Oral manifestations of hematologic and nutritional deficiencies can affect the mucous membranes, teeth, periodontal tissues, salivary glands, and perioral skin. This article reviews common oral manifestations of hematologic conditions starting with disorders of the white blood cells including cyclic hematopoiesis (cyclic neutropenia), leukemias, lymphomas, plasma cell dyscrasias, and mast cell disorders; this is followed by a discussion of the impact of red blood cell disorders including anemias and less common red blood cell dyscrasias (sickle cell disease, hemochromatosis, and congenital erythropoietic porphyria) as well as thrombocytopenia. Several nutritional deficiencies exhibit oral manifestations. The authors specifically discuss the impact of water-soluble vitamins (B2, B3, B6, B9, B12, and C), fat-soluble vitamins (A, D, and K) and the eating disorders anorexia nervosa and bulimia nervosa on the oral mucosa.
Oral manifestations of hematologic and nutritional deficiencies can affect the mucous membranes, teeth, periodontal tissues, salivary glands, and perioral skin. In this article the authors review common oral manifestations of hematologic conditions starting with disorders of the white blood cells including cyclic hematopoiesis (cyclic neutropenia), leukemias, lymphomas, plasma cell dyscrasias, and mast cell disorders. This review is followed by a discussion of the impact of red blood cell disorders including anemias, and less common red blood cell dyscrasias (sickle cell disease, hemochromatosis, and congenital erythropoietic porphyria) as well as thrombocytopenia. Several nutritional deficiencies exhibit oral manifestations. The authors specifically discuss the impact of water-soluble vitamins (B2, B3, B6, B9, B12, and C), fat-soluble vitamins (A, D, and K), and the eating disorders anorexia nervosa and bulimia nervosa on the oral tissues.
Oral manifestations of hematologic diseases
Common and rare hematologic disorders may exhibit nonspecific as well as pathognomonic oral manifestations. Mechanisms of oral pathology may include direct infiltration by abnormal hematologic cells, deposition of abnormal proteins, oral ulceration, and abnormal hematopoiesis. All hematopoietic lineages may present with oral findings depending on the specific disorder.
White Blood Cell Disorders
Cyclic hematopoiesis
Neutrophils, or polymorphonuclear leukocytes (PMNs), are an integral part of the innate immune system against bacterial pathogens, and typically account for 50% to 70% of the circulating white blood cell population. Neutrophil activation releases myeloperoxidase, a heme protein that produces cytotoxic oxidants and affects nitric oxide–dependent signaling within the vascular endothelium. Cyclic hematopoiesis (previously termed cyclic neutropenia, Online Mendelian Inheritance in Man [OMIM] #162800) is a rare disorder characterized by periodic failure of hematopoietic progenitor cells resulting in dramatic oscillations in neutrophil, monocyte, eosinophil, platelet, and reticulocyte counts. Patients typically experience transient fever, oral ulcerations, and recurrent skin infections in conjunction with the neutropenia that occurs at intervals of 15 to 35 days (most commonly 21 days). Both the autosomal dominant form of the disease and sporadic cases are caused by a mutation in the gene for neutrophil elastase ( ELA2 , chromosome 19p13.3). These mutations disrupt granulopoiesis and induce apoptosis.
Cyclic hematopoiesis most commonly presents in infants and children, although adult onset may occur. In general, disease manifestations recede with age. Clinical presentation can vary in severity and tends to occur when the neutrophil count drops below 500 cells/μL. Systemic and extraoral manifestations include fever, lymphadenopathy, and skin and respiratory infections. The oral manifestations of cyclic hematopoiesis include recurrent aphthous stomatitis (RAS), recurrent gingivitis, and periodontitis. RAS is one of the most common presenting symptoms in cyclic hematopoiesis; RAS arises during the nadir and resolves spontaneously as the neutrophil count improves. The finding of RAS with or without periodontal disease, particularly in a child, should raise the suspicion of cyclic neutropenia.
Diagnostic evaluation entails serial measurement of circulating neutrophils. The diagnosis may be established by demonstrating at least 2 cycles of neutropenia. Treatment involves regular administration of recombinant granulocyte colony-stimulating factor (G-CSF), which can diminish the frequency and severity of symptoms.
Leukemias
The leukemias are malignancies of hematopoietic cells characterized by the proliferation of malignant leukocytes and destruction of the bone marrow. The neoplastic immature leukocytes (blast cells) appear in the peripheral blood, often resulting in an impressive leukocytosis. The leukemias are classified according to the progenitor cell involved (lymphoid or myeloid lineage) and whether the disease follows an acute or chronic course. Clinical manifestations of leukemia may result from loss of normal leukocyte function, suppression of hematopoietic cell lines, or direct infiltration of leukemic cells into tissues. Consequently, the signs and symptoms are varied and may include fatigue, anemia, lymphadenopathy, recurrent infection, bone and abdominal pain, bleeding, and purpura.
Leukemia cutis, infiltration of the skin by leukemic cells, presents as firm and rubbery papules, plaques, and nodules, and may precede development of systemic leukemia. Ulcers and blisters occur less commonly. Myelogenous leukemias may present as dermal nodules termed chloromas or granulocytic sarcomas. On sectioning and exposure to air, these nodules develop a blue-green color due to the presence of myeloperoxidase within the leukemic cells.
Oral manifestations may occur in any of the leukemias, but they are more prevalent in acute (vs chronic) and myeloid (vs lymphoid) leukemias. Oral examination of patients may reveal mucosal pallor due to anemia, or bleeding and petechiae of the palate, tongue, or lips as the result of underlying thrombocytopenia. Painful and deep oral ulcerations are common and may result from either neutropenia or direct infiltration by malignant cells. Patients may also develop severe viral, fungal, and bacterial oral infections as a consequence of immunosuppression.
Gingival hyperplasia results from leukemic infiltration of the gingivae. This infiltration is most common in the acute leukemias, particularly acute monocytic leukemia and acute promyelocytic leukemia. Patients typically present with moderately edematous, erythematous, and friable gingivae that may encroach on the teeth. Gingival hyperplasia often improves markedly following appropriate chemotherapy.
