous surgery, retained foreign body, extrascleral extension of endophthalmitis, extension of subperiosteal abscess (SPA), or from endogenous seeding. Treatment is surgical drainage and intravenous antibiotics. Drainage may be difficult because of several isolated loculations.
 Cavernous sinus thrombosis: Rare in era of antibiotics. Most commonly seen with Mucormycosis/Zygomycosis [see 10.10, Cavernous Sinus and Associated Syndromes (Multple Ocular Motor Nerve Palsies)]. In bacterial cases, the patient is usually also septic and may be obtunded and hemodynamically unstable. Prognosis is guarded in all cases. Manage with hemodynamic support (usually in intensive care unit), broad-spectrum antibiotics, and surgical drainage if an infectious nidus is identified (e.g., paranasal sinuses, orbit). Anticoagulation can be considered.
Cavernous sinus thrombosis: Rare in era of antibiotics. Most commonly seen with Mucormycosis/Zygomycosis [see 10.10, Cavernous Sinus and Associated Syndromes (Multple Ocular Motor Nerve Palsies)]. In bacterial cases, the patient is usually also septic and may be obtunded and hemodynamically unstable. Prognosis is guarded in all cases. Manage with hemodynamic support (usually in intensive care unit), broad-spectrum antibiotics, and surgical drainage if an infectious nidus is identified (e.g., paranasal sinuses, orbit). Anticoagulation can be considered.
Work-Up
See 7.3.1, Orbital Cellulitis, for work-up. In addition:
1. Obtain CT with contrast, which allows for easier identification and extent of abscess. In cases of suspected cavernous sinus thrombosis, discuss with the radiologist before CT, since special CT techniques and windows may help with diagnosis. MRI may also be indicated.
NOTE: All orbital cellulitis patients who do not improve after 48 to 72 hours of intravenous antibiotic therapy should undergo repeat imaging.
Treatment
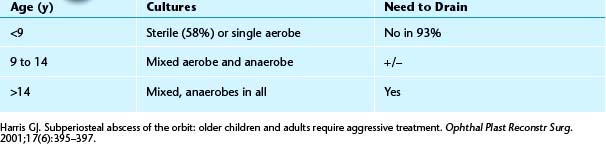
1. Microbes involved in SPA formation are related to the age of the patient. The causative microbes influence response to intravenous antibiotics and the need for surgical drainage. See Table 7.3.2.1.
TABLE 7.3.2.1 Age and Subperiosteal Abscess
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