Lymphomas
Lymphomas are malignancies of lymphocytes and their precursor cells. These tumors develop in secondary lymphatic tissues, most commonly in the lymph nodes and less frequently in extranodal lymph tissues. One classification scheme differentiates Hodgkin lymphoma (HL) from non-Hodgkin lymphoma (NHL). HL predominantly affects adolescents and young adults with an additional prevalence peak in middle age. NHL typically presents in middle-aged to older individuals. Both HL and NHL occur more commonly in men.
Clinical manifestations are diverse but frequently include painless lymphadenopathy, hepatosplenomegaly, and secondary infections. The symptoms of fever, night sweats, and weight loss (B symptoms) as well as pruritus suggest advanced disease and a poor prognosis. The diagnosis is based on histologic and immunohistochemical findings in diseased tissue.
Oral manifestations of lymphoma are far more likely to occur in NHL, particularly Burkitt lymphoma and AIDS-associated B-cell lymphoma ( Fig. 1 ). In NHL, oral involvement preferentially affects the lymphoid tissues of Waldeyer’s ring as well as the vestibule and gingivae. Painless, soft masses, with or without traumatic ulceration, may also involve the palate, buccal mucosa, and gingivae. The clinical differential diagnosis includes minor salivary gland neoplasms, Kaposi sarcoma, and infections.

Burkitt lymphoma is an aggressive pediatric lymphoma that is commonly associated with oral manifestations. Epstein-Barr virus infection has been implicated in its pathogenesis. Burkitt lymphoma presents as a rapidly expanding mass causing bone and adjacent soft tissue destruction, resulting in painful loosening of the teeth; it more commonly affects the maxilla than the mandible.
AIDS-associated B-cell lymphoma is typically a non-Hodgkin B-cell lymphoma that presents as a papule, nodule, or tumor with or without ulceration; this entity typically affects Waldeyer’s ring or the gingivae (see Fig. 1 ). AIDS-associated lymphoma manifests when the CD4 count is less than 50/μL and portends a poor prognosis.
Amyloidosis
The amyloidoses are a group of disorders characterized by pathologic deposition of fibrillar proteins in various tissues. Amyloidosis is classified according to the type of protein produced and whether protein deposition is localized or systemic. Amyloidosis may be a primary disorder (AL amyloidosis), or it can be a secondary manifestation of neoplastic (ie, multiple myeloma) or chronic inflammatory (ie, rheumatoid arthritis, tuberculosis) disorders. AL amyloidosis is the most common systemic amyloidosis and the amyloidosis that most frequently affects the oral cavity. Localized amyloidosis may also produce oral lesions.
AL amyloidosis is characterized by systemic deposition of immunoglobulin light or heavy chains, which may occur as a primary disease process or as the sequela of multiple myeloma. Due to its extensive range of organ and tissue involvement, the clinical manifestations of the disease are numerous. Some signs and symptoms include fatigue, weight loss, edema, renal failure, autonomic and peripheral neuropathy, and rapidly evolving congestive heart failure due to a restrictive cardiomyopathy.
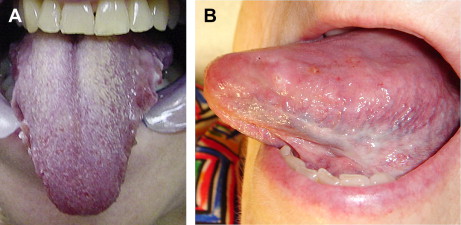
The oral manifestations of amyloidosis include macroglossia, edema, submucosal hemorrhage, glossodynia, taste disturbance, and xerostomia (due to destruction of salivary glands). Macroglossia is found in 20% of patients, making it the most widely documented oral finding; it is a distinctive feature of AL amyloidosis that is not typically found in the other systemic amyloidoses. Patients with macroglossia present with enlargement (localized nodular or diffuse) and/or woody induration of the tongue. Scalloping of the lateral tongue borders may result from counterpressure exerted by the teeth as the tongue enlarges ( Fig. 2 ). On occasion, macroglossia can be severe enough to compromise the airway and require surgical intervention. In some patients with AL amyloidosis, firm, yellowish nodules composed of amyloid may also occur on the gingivae, buccal mucosa, or palate.
Localized amyloidosis of the oral cavity is relatively rare, but patients typically present with one or more soft, red, yellow, purple, or blue nodules on the buccal mucosa, tongue, gingivae, or less commonly, the palate.
Dogma suggests that diagnostic biopsy should be obtained from the rectum. However, oral biopsies are easier to obtain, less traumatic, and of equal yield compared with rectal biopsies. Diagnosis of amyloidosis requires histologic examination and demonstration of extracellular amyloid deposits. Histologic specimens are stained with Congo red and examined with polarized microscopy for the characteristic apple-green birefringence. Depending on the type of amyloidosis suspected, additional immunohistochemical stains may include κ and λ light chain, β-amyloid A4 protein, transthyretin, and β2-microglobulin. Immunofixation electrophoresis of serum or urine may also be used to detect and characterize circulating proteins.
Multiple myeloma
Multiple myeloma (MM) is a malignant plasma cell dyscrasia that results in the overproduction of immunoglobulin light chains. MM typically presents in middle-aged and older adults, and is more prevalent in men and African Americans. Amyloidosis confers a poorer prognosis in patients with MM. The most common presenting symptom is bone pain caused by osteolytic lesions or pathologic fractures. However, patients may also present with hypercalcemia, proteinuria, renal failure, anemia, or thrombocytopenia. The radiographic finding of multiple “punched-out” bone lesions is highly suggestive of advanced MM. Up to 30% of patients have involvement of the mandible with associated swelling, pain, paresthesias, and tooth loss. Gingival bleeding or oral petechiae may be seen when marrow infiltration by malignant plasma cells causes thrombocytopenia. In rare instances, MM can produce extramedullary plasmacytomas. When located in the oral cavity, plasmacytomas are most commonly found on the gingivae or hard palate, and appear as dome-shaped nodules that have a tendency to ulcerate.
The diagnosis of MM requires evidence of end-organ damage (ie, lytic bone lesions, anemia, hypercalcemia, or renal insufficiency), bone marrow aspiration or biopsy to demonstrate plasma cell proliferation in the marrow, and the detection of monoclonal protein in the serum or urine. Treatment with cyclophosphamide and other chemotherapeutic agents may be associated with both cutaneous and oral mucosal manifestations that are beyond the scope of this article.
Langerhans cell histiocytosis
Formerly known as histiocytosis X, Langerhans cell histiocytosis (LCH) is a rare disorder of unknown etiology that encompasses several different clinical entities involving the proliferation of Langerhans cells. The disease is characterized by destructive tissue infiltration by abnormal histiocytes mixed with lymphocytes and eosinophils. LCH has a broad spectrum of clinical manifestations depending on the site and extent of organ involvement. Some patients have mild, localized pain caused by isolated bone lesions, whereas others develop rapidly progressive systemic disease involving nearly every organ system. Definitive diagnosis of LCH requires histologic confirmation.
Ten percent to 20% of patients have lytic lesions of the maxilla or mandible, resulting in edema and ulceration of the overlying mucosa, gingival inflammation, necrosis, and recession as well as increased tooth mobility and premature tooth loss. Radiographic findings include localized osteolytic lesions, pathologic fractures, “floating teeth” in which the teeth appear to “float” within the radiographic lucency, and premature tooth loss. Ulceration of the oral mucosa in the absence of underlying bone lesions rarely occurs. These painful ulcers are most commonly located on the buccal mucosa or the posterior vestibule. Evaluation of the patient with LCH should include whole-body radiographic skeletal survey or bone scintigraphy, and serum studies to assess for diabetes insipidus and hypercalcemia.
Systemic mastocytosis
Mastocytosis encompasses several distinct clinical entities characterized by abnormal proliferation of mast cells. Most cases of mastocytosis exclusively involve the skin, but systemic disease is characterized by involvement of bone marrow and other organs. Typical symptoms of mastocytosis are related to release of mast cell mediators, including histamine and various vasoactive factors. Consequently, clinical manifestations include urticaria, flushing, pruritus, diarrhea, palpitations, and syncope. In systemic mastocytosis, patients may present with bone pain, osteoporosis, lymphadenopathy, hepatosplenomegaly, and neuropsychiatric disturbances.
Oral manifestations of systemic mastocytosis are rare. However, painful osteolytic lesions of the mandible or maxilla have been reported, and they may be associated with ulceration and sinus tract formation. Mast cell infiltration of the salivary and lacrimal glands may lead to the sicca syndrome, characterized by excessive dryness of the mouth and eyes.
Systemic mastocytosis is defined by major and minor criteria: the major criterion is the presence of dense mast cell infiltrates in the bone marrow or extracutaneous organs, and the minor criteria include (1) presence of 25% abnormal or spindle-shaped mast cells on bone marrow aspirate or tissue biopsy, (2) c-Kit mutation at codon 816V, (3) expression of CD2 and/or CD25 on CD117+ mast cells, and (4) total serum tryptase levels persistently greater than 20 ng/mL. The diagnosis requires evidence of either the major criterion and one minor criterion, or 3 minor criteria.
Red Blood Cell Disorders
Anemia, regardless of cause, is associated with pallor, fatigue, dyspnea, tachycardia, glossitis, glossodynia, and stomatitis. In anemia due to deficiency of iron, folate, or vitamin B12, the oral findings may be the initial presentation, and may precede a decrease in hemoglobin or change in mean corpuscular volume.
Iron-deficiency anemia
Iron-deficiency anemia, the most common cause of anemia worldwide, may result from insufficient dietary intake or malabsorption of iron, chronic blood loss, hemolysis, and pregnancy. As in other anemias, iron deficiency presents with pallor, fatigue, dyspnea, tachycardia, and telogen effluvium. Iron-deficiency anemia tends to produce nail findings such as splitting or spooning (koilonychia).
The most common oral manifestation of iron-deficiency anemia is mucosal pallor, most notable on the gingivae and vermilion lips. Angular cheilitis and atrophic glossitis (loss of filiform and fungiform papillae of the tongue, causing the tongue to appear smooth and red) are also important diagnostic clues. This atrophic glossitis may be preceded by glossodynia, burning sensation, or dysphagia. Epidemiologic studies show variable association between iron deficiency and RAS, and repletion of iron stores may not affect the clinical course of RAS. Iron deficiency is a predisposing factor for oral candidiasis.
The combination of iron deficiency anemia, dysphagia, and esophageal strictures or webs comprises the Plummer-Vinson syndrome. This disorder is now rare but was previously found in middle-aged women with glossitis, glossodynia, angular cheilitis, and koilonychia. Plummer-Vinson syndrome is associated with an increased risk of oral and pharyngeal carcinoma.
A diagnosis of iron-deficiency anemia is suggested by the finding of microcytic, hypochromic anemia in conjunction with decreased serum iron (<60 μg/dL), decreased serum ferritin (<15 μg/dL), and elevated total iron-binding capacity (>400 μg/dL). In men and postmenopausal women, the diagnosis of iron deficiency anemia should prompt further investigation for possible gastrointestinal bleeding.
Megaloblastic anemia
Megaloblastic anemia is a consequence of defective DNA synthesis during erythropoiesis and most commonly results from vitamin B12 (cobalamin, cyanocobalamin) or folate deficiency. Potential causes of folate deficiency include inadequate dietary intake, malabsorption, or increased folate consumption that may occur during pregnancy, periods of rapid growth, or chronic inflammation. Vitamin B12 deficiency is less common but may be seen in the elderly, vegetarians, and patients with pernicious anemia, human immunodeficiency virus, or gastrointestinal disease. In addition to the usual clinical manifestations of anemia, vitamin B12 deficiency may cause neuropsychiatric findings such as ataxia, loss of vibratory sensation, dementia, or psychosis.
Megaloblastic anemia frequently causes atrophy of oral mucosa exhibited by glossitis and angular cheilitis. The tongue may be painful, and patients may note alterations in taste sensation. The tongue may be beefy red, and occasionally erythematous patches can be found on the buccal mucosa as well. Folate and vitamin B12 deficiencies have also been implicated as contributing factors to RAS, and in some patients aphthae will improve following folate and vitamin B12 repletion. The diagnosis of vitamin B12 deficiency can be distinguished from folate deficiency by direct measurement of serum vitamin B12 levels or the detection of elevated serum methylmalonic acid.
Sickle cell disease
Sickle cell disease (SCD) is an autosomal recessive disorder in which a hemoglobin mutation predisposes erythrocytes to deformation in the setting of low oxygen tension. The clinical manifestations of SCD are diverse, and may result from vaso-occlusion and infarction of tissues, hemolysis, or increased susceptibility to bacterial infection. In general, patients with SCD are at increased risk of osteomyelitis, which is thought to result from repetitive bone infarction providing a favorable environment for bacterial growth. Acute pain in the long bones, chest, or abdomen, fever, malaise, numbness, weakness and altered cognition may signify an acute sickle crisis.
The most common oral manifestations of SCD are pallor or jaundice of the oral mucosa due to hemolysis. The soft palate or floor of the mouth may be the most sensitive areas for detecting jaundice. Osteomyelitis of the mandible is a rare complication. Infarction of branches of the mandibular nerve, due to vaso-occlusion, rarely causes persistent anesthesia of the teeth, gingivae, or oral mucosa. In addition, SCD patients may develop sudden onset of pain or necrosis in previously healthy teeth. The definitive diagnosis of SCD requires demonstration of hemoglobin S by hemoglobin electrophoresis.
Hemochromatosis
Hereditary hemochromatosis is an autosomal recessive disease caused by increased gastrointestinal absorption of iron in the gut resulting in systemic iron overload. This genetic disorder is most often caused by mutation in the HFE gene (6p21.3, OMIM #235200), but mutation in the hemojuvelin gen ( HJV , 1q21) has also been described. Hereditary hemochromatosis is characterized by the deposition of hemosiderin pigment in various tissues, which if left untreated may lead to diabetes mellitus, cirrhosis, heart failure, joint disease (preferentially affecting the second and third metacarpophalangeal joints), gonadal dysfunction, amenorrhea, and generalized bronze cutaneous hyperpigmentation.
The primary oral manifestation of hereditary hemochromatosis, or any state of iron overload, is blue-gray to brown hyperpigmentation that most commonly affects the palate, buccal mucosa, and gingivae. This oral pigmentation, however, is seen in a minority of patients with hereditary hemochromatosis. When stained with Prussian blue, biopsy specimens may demonstrate iron deposits.
The diagnosis of hereditary hemochromatosis requires measurement of serum ferritin and transferrin saturation. Serum ferritin levels greater than 200 μg/L in premenopausal women and 300 μg/L in men and postmenopausal women indicate iron overload due to hemochromatosis. Transferrin saturation refers to the ratio of serum iron and total iron-binding capacity, and is more sensitive than serum ferritin as a screening tool for hemochromatosis. A fasting transferrin saturation greater than 45% to 50% is diagnostic for hemochromatosis. Genetic testing for HFE mutations should be considered in patients with laboratory or histologic evidence of iron overload, especially in the context of liver disease. Treatment consists of serial phlebotomy, and chelation therapy may also be indicated.
Congenital erythropoietic porphyria
Porphyrias are a heterogeneous group of genetic metabolic disorders involving disruption of the heme biosynthetic pathway. Porphyrias are categorized based on the enzymatic defect and organ systems affected. Congenital erythropoietic porphyria (CEP, OMIM #263700, also known as Gunther disease) is a very rare autosomal recessive disorder caused by a deficiency of uroporphyrinogen III synthase ( UROS gene, 10q25.2-q26.3). High amounts of uroporphyrin accumulate in all tissues and when concentrated in erythrocytes, osmotic fragility results in hemolysis. Hemolytic anemia may present as early as in utero, potentially resulting in hydrops fetalis or intrauterine fetal demise. Porphyrins deposited in bone impart orange-red fluorescence and result in severe bone loss, osteopenia, and acro-osteolysis. Pink to red discoloration of the urine is pathognomonic; pink staining of the diapers in infancy may be the initial presenting sign. Mucocutaneous manifestations are common, and the disease can have devastating sequelae.
CEP typically presents in infancy or early childhood with severe photosensitivity leading to burning, blistering, erosions, hyperpigmentation, milia, and scarring of sun-exposed skin. Mutilation deformity of the face and hands with syndactyly (mitten deformity) is notable. Hypertrichosis of the face and extremities is common; the pathogenesis of this clinical manifestation is not known. Porphyrin deposition also affects the conjunctiva and manifests as conjunctivitis, blepharitis, and scarring with ectropion. Corneal scarring with eventual blindness may occur.
A pathognomonic oral manifestation of CEP is erythrodontia, a condition in which the teeth develop a red-brown discoloration and bright red fluorescence on Wood’s lamp examination ( Fig. 3 ). This unusual finding is thought to result from increased binding of porphyrin to calcium phosphate in dentin and enamel. Erythrodontia is not observed in other porphyrias.

Treatment includes strict avoidance of sun exposure and use of ocular lubricants. Red blood cell transfusion and bone marrow transplantation have been reported to be successful.
Platelet Disorders
Thrombocytopenia
A reduction in platelet number or function can occur through a variety of mechanisms, including autoimmune destruction (including connective tissue disease), splenic sequestration, bone marrow infiltration by tumor cells, infection (eg, infectious mononucleosis), and adverse drug reaction. Regardless of the cause, platelet disorders typically manifest with petechiae, purpura, and bleeding of the mucous membranes. Other presentations include epistaxis, hematuria, gastrointestinal bleeding, and on rare occasion, intracranial hemorrhage.
Gingival bleeding, either spontaneous or in response to minor trauma (ie, toothbrushing, flossing), is often the first sign of thrombocytopenia. The oral mucosa, most notably soft palate and buccal mucosa, may demonstrate petechiae and ecchymoses. Deep red to black hemorrhagic bullae may occur with very low platelet counts.
Oral manifestations of nutritional diseases
Vitamins and minerals are organic and inorganic substances, respectively, that are required for the health and function of epithelia including skin and mucous membranes. Nutritional deficiencies of vitamins and minerals can result from reduced intake, impaired absorption, or increased use (relative to the amount consumed). In economically disadvantaged communities, inadequate dietary consumption accounts for the majority of nutrient deficiencies. Eating disorders, fad diets, debilitated states, and alcoholism can also result in inadequate consumption of vitamins and minerals. Nutrient intake correlates with the number of posterior occluding pairs of natural teeth that an individual possesses. Edentulous adults have been shown to have lower levels of retinol, β-carotene, ascorbate, tocopherol, and folic acid than dentate adults.
The rate of epithelial cell turnover of the oral mucous membranes is much more rapid than that of skin (3–7 days vs up to 28 days ). As a result, the oral cavity often demonstrates early signs and symptoms of metabolic alteration resulting from systemic diseases, medications, or nutritional deficiencies. Repetitive exposures and trauma that occur with normal daily activities (ie, eating, breathing, talking) may augment the impact of nutritional deficiencies on mucous membrane integrity. Oral commensal microflora and pathologic microorganisms can further challenge weakened mucous membranes.
Water-soluble vitamins that have a role in the health and normal function of the oral mucosa, and therefore exhibit oral manifestations when deficient, include vitamins B2 (riboflavin), B3 (niacin), B6 (pyridoxine), B9 (folic acid), B12 (cobalamin), and C. Water-soluble vitamins are not stored in the body in large amounts and therefore must be obtained through dietary or supplement sources on a regular and frequent basis. The lack of large body stores effectively prevents hypervitaminoses of water-soluble vitamins. By contrast, significant physiologic reservoirs of fat-soluble vitamins preclude the need for daily consumption but also predispose to potential toxicity. Fat-soluble vitamins that affect the oral mucosa include vitamins A, D, and K.
Water-Soluble Vitamins
Vitamin B1 (thiamine, thiamin, aneurin)
Vitamin B1 was the first B vitamin discovered. Vitamin B1 facilitates the conversion of carbohydrates to glucose and the intracellular metabolism of fats and proteins. Dietary sources of vitamin B1 include yeast, wheat germ, whole-grain or enriched cereals, legumes, liver and other organ meats, lean meats (especially pork), blackstrap molasses, and soybeans. Vitamin B1 is easily destroyed on exposure to heat. Vitamin B1 is absorbed by the small intestine (predominantly the jejunum and ileum) through both passive and active transport mechanisms. The half-life of thiamine is 9 to 18 days, and thiamine stores become depleted within 1 month. Risk factors for vitamin B1 deficiency include alcoholism (which interferes with thiamine absorption), gastrointestinal disease (including prolonged diarrhea), renal dialysis, hyperemesis gravidarum, hyperthyroidism, lactation, diabetes mellitus, parenteral nutrition, anorexia nervosa, and a diet consisting predominantly of polished rice. Thiamine deficiency results in beriberi and Wernicke-Korsakoff syndrome, neither of which have oral manifestations.
Vitamin B2 (riboflavin, lactoflavin)
Vitamin B2 is part of the coenzymes flavin mononucleotide (FMN) and flavin adenine dinucleotide (FAD), which aid enzymes in several intracellular metabolic oxidation/reduction reactions involved in cellular metabolism, the processing of carbohydrates, amino acids, and fats, and the regeneration of the free radical scavenger glutathione. Riboflavin is found in milk, other dairy products, and dietary sources that contain significant amounts of vitamin B1. Unlike vitamin B1, however, vitamin B2 is heat-stable. Vitamin B2 is absorbed primarily in the proximal small bowel. Risk factors for vitamin B2 deficiency include alcoholism, gastrointestinal disease (ie, achlorhydria, malabsorption, diarrhea, and so forth), chlorpromazine use (due to increased excretion of riboflavin), and other nutrient deficiencies (ie, zinc, vitamin B3). Vitamin B2 deficiency is usually seen as a component of mixed B vitamin deficiency and classically manifests as the oculo-oro-genital syndrome. Patients with this triad present with conjunctivitis, photophobia, and pruritic or burning, erythematous, scaling patches involving the genitalia (scrotum, penis, vulva) and perianal skin that may progress to superficial ulceration. Oral manifestations include erythema of the pharyngeal and oral mucous membranes, atrophic glossitis with a magenta color, glossodynia, cheilosis, and angular cheilitis.
The diagnosis of riboflavin deficiency is made clinically but may be assisted by the detection of an increased activation coefficient for red blood cell glutathione reductase activity. Rapid amelioration of signs and symptoms on administration of vitamin B2 (1–3 mg/d for children, 10–20 mg/d for adults) confirms the diagnosis.
Vitamin B3 (niacin, nicotinic acid)
Vitamin B3 and its amide form, niacinamide (nicotinamide), are required for normal cell function and metabolism. The amide derivatives, nicotinamide adenine dinucleotide (NAD) and nicotinamide adenine dinucleotide phosphate (NADP), play vital roles in pyridoxine nucleotide (cytosine, thymidine) synthesis, oxidation/reduction reactions involved in carbohydrate, amino acid, glycerol, and fatty acid metabolism, and adenine triphosphate (ATP) production. Sources of niacin include yeast, meats (eg, liver, lean pork, salmon, and poultry), cereals, legumes, and seeds. Niacin and niacinamide are absorbed through the intestinal epithelium via simple diffusion. Niacin is also produced de novo from tryptophan with the assistance of vitamin and mineral cofactors (vitamin B2, vitamin B6, copper, and iron). Predisposing factors for the development of vitamin B3 deficiency include alcoholism, gastrointestinal disease, consumption of a corn-dominant diet, drug therapy (ie, isoniazid, 5-fluorouracil, 6-mercaptopurine, and sulfapyridine), congenital defects of tryptophan transport in the intestine and/or kidneys (eg, Hartnup disorder, OMIM #234500), and carcinoid syndrome in which tryptophan is converted preferentially to serotonin instead of niacin.
Niacin deficiency, termed pellagra, exhibits diarrhea, photodistributed dermatitis, and dementia; death may occur. Early symptoms include malaise, apathy, and weakness. Gastrointestinal involvement may precede other organ systems and presents with nausea, abdominal pain, and diarrhea (typically watery, but bloody and mucoid may also be seen) with malabsorption. Initial cutaneous findings include erythema and edema accompanied by a burning sensation, with or without blisters (much like acute sunburn) symmetrically distributed at areas of sun exposure and/or trauma. Over time, progressive brittle scaling, lichenification, and hyperpigmentation of skin lesions occur. Neurologic symptoms may include paresthesias and muscle weakness with ataxia. Mental status changes, including apathy, depression, irritability, and poor concentration occur early in the course of disease and can progress to disorientation, delirium, and coma. Within the oral cavity, niacin deficiency exhibits mucosal edema, cheilosis, angular cheilitis, bright red glossitis, burning mouth, gingival erythema, and dental caries.
Low serum levels of niacin, tryptophan, NAD, and NADP confirm the diagnosis of pellagra. Measurement of urinary niacin metabolites (eg, N- methylnicotinamide) may be more sensitive than measurement of serum NAD and NADP levels. Oral administration of niacinamide (for adults, 100 mg every 6 hours until resolution of major acute symptoms followed by 50 mg every 8–12 hours until the skin normalizes; for children, 10–50 mg every 6 hours until disease resolution) effectively reverses the clinical signs and symptoms of pellagra. Patients with pellagra often suffer from other nutritional deficiencies mandating provision of a high-protein diet and B-complex vitamin supplementation.
Vitamin B5 (pantothenic acid)
Vitamin B5 is a component of coenzyme A and therefore plays an instrumental role in many cellular metabolic processes including fatty acid metabolism, cholesterol synthesis, and amino acid degradation. Key sources of pantothenic acid include meat (ie, beef, chicken, liver), eggs, tomatoes, broccoli, potatoes, and whole grains. Pantothenic acid deficiency is rare due to its wide presence in foods and large body stores. Symptoms of vitamin B5 deficiency include numbness and burning paresthesias of the feet. Pantothenic acid deficiency does not exhibit oral manifestations.
Vitamin B6 (pyridoxine, pyridoxal, pyridoxamine)
Vitamin B6 has various forms and is involved in gluconeogenesis, amino acid decarboxylation, fatty acid metabolism, heme biosynthesis, and neurotransmitter synthesis. As noted previously, vitamin B6 is an important cofactor in the conversion of tryptophan to niacin. Sources of vitamin B6 include meat, fish, eggs, milk, whole grains, vegetables, and nuts. Intestinal absorption of vitamin B6 occurs in the proximal jejunum. Advanced age, alcoholism, chronic renal failure and/or renal dialysis, liver disease, malnutrition, and intestinal malabsorption predispose to vitamin B6 deficiency. Increased pyridoxine requirements occur during pregnancy and lactation. Administration of isoniazid, d -penicillamine, hydralazine, l -dopa, or cycloserine may precipitate pyridoxine deficiency.
Pyridoxine deficiency presents with weakness, dizziness, and fatigue resulting from the associated anemia. Bilateral distal extremity numbness followed by burning paresthesia with impaired proprioception and vibration, depression, confusion, and generalized seizures may also occur. Patients may experience anorexia, nausea, abdominal discomfort, and diarrhea. Examination may reveal a scaling, erythematous eruption, similar to seborrheic dermatitis, around the eyes, nose, and mouth. Oral manifestations include atrophic glossitis, cheilosis, angular stomatitis, and gingival erythema.
Low plasma pyridoxal-5-phosphate levels confirm vitamin B6 deficiency. Pyridoxine replacement, the dose and administration route of which depend on the disease severity and underlying etiology, results in improvement over days to weeks. Secondary B vitamin deficiencies (eg, niacin) may result from pyridoxine deficiency, and the patient’s comprehensive nutritional needs should be addressed.
Vitamin B7 (biotin, vitamin H)
Vitamin B7 is an essential cofactor for carboxylases involved in fatty acid synthesis, gluconeogenesis, and amino acid catabolism. Dietary sources of biotin include cooked egg yolks, sardines, nuts (almonds, peanuts, pecans, walnuts), and legumes. Inadequate dietary intake rarely causes biotin deficiency. Prolonged consumption of raw egg white, parenteral nutrition without biotin supplementation, and biotinidase deficiency (OMIM #253260) cause biotin deficiency. In addition, long-term anticonvulsant therapy can deplete biotin stores.
Neurologic symptoms include depression, hallucination, ataxia, and peripheral paresthesias. In infancy, hypotonia, lethargy, and developmental delay may occur. Biotin deficiency presents with alopecia, conjunctivitis, and periorificial dermatitis with erythema and fine scaling around the eyes, nose, mouth, genitalia, and anus. Biotin deficiency does not cause oral mucous membrane pathology.
Vitamin B9 (folic acid, folate)
Vitamin B9 is reduced by dihydrofolate reductase to the biologically active form, tetrahydrofolate (tetrahydrofolic acid). Tetrahydrofolate plays an integral role in the synthesis of purines, thymidine, and amino acids and therefore affects DNA, RNA, and protein production and cell division. As such, folate deficiency preferentially affects tissues with rapid rates of cell turnover and high DNA synthesis requirements (ie, bone marrow, gastrointestinal epithelium, and mucosa).
Folate is widely distributed among food groups but is found in significant amounts in green leafy vegetables (eg, spinach), yeast, legumes (eg, lima and kidney beans), peanuts, organ meats (eg, liver, kidney), and dairy products. Food preparation and cooking (eg, boiling) can significantly reduce folate content. Folate is absorbed in the proximal jejunum through both active and passive transport. Risk factors for vitamin B9 deficiency include low socioeconomic status, infancy and prematurity, advanced age, institutionalization, alcoholism, malnutrition, and gastrointestinal diseases (ie, celiac disease and inflammatory bowel disease) with resulting malabsorption, as well as pregnancy, lactation, and chronic hemolytic anemia (due to increased demand). Methotrexate, sulfasalazine, and valproic acid interfere with folate metabolism. Increased excretion of folate occurs in the context of vitamin B12 deficiency.
Folate deficiency results in megaloblastic anemia with or without thrombocytopenia and leukopenia as well as gastrointestinal and neurologic disturbances. Anorexia, abdominal pain, nausea, vomiting, and diarrhea are common. Neurologic sequelae include confusion, peripheral neuropathy, and seizures. Folate deficiency results in elevated serum homocysteine levels and predisposes to atherosclerosis. During pregnancy, folate deficiency may result in spontaneous abortion, placental abruption, and congenital neural tube defects. Oral findings include atrophic glossitis with erythema and swelling of the tongue and angular cheilitis. Patients may also report tongue soreness or burning and dysphagia.
Folate administration in the context of vitamin B12 deficiency can result in significant neurologic deterioration; therefore, patients with megaloblastic anemia should be evaluated with measurement of both serum folate and vitamin B12 levels. Folate supplementation corrects folate deficiency and prevents complications.
Vitamin B12 (cobalamin, cyanocobalamin)
Vitamin B12 is an important cofactor required for DNA synthesis. Dietary sources of vitamin B12 include milk, cobalamin-fortified cereals, eggs, and meat; plants have little cobalamin content. Ingested cobalamin in food is liberated by pepsin digestion in the gastric acidic milieu. Cobalamin is then bound by intrinsic factor (IF), a glycoprotein produced by gastric parietal cells. The IF-cobalamin complex eventually binds to and is internalized with the IF receptor on the epithelial cells of the duodenum and ileum. Intestinal cobalamin absorption also occurs less efficiently via passive diffusion. The elderly, strict vegetarians or vegans, and those who have undergone gastric or ileal resection are particularly susceptible to vitamin B12 deficiency. Pernicious anemia, the most common form of vitamin B12 deficiency, is caused by autoantibodies against IF and/or gastric parietal cells and appears to have a genetic predisposition. Large body stores, half of which are located in the liver, delay clinical manifestations of cobalamin deficiency by 2 to 5 years.
Vitamin B12 deficiency results in megaloblastic anemia, which is indistinguishable from that of folate deficiency. Neurologic sequelae of cobalamin deficiency involve the brain, spinal cord (posterior and lateral columns), and peripheral and optic nerves. Symptoms include ascending numbness or paresthesias that begin in the distal extremities, ataxia and gait difficulties, limb weakness, and psychiatric and cognitive disturbances. Deficiency of cobalamin manifests orally as generalized stomatitis, taste disturbance, and a red, atrophic, beefy, burning tongue in which the loss of filiform papillae imparts a “bald” appearance. Oral changes may occur in the absence of symptomatic anemia. Folate and vitamin B12 deficiencies have been implicated in RAS, with improvement of some patients’ aphthae following repletion.
The diagnosis of vitamin B12 deficiency is made when megaloblasts and hypersegmented neutrophils are noted on peripheral blood smear in the context of a low serum vitamin B12 level. Detection of either antiparietal cell antibodies or antibodies to IF confirms the diagnosis of pernicious anemia. In the absence of these autoantibodies, elevated serum gastrin levels demonstrate achlorhydria and suggest pernicious anemia. If the aforementioned laboratory evaluation is unrevealing, the Schilling test can be used to determine the etiology of cobalamin deficiency. Depending on the pathogenesis of cobalamin deficiency, parenteral or oral cyanocobalamin administration can correct the hematologic, neurologic, and mucocutaneous abnormalities. Patients should be evaluated and treated for additional nutritional deficiencies, specifically folate. Patients with pernicious anemia exhibit increased risk of gastric carcinoma and carcinoid tumors, and should undergo close surveillance.
Vitamin C (ascorbic acid, l -ascorbic acid, ascorbate)
Vitamin C is a cofactor for norepinephrine synthesis, amidation of peptide hormones, carnitine biosynthesis, and tyrosine metabolism. Vitamin C is also an essential cofactor for prolyl hydroxylase and lysyl hydroxylase, and therefore plays an integral role in collagen formation. Vitamin C participates in redox reactions and acts as an antioxidant. Vitamin C also enhances the absorption of iron in the small intestine. Humans are unable to synthesize ascorbic acid. Excellent dietary sources of vitamin C include citrus fruits, broccoli, tomatoes, green peppers, and cabbage. Vitamin C levels are depleted after 30 days if no exogenous vitamin C is consumed. Risk factors for vitamin C deficiency include male gender, low dietary intake, and tobacco smoking (which reduces absorption and accelerates degradation of vitamin C). Additional predisposing conditions include advanced age, alcoholism, low socioeconomic status, small bowel diseases, and chronic diarrhea. Pregnancy, lactation, type 1 diabetes mellitus, and hemodialysis exhibit increased demands for vitamin C.
Early signs of vitamin C deficiency include lethargy and malaise. Shortness of breath, myalgias, and arthralgias also occur. Due to its essential role in collagen synthesis, vitamin C deficiency results in poor wound healing, dehiscence of established scars, and bony abnormalities. Capillary fragility manifests as perifollicular petechiae (most notable on the lower extremities and buttocks), generalized ecchymosis, and subperiosteal, retrobulbar, subarachnoid, and intracerebral hemorrhages. Capillary fragility may be demonstrated at the bedside using the Rumpel-Leede test (capillary fragility test, tourniquet test). Advanced scurvy presents with anemia, convulsions, neuropathy, jaundice (secondary to hemolysis), oliguria, and generalized edema, and may be fatal. Cutaneous findings include roughness and scaling with follicular accentuation, corkscrew hairs, and alopecia. Intraoral manifestations include mucosal petechiae, swollen and blue or red gingivae (hemorrhagic gingivitis), gingival bleeding, gingival hypertrophy, and interdental infarcts. Loss of connective tissue and alveolar bone result in loosening and loss of the teeth. Low dietary vitamin C intake confers an increased risk of 20% for developing periodontal disease.
Symptoms of deficiency manifest at a vitamin C level of less than 2.5 mg/dL. Oral vitamin C (100 mg 3 times daily) results in rapid improvement; intestinal absorption is limited to 100 mg at a time. Parenteral administration should be used in patients with malabsorption. Prompt diagnosis and treatment can reverse signs and symptoms and prevent permanent sequelae.
Fat-Soluble Vitamins
Vitamin A (retinol)
Vitamin A encompasses a family of fat-soluble vitamins that include retinol (preformed vitamin A, obtained from animal sources), β-carotene (provitamin A, obtained from plant sources), and carotenoids. Retinol is the most biologically active form. Vitamin A plays an important role in epithelial integrity, vision, immune response, and reproduction as well as the growth and modeling of bones and teeth. Rich sources of vitamin A include liver, cod liver oil, eggs, whole milk, and yellow-green leafy vegetables. Vitamin A is absorbed throughout the intestine and is stored in the liver (50%–80% of total body stores), lungs, kidneys, and adipose tissue. The bioavailability of vitamin A from animal sources is greater than that from plant sources. Predisposing conditions for vitamin A deficiency include malnutrition, alcoholism, fat malabsorption disorders, small bowel bypass surgery, impaired biliary or pancreatic secretions, and a vegan diet. Ethanol consumption inhibits the biochemical processing of retinol.
Vitamin A deficiency is associated with impaired cellular and humoral immunity as well as ocular, cutaneous, and mucosal changes. Xerophthalmia, abnormal keratinization of the cornea, nyctalopia (poor adaption to darkness), and blindness may result. Follicular hyperkeratosis (phrynoderma, toadskin ), diffuse dryness and scaling, and wrinkling are typical cutaneous findings. Oral manifestations of vitamin A deficiency include xerostomia, periodontal disease, and increased rates of intraoral infection. In infants and children with vitamin A deficiency, impaired tooth development is noted. Laboratory evaluation of persons with suspected vitamin A deficiency should include serum retinol level, zinc level, iron studies (as low iron may worsen vitamin A deficiency), and complete blood count (to assess for anemia or infection). Treatment requires vitamin A supplementation, the dose of which varies with deficiency severity, and remediation of underlying contributing factors.
The large stores of vitamin A in conjunction with the body’s inability to catabolize vitamin A predispose to potential toxicity. Hypervitaminosis A may be acute or chronic and occur in the setting of food fads (ie, excessive consumption of liver) and accidental overdose (carotenemia or other vitamin A ingestion). Clinical manifestations exhibit dose-dependent severity and include headache, anorexia, nausea, abdominal pain, myalgias, bone and joint pain, and irritability. Hepatic dysfunction and reduced bone mineral density may result. Women of reproductive age are at risk for retinoid embryopathy (hydrocephalus, central nervous system abnormalities, cerebellar malformation, microphthalmia, microtia/anotia, micrognathia, cleft palate, cardiac defects, hypoplastic or absent thymus) if toxicity occurs early in pregnancy. Generalized dryness of the skin and mucous membranes (conjunctivae, nasal mucosa) is characteristic. Oral manifestations of vitamin A toxicity include cheilitis, gingivitis, and impaired healing. Carotenemia (excessive consumption of β-carotene) manifests as yellow-orange discoloration of the skin; the sclera and oral mucous membranes, however, are not affected. Treatment of vitamin A intoxication includes discontinuation of vitamin A consumption and supportive care; signs and symptoms typically improve over several weeks.
Vitamin D (calciferol, cholecalciferol, ergocalciferol)
Vitamin D regulates calcium and phosphorus homeostasis via intestinal absorption and bone deposition and resorption. Ultraviolet B radiation (290–320 nm) transforms provitamin D 3 in the epidermis and dermis to previtamin D 3 , which is then isomerized to vitamin D 3 (cholecalciferol). Alternatively, vitamin D 3 (cholecalciferol) and vitamin D 2 (ergocalciferol) may be absorbed from dietary sources. Vitamin D (which includes vitamin D 3 and vitamin D 2 ) must be sequentially hydroxylated in the liver and kidneys to be biologically active. Dietary sources of vitamin D are somewhat limited and include fish liver oils (ie, cod liver oil), fatty fish (ie, salmon, mackerel), egg yolks, and fortified milk. Vitamin D is absorbed in the small intestine. Risk factors for vitamin D deficiency include inadequate exposure to sunlight, advanced age, more darkly pigmented skin, institutionalization, malabsorption or resection of the small intestine, hepatic or renal disease, and exclusive breast feeding of infants. Medications that induce the activity of hepatic cytochrome P450 enzymes (ie, phenytoin, phenobarbital, and rifampin) increase the catabolism of vitamin D.
Rickets, vitamin D deficiency in children, presents with frontal bossing, pectus carinatum, kyphosis, and bowing of the legs with delayed gross motor milestones. Vitamin D deficiency in adults results in osteomalacia (poor mineralization of the skeletal matrix) with periosteal bone pain, myalgias, and proximal muscle weakness. Although lower levels of vitamin D may increase the likelihood of the loss of periodontal attachment, vitamin D deficiency lacks other oral mucosal findings. Patients with hypervitaminosis D exhibit signs and symptoms of hypercalcemia.
Vitamin E (tocopherol)
Vitamin E is an antioxidant that prevents propagation of free radical damage to biologic membrane lipids. Vitamin E is found in a wide variety of dietary sources, notably oils and fats. Susceptible populations for vitamin E deficiency include premature infants and patients with fat malabsorption syndromes, impaired pancreatic or biliary secretion, lipid transport abnormalities, or genetic abnormalities of α-tocopherol transfer protein (α-TTP) (ie, ataxia with vitamin E deficiency, OMIM #277460). Vitamin E deficiency is rare and presents with peripheral neuropathy, muscle weakness, and cardiac arrhythmias. There are no oral manifestations of tocopherol deficiency.
Vitamin K (phylloquinone)
Vitamin K is an essential cofactor in the production of the procoagulant Factors II (prothrombin), VII, IX, and X, and the anticoagulant proteins, Protein C and Protein S. Vitamin K is found in significant amounts in green leafy vegetables (ie, collard greens, spinach, broccoli) and oils (ie, soybean, canola, olive). Vitamin K is absorbed predominantly in the terminal ileum. Risk factors for vitamin K deficiency include small bowel resection, chronic liver disease, cholestasis, lipid malabsorption, chronic illness, alcoholism, malnutrition, oral anticoagulant therapy (ie, warfarin, salicylates), or prolonged use of antibiotics. Newborns, especially those that are exclusively breast-fed, are also susceptible. The main clinical manifestation of vitamin K deficiency is bleeding, which can affect any site. Oral signs may include submucosal hemorrhage and gingival bleeding. Diagnostic testing reveals a low serum vitamin K level and prolonged prothrombin time. Asymptomatic vitamin K deficiency can be treated with oral phytonadione. Menadione, a synthetic, water-soluble form of vitamin K, is administered orally in patients with fat malabsorption. In more severe cases, intramuscular or subcutaneous vitamin K administration may be warranted.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


